Page 6 of 22
IM28.8-10 | Obstructive Airway Disease Clinical Evaluation — SDL Guide (Part 2)
Identifying Signs of Specific Conditions and Differential Diagnosis
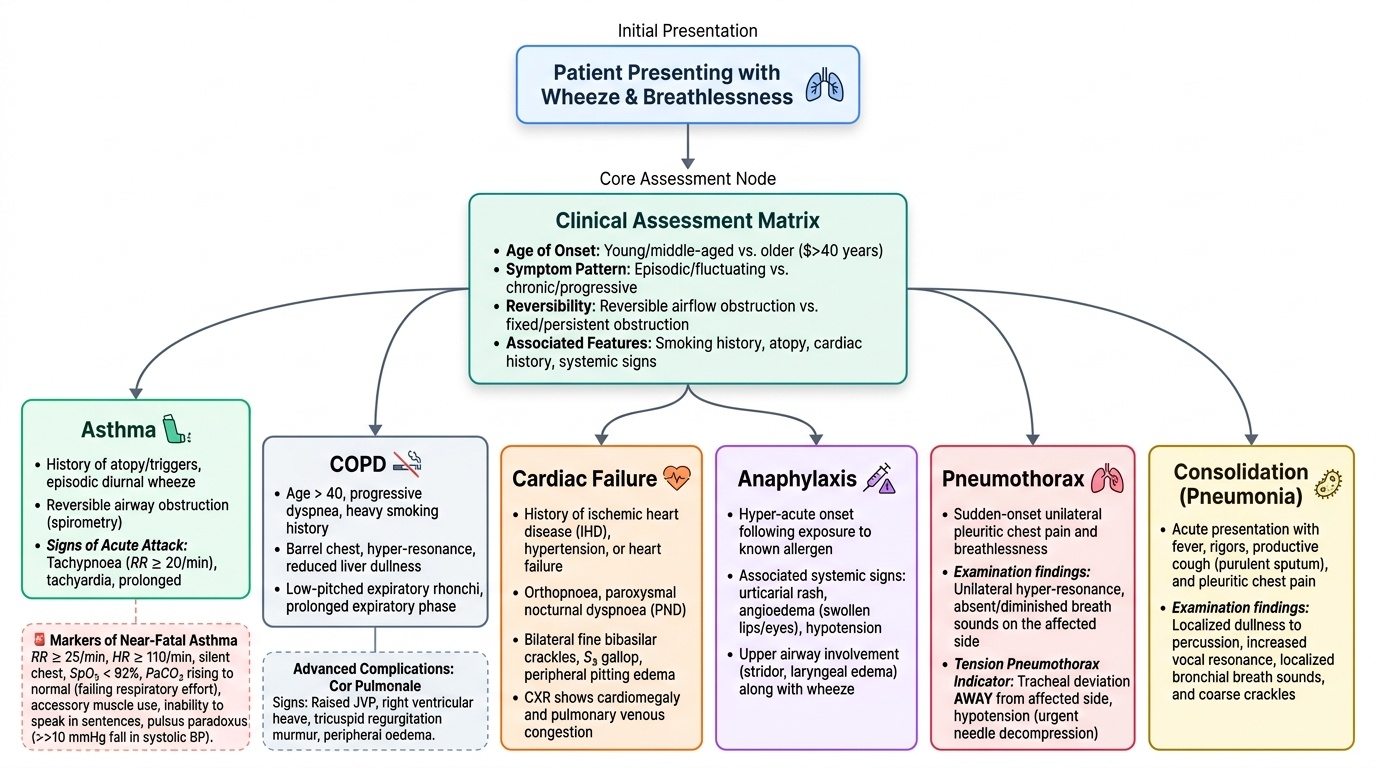
A central clinical skill is the ability to integrate the history and examination findings to distinguish obstructive airway disease from its major mimics, and to recognise the complications that modify the clinical picture. The differential diagnosis of wheeze and breathlessness extends beyond asthma and COPD, and generating a prioritised differential from clinical features is the core of NMC competency IM28.10.
