Page 13 of 20
IM29.{24,26} | Impaired Physicians and Research Consent — SDL Guide
Learning Objectives
- Define physician impairment and identify its principal causes including substance use disorders, mental health conditions, physical illness, and systemic factors (IM29.24)
- Discuss the medico-legal, ethical, and professional obligations that apply when dealing with an impaired physician — whether as a colleague, supervisor, or the impaired physician themselves (IM29.24)
- Describe the Indian regulatory framework governing impaired physicians under the NMC Act 2020 and the Mental Healthcare Act 2017 (IM29.24)
- Demonstrate the ability to administer informed consent to a patient being enrolled in a research protocol in a simulated environment (IM29.26)
- Apply the ICMR Guidelines 2017/2023 and Good Clinical Practice principles for research participant consent including vulnerable populations
INSTRUCTIONS
Two of the most professionally charged scenarios a clinician encounters are the discovery that a colleague's impairment is affecting patient safety, and the responsibility to enrol a patient into a research protocol with genuinely valid consent. Both scenarios require ethical clarity, legal literacy, and practical communication skill. This module develops the frameworks and simulation-based practice needed to handle both.
References
- ICMR National Ethical Guidelines for Biomedical and Health Research Involving Human Participants, 2017 (updated 2023) (guideline)
- NMC Act 2020 — professional conduct and disciplinary provisions (legal)
- Mental Healthcare Act 2017 — provisions applicable to healthcare professionals with mental health conditions (legal)
- Harrison's Principles of Internal Medicine, 21st ed., Chapter 4 — Ethical Issues in Clinical Medicine (textbook)
- Declaration of Helsinki 2013 — ethical principles for medical research (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two scenarios. In the first: you are a junior registrar on the neurology ward. Your senior, Dr. Kapoor, has been noticeably unwell for the past three weeks — his hands shake in the morning, his clinical decisions have been inconsistent, and last week a nurse told you she smelled alcohol on his breath on a Tuesday afternoon. He has not been to the mandatory morning conference in ten days. Today he prescribed valproate for a patient without checking the pregnancy status — the patient is 14 weeks pregnant. You said nothing. In the second scenario: you are on the research team of a clinical trial studying a new antiplatelet agent. A 68-year-old farmer with limited literacy has been identified as a potential participant. He has been told the details in Hindi by a research assistant. He nods when asked if he understands. The principal investigator asks you to get his signature on the consent form before the next clinic. You have not personally spoken to the patient. You are unsure he truly understands. Both scenarios have something in common: they present a gap between what appears to be happening and what is ethically and legally required. This module develops the professional clarity to act in both.
WHY THIS MATTERS
Impaired physician management (IM29.24) and research consent administration (IM29.26) are placed at the Knowledge (K) and Skill/Habit (SH) levels respectively in the NMC 2024 curriculum — indicating that the former requires the ability to reason through medico-legal and ethical dimensions, while the latter requires demonstrated performance in a simulated environment. Both competencies address professional scenarios that are genuinely high-stakes: a failure to address an impaired colleague can result in patient harm that is foreseeable and therefore legally attributable to those who remained silent; an inadequate research consent process can expose participants to risks they never truly understood and can render an entire trial's data ethically invalid. In India, both areas are governed by explicit regulatory frameworks that the final-year student must know — the NMC Act 2020 and Mental Healthcare Act 2017 for impaired physicians, and the ICMR Guidelines 2017/2023 and GCP Guidelines for research consent.
RECALL
Before proceeding, activate your prior knowledge. From your ethics module (SDL: Principles of Medical Ethics), recall the concept of beneficence — acting in the patient's best interest — and its relationship to non-maleficence — the duty to prevent harm. Ask yourself: if a colleague is impaired and potentially harmful to patients, what does beneficence require of the physician who knows? From your pharmacology training, recall the concept of informed consent for clinical treatment — the five elements (disclosure, understanding, voluntariness, capacity, decision). Now extrapolate: what additional obligations apply when the procedure is for research rather than direct therapeutic benefit, and when the participant is a vulnerable or illiterate individual? These two prior knowledge pillars — ethical principles and consent theory — are the foundation on which this module builds its applied frameworks.
Physician Impairment: Definitions, Causes, and Magnitude
Physician impairment refers to a condition in which a registered medical practitioner's ability to practise medicine safely and competently is compromised by any of a range of physical, psychological, or substance-use related conditions. The definition used by most medical councils — including the frameworks being adopted under the NMC Act 2020 — is functional rather than diagnostic: impairment is present when the physician's condition affects their clinical performance in a way that creates or could create risk for patients, regardless of the specific cause.