Provided image
Signs specific to asthma (acute attack):
The acute asthmatic attack produces the triad of breathlessness, wheeze, and chest tightness. On examination: tachypnoea (RR ≥20/min), tachycardia, prolonged expiratory phase, diffuse expiratory (or biphasic) wheeze, reduced air entry in severe attacks. Markers of near-fatal asthma (requiring immediate intensive treatment): RR ≥25/min, HR ≥110/min, inability to complete a sentence in one breath, accessory muscle use, SpO₂ <92%, PaCO₂ rising toward normal (a rising PaCO₂ in asthma is paradoxically dangerous — it means the patient's respiratory effort is failing). Pulsus paradoxus (>10 mmHg fall in systolic BP on inspiration) reflects large swings in intrathoracic pressure from severe airway obstruction — it is measurable but less commonly formally assessed.
Signs specific to COPD:
In stable moderate-severe COPD: barrel chest, hyper-resonance, reduced liver dullness (diaphragm displaced downward), prolonged expiratory phase, low-pitched expiratory rhonchi (wheeze from large-airway secretions — different quality from asthma's high-pitched polyphonic wheeze), reduced air entry particularly at the bases. In advanced COPD with cor pulmonale: raised JVP, right ventricular heave, tricuspid regurgitation murmur, peripheral oedema. The combination of hypoxaemia, peripheral oedema, and elevated JVP with a large heart on CXR suggests cor pulmonale.
Identification of specific complications on examination:
Pneumothorax: unilateral hyper-resonance on percussion + absent or markedly reduced breath sounds on the affected side + tracheal deviation AWAY from the affected side (in tension pneumothorax). In COPD, a spontaneous pneumothorax can precipitate acute exacerbation — the clinical picture may mimic a severe exacerbation, but the unilateral nature and percussion findings distinguish it. A pneumothorax in COPD with emphysematous bullae is a surgical emergency.
Pleural effusion: stony dullness (markedly dull, more than consolidation) on percussion + absent breath sounds over the effusion + bronchial breathing just above the upper border of the effusion (at the fluid-lung interface) + reduced vocal fremitus and resonance. In COPD, a parapneumonic effusion complicating pneumonia is the commonest cause; malignant effusion should be considered in smokers with new effusion.
Consolidation (pneumonia complicating OAD): dullness on percussion + bronchial breathing (harsh, tubular, with equal inspiration and expiration, audible pause between) + increased vocal resonance and fremitus + coarse late inspiratory crackles in the affected area. Pneumonia is the commonest infective precipitant of COPD exacerbation requiring hospitalisation — its identification changes management (specific antibiotics, chest physiotherapy).
Differential diagnosis of wheeze and breathlessness — prioritised by clinical features:
| Clinical pattern | Most likely diagnosis | Key distinguishing feature |
|---|---|---|
| Episodic wheeze, nocturnal, triggers, young patient, atopy | Asthma | Reversible obstruction, diurnal variation, atopic history |
| Progressive dyspnoea, >40 yr, heavy smoker, daily sputum | COPD | Irreversible obstruction, smoking history, no symptom-free periods |
| Acute wheeze + urticaria + hypotension after allergen | Anaphylaxis | Systemic allergic reaction, shock, urticaria |
| Wheeze + bilateral crackles + orthopnoea + elevated JVP | Left ventricular failure ("cardiac asthma") | Raised JVP, S3 gallop, bilateral basal crepitations, response to diuretics not bronchodilators |
| Stridor (inspiratory) + hoarse voice + recent URTI | Croup or laryngeal oedema | Stridor is INSPIRATORY (large airway) — wheeze is expiratory (small airway obstruction) |
| Sudden onset breathlessness + unilateral hyper-resonance | Pneumothorax | Unilateral findings, absent breath sounds, tracheal deviation |
| Monophonic wheeze + haemoptysis + weight loss in smoker | Endobronchial tumour | Localised, fixed wheeze; chest radiograph shows a mass |
| Fever + productive cough + dullness + bronchial breathing | Pneumonia | Consolidation signs, fever, acute onset |
Prioritising the Differential Diagnosis of Wheeze
SELF-CHECK
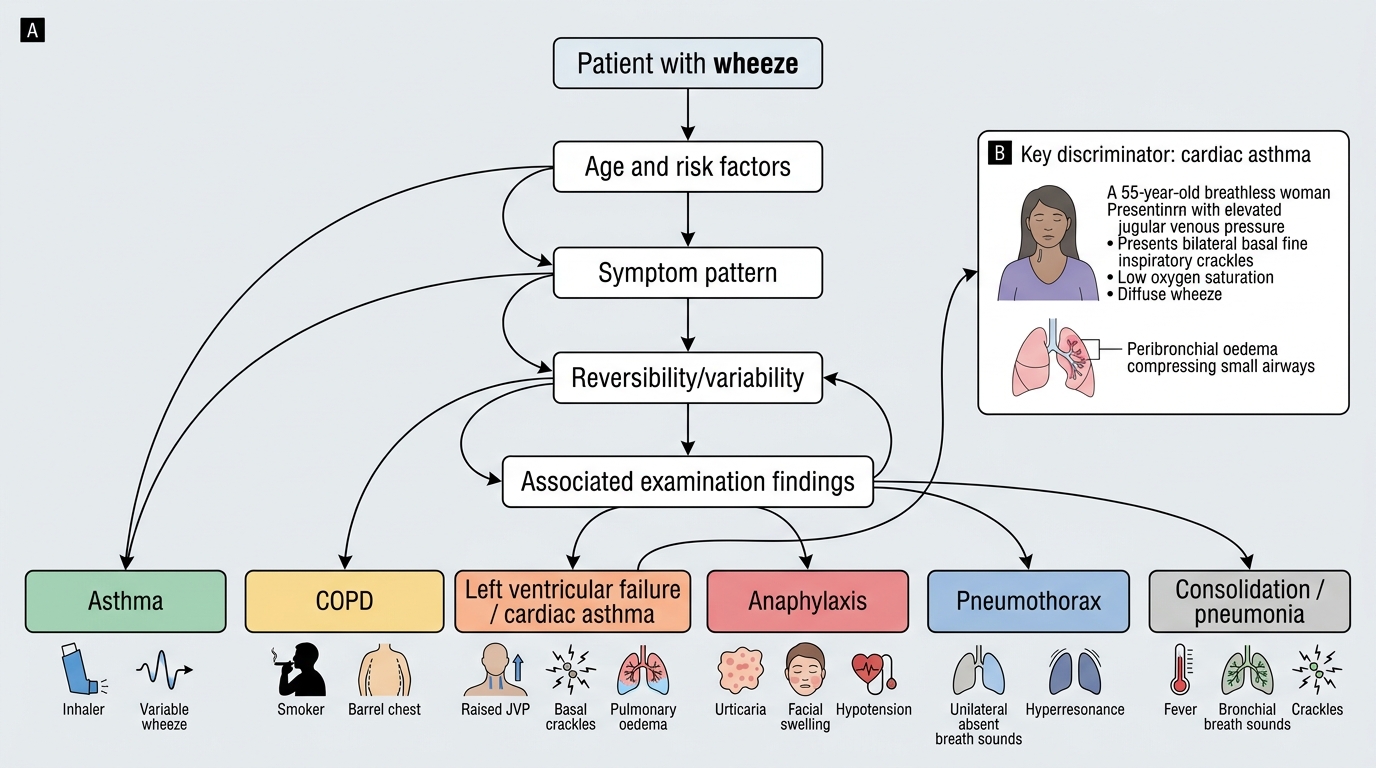
During examination of a 55-year-old breathless woman, you note: RR 24/min, SpO₂ 90%, elevated JVP at 4 cm above the sternal angle, bilateral basal fine inspiratory crackles, and a wheeze heard throughout both lungs. She has no smoking history and her symptoms began 2 days ago. What is the MOST likely diagnosis?
A. Acute severe asthma — wheeze is the dominant finding
B. COPD exacerbation — bilateral wheeze and dyspnoea
C. Left ventricular failure presenting with wheeze (cardiac asthma)
D. Bilateral pneumonia — crackles and wheeze coexist
Reveal Answer
Answer: C. Left ventricular failure presenting with wheeze (cardiac asthma)
The combination of wheeze (which in left ventricular failure arises from peribronchial oedema compressing small airways — 'cardiac asthma'), elevated JVP, bilateral fine basal inspiratory crackles (from alveolar flooding), acute onset, and no smoking history points strongly to left ventricular failure. In true asthma, JVP is not elevated and crackles are not a prominent finding. COPD would require a smoking history and a more gradual onset. The JVP elevation is the discriminating finding — it does not occur in asthma or COPD but is the cardinal sign of right and left heart failure. This distinction is critical because management differs completely: LVF requires diuretics, not bronchodilators (though bronchodilators may be added for the wheezing component).
Applied Practice: Documentation and Clinical Reasoning
Having established how to take the history and perform the examination, the third clinical skill is translating findings into a structured clinical presentation — the verbal or written summary that communicates findings to colleagues and guides management decisions. In the OSPE or clinical examination context, you will be expected to present the case in a logical sequence that mirrors your clinical reasoning: complaint → history → findings → interpretation → differential → most likely diagnosis → next investigation.
Provided image
A model presentation for a COPD patient might proceed as follows: 'Mr Rajan is a 58-year-old retired textile worker who presents with progressive exertional dyspnoea over 3 years and a daily productive cough for 5 years, with two exacerbations requiring hospitalisation in the past year. He has a 35 pack-year smoking history. On examination he is afebrile, tachypnoeic at 22/min, SpO₂ 91% on room air, using accessory muscles. He has a barrel chest, bilateral hyper-resonance, prolonged expiratory phase, and diffuse low-pitched expiratory rhonchi. The MRC dyspnoea grade is 3. There is mild peripheral oedema. My assessment is that this is most consistent with GOLD stage 2–3 COPD with a possible element of cor pulmonale. My immediate investigations would be pulse oximetry-guided ABG, peak flow or spirometry to document current FEV1, chest radiograph to exclude pneumothorax or pneumonia, and ECG to assess for right ventricular strain.' This presentation is compact, complete, and clinically actionable.
Clinical documentation requirements for obstructive airway disease:
- Smoking history in pack-years (documented numerically, not as 'heavy smoker')
- Exacerbation frequency in the past 12 months (number of courses of antibiotics, hospital admissions)
- Current medications and inhaler device types
- MRC dyspnoea grade (1–5)
- SpO₂ at rest on room air and on exertion
- Weight and BMI (low BMI in COPD = poor prognostic marker; obesity is relevant to sleep apnoea)
Recognising severity markers in the clinical evaluation:
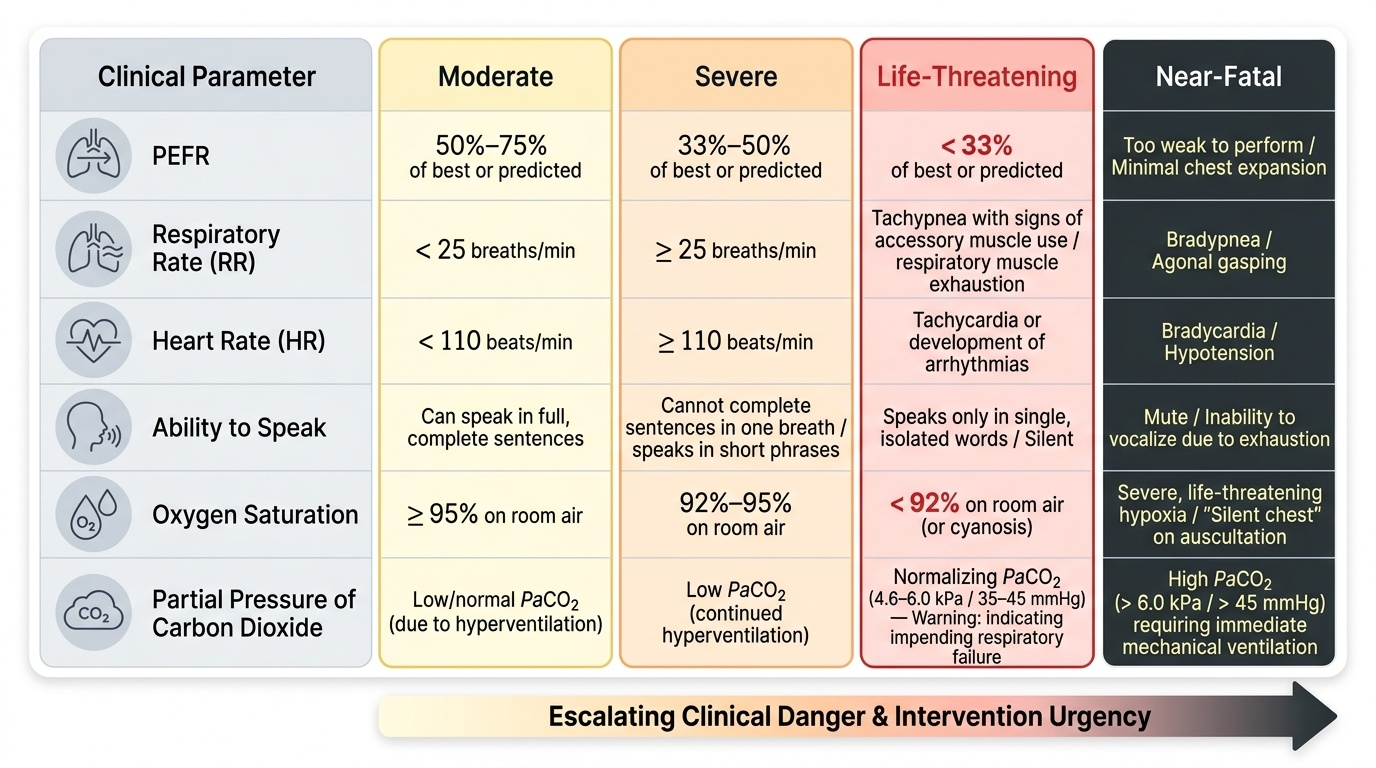
For acute asthma — the British Thoracic Society (BTS) / GINA classification:
- Moderate: PEFR 50–75% best, RR <25/min, HR <110/min, can speak in sentences
- Severe: PEFR 33–50% best, RR ≥25/min, HR ≥110/min, unable to complete sentences
- Life-threatening: PEFR <33%, SpO₂ <92%, PaO₂ <8 kPa, silent chest, cyanosis, feeble respiratory effort, bradycardia, exhaustion
- Near-fatal: rising PaCO₂ and/or requiring mechanical ventilation
For COPD exacerbations — severity based on clinical assessment:
- Mild: managed at home with increased bronchodilators
- Moderate: hospital assessment required, systemic steroids and antibiotics
- Severe: hospitalisation, ABG required, non-invasive ventilation if pH < 7.35 and PaCO₂ elevated
Acute Asthma Attack Severity Classification
SELF-CHECK
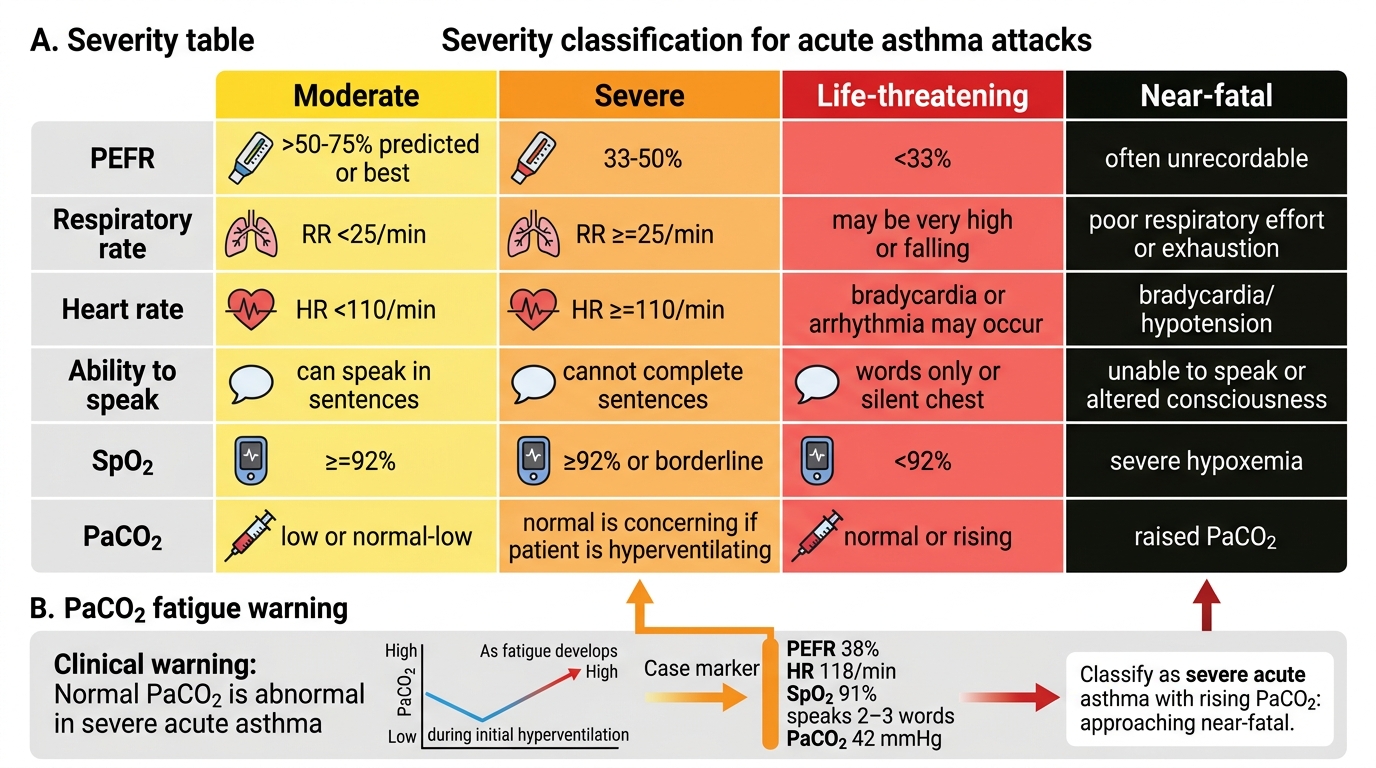
A 32-year-old asthmatic woman is brought to emergency with acute breathlessness. Her PEFR is 38% of predicted, RR 28/min, HR 118/min, SpO₂ 91%, and she can only speak two or three words at a time. Her ABG shows PaCO₂ 42 mmHg (upper limit of normal). How should this be classified?
A. Moderate acute asthma — PEFR above 33%
B. Severe acute asthma with a rising PaCO₂ — this is approaching near-fatal
C. Life-threatening asthma — PEFR <33%
D. Mild exacerbation — ABG is normal so ventilatory failure is not present
Reveal Answer
Answer: B. Severe acute asthma with a rising PaCO₂ — this is approaching near-fatal
PEFR 38% (between 33–50%) + RR ≥25/min + HR ≥110/min + inability to complete sentences = severe acute asthma by BTS/GINA criteria. However, the PaCO₂ of 42 mmHg is critically important: in a hyperventilating asthmatic (as expected with RR 28/min and severe airway obstruction), PaCO₂ should be LOW (25–35 mmHg) due to the increased ventilatory drive. A 'normal' PaCO₂ of 42 mmHg in this context is actually a sign of ventilatory FATIGUE — the respiratory muscles can no longer sustain the compensatory hyperventilation, and PaCO₂ is rising back toward normal. This is a near-fatal indicator and should trigger immediate escalation to ICU level care and preparation for NIV or intubation.
CLINICAL PEARL
Two examination traps that every final-year student must know: First, absence of wheeze does not mean absence of obstruction — wheeze requires sufficient airflow velocity to generate the vibrating sound; in a very severe attack ('silent chest'), airflow is so reduced that no wheeze is audible. A silent chest in a breathless, distressed patient is a medical emergency, not reassurance. Second, a normal PaCO₂ in a breathless asthmatic is not normal — in acute asthma with hyperventilation, PaCO₂ should be suppressed (25–35 mmHg). A PaCO₂ that is 'normal' (38–42 mmHg) in this context signals ventilatory fatigue and impending respiratory failure. Always interpret the ABG in the context of the clinical state.
Self-Assessment: Clinical Evaluation Scenarios
Test your ability to apply history, examination, and differential diagnosis skills through the following structured clinical scenarios. For each, formulate a diagnosis and identify the key clinical feature that clinches it.
Scenario A: A 26-year-old medical student presents to the student health clinic with a 3-month history of episodic wheeze and breathlessness. Symptoms occur mainly at night and on waking, improve by 10 AM, and worsen with exercise and during the cold season. She has eczema and her mother has allergic rhinitis. Examination today (a weekday afternoon, several hours after a mild episode this morning) is entirely normal — no wheeze, normal air entry, RR 16/min, SpO₂ 99%. What is your differential and most likely diagnosis?
Analysis: Episodic symptoms, nocturnal pattern, diurnal variation, triggers (exercise, cold), atopic background (eczema, family history of atopy), and complete resolution between episodes — all strongly favour allergic asthma. The normal examination between episodes is entirely consistent with asthma (inter-attack normalcy is a defining feature). Differential includes exercise-induced laryngeal obstruction (EILO — inspiratory rather than expiratory symptoms, no diurnal pattern) and vocal cord dysfunction. Confirm with spirometry (pre- and post-bronchodilator) and, if normal, bronchial provocation challenge (methacholine or exercise challenge).
Scenario B: A 70-year-old ex-miner presents with bilateral wheeze, raised JVP 6 cm above the sternal angle, bilateral ankle oedema to the knee, and fine inspiratory crackles at both bases. He stopped smoking 10 years ago after a 40 pack-year history. He has had a cough for years, but the breathlessness and ankle swelling have worsened over the past 6 weeks. What is the most important differential at this point, and what single examination finding distinguishes it from pure COPD exacerbation?
Analysis: The combination of wheeze (airway disease), elevated JVP (right or left heart failure), ankle oedema (right heart failure / cor pulmonale or biventricular failure), and bilateral crackles (either airway secretions in COPD or pulmonary oedema in cardiac failure) creates a complex picture. The raised JVP is the key distinguishing finding — it does not occur in uncomplicated COPD exacerbation (unless cor pulmonale is present, in which case it is a COPD complication, not a separate diagnosis). The most important differential is left ventricular failure (or biventricular failure), which would require a chest radiograph (cardiomegaly, upper-lobe diversion, septal lines), echocardiogram, and NT-proBNP measurement to confirm. Management pivots entirely if cardiac failure is the primary driver.
Scenario C: A 45-year-old woman is admitted with sudden-onset severe breathlessness after a COPD exacerbation. She was on 4 L/min oxygen via nasal cannula and then suddenly became very breathless. On examination: RR 32/min, SpO₂ 85%, trachea deviated to the RIGHT, LEFT side of chest is hyper-resonant on percussion with absent breath sounds. What is the diagnosis and the immediate management?
Analysis: Left-sided tension pneumothorax — the sudden worsening, tracheal deviation AWAY from the affected left side, unilateral hyper-resonance, and absent left breath sounds are pathognomonic. In COPD with emphysematous bullae, a spontaneous pneumothorax is a recognised complication and can be precipitated by high-flow oxygen or ventilator pressures. Immediate management: do NOT wait for a chest radiograph. Perform emergency needle decompression (second intercostal space, mid-clavicular line, left side) followed immediately by intercostal drain insertion. This is a clinical diagnosis requiring immediate action.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
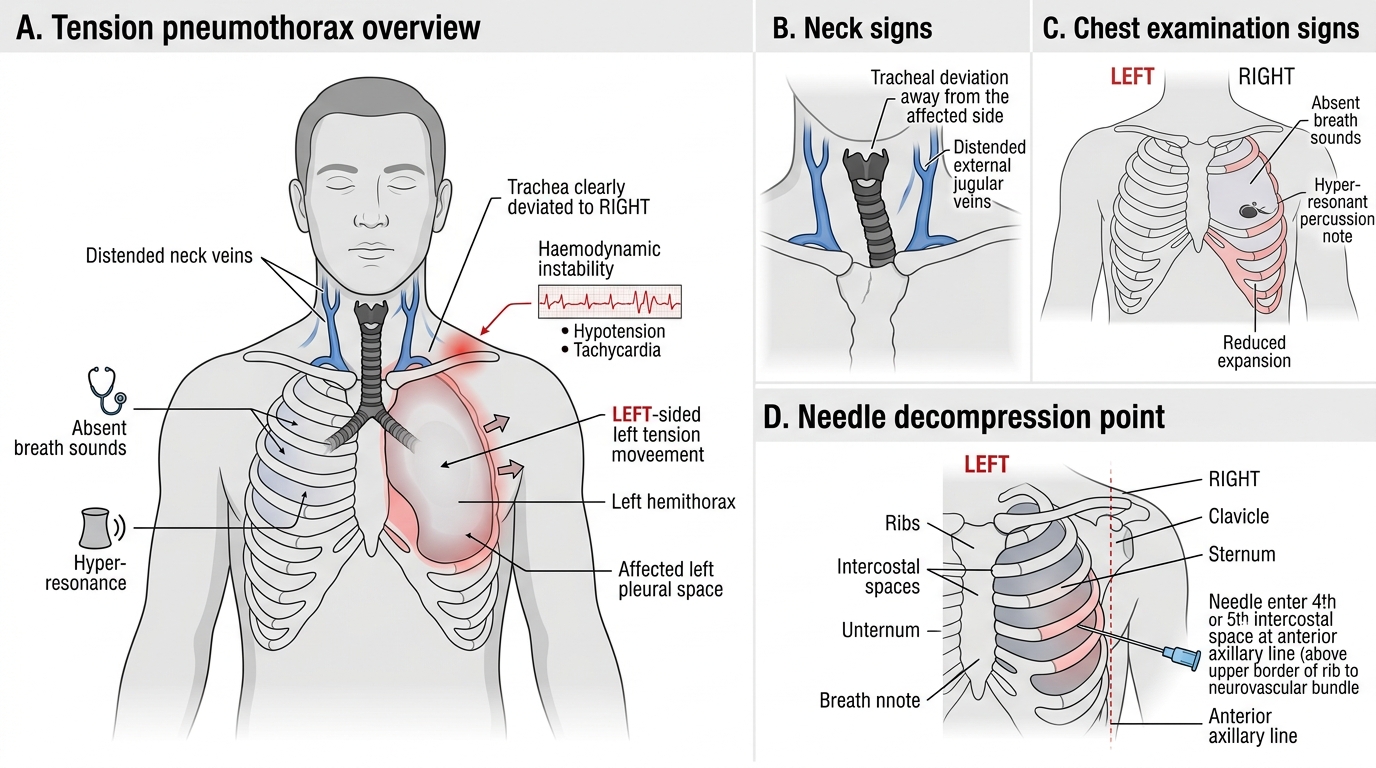
Clinical Signs and Emergency Decompression in Tension Pneumothorax