Provided image
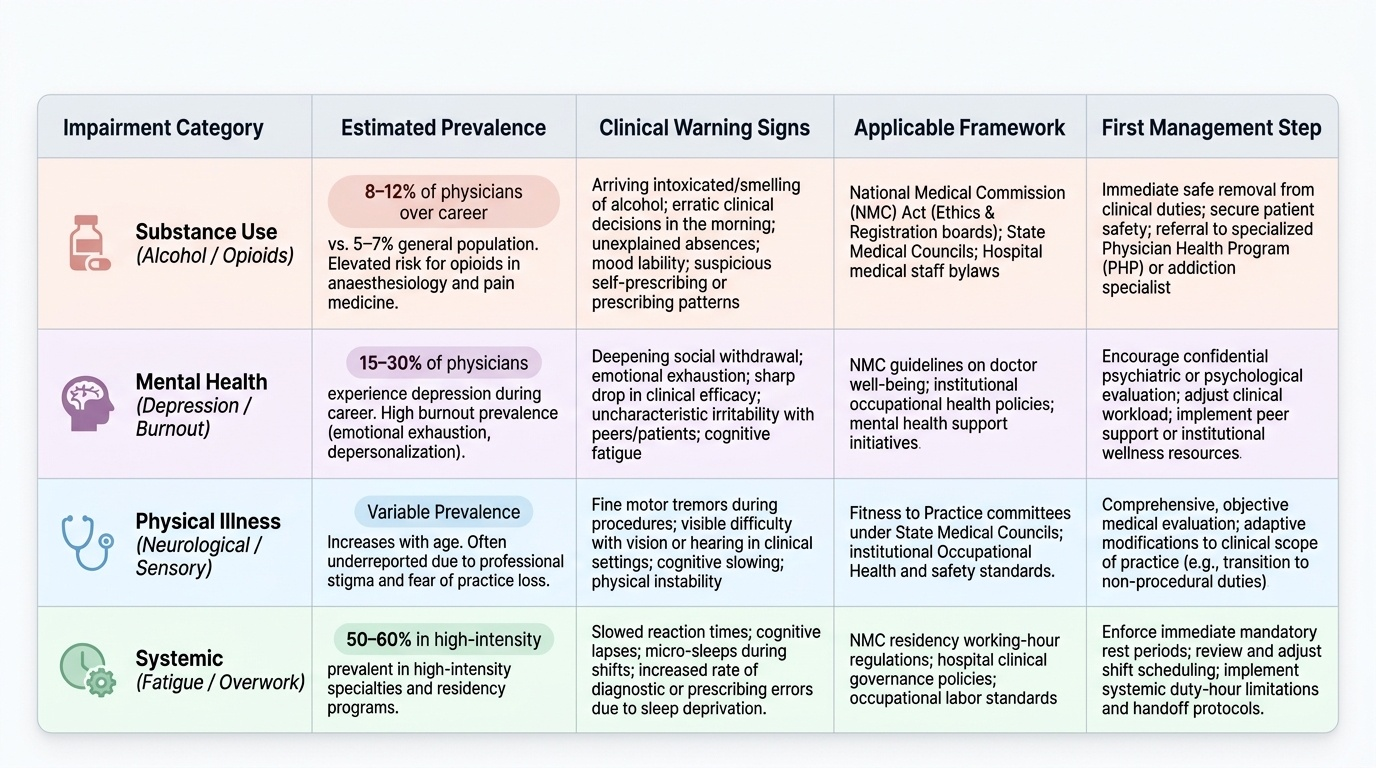
The principal categories of physician impairment and their relative prevalence in medical literature (primarily from Indian and international data on healthcare worker health) are:
Substance use disorders are the most publicly discussed cause of physician impairment. Alcohol use disorder is estimated to affect 8–12% of physicians over a career, compared with 5–7% in the general population — an elevation that reflects specific occupational risk factors including access to controlled substances, professional stress, self-prescribing culture, and the professional culture that normalises excessive drinking as a coping behaviour. Opioid use disorder is a particular risk in anaesthesiology and pain medicine, where healthcare workers have direct access to potent opioids. The clinical signature of substance-related impairment includes: arriving at work appearing intoxicated or smelling of alcohol, inconsistent or erratic clinical decisions particularly in the morning hours (consistent with morning alcohol or metabolite effects), unexplained absences, mood lability, and in some cases requests for controlled substance prescriptions for named patients that the prescribing doctor has not recently examined.
Mental health conditions are the most prevalent but least visible cause of physician impairment. Depression affects an estimated 15–30% of physicians during their career — a rate substantially higher than the general population, driven by occupational factors including high-stakes responsibility, continuous exposure to suffering and death, poor work-life balance, and limited help-seeking behaviour in a professional culture that stigmatises mental health conditions. Burnout — characterised by emotional exhaustion, depersonalisation, and reduced efficacy — is not a psychiatric diagnosis but produces functional impairment qualitatively similar to major depressive disorder. An important and underappreciated point: burnout and depression frequently co-occur and are clinically difficult to distinguish without formal assessment. Both can impair clinical judgment, reduce attention to detail, and produce the emotional blunting that is particularly dangerous in high-stakes clinical encounters.
Physical illness — including neurological conditions (early dementia, post-stroke cognitive impairment, Parkinson disease), severe musculoskeletal disease, uncontrolled diabetes, or major visual or hearing impairment — can produce impairment that the physician themselves may not accurately perceive due to the well-documented phenomenon of anosognosia (impaired awareness of one's own deficits) that accompanies many neurological and some psychiatric conditions.
Systemic factors are often the primary driver: extreme fatigue from excessive working hours, inadequate sleep, chronic stress without adequate support, and the absence of occupational health systems that allow physicians to seek help without risking their registration. The WHO and NMC both recognise that physician impairment is not solely an individual failure — it is a systems problem that requires institutional-level response.
The magnitude of the problem in India is substantial. A 2019 survey of over 2,000 Indian medical professionals (published in the Indian Journal of Psychiatry) found that over 30% met criteria for probable depressive episode and over 60% reported symptoms of burnout. Alcohol consumption was reported at harmful levels by approximately 15% of male physicians surveyed. Against this backdrop, the probability that any practising Indian physician will encounter an impaired colleague during their career is very high — which is precisely why IM29.24 is a curriculum competency.
Medico-Legal and Ethical Obligations When Dealing with an Impaired Physician
The ethical and legal obligations that arise when a clinician becomes aware of a colleague's impairment are among the most professionally challenging in medicine — because they create a direct conflict between collegial loyalty (protect the colleague, enable recovery without public disclosure) and patient protection (prevent harm to patients who may be exposed to the impaired clinician's care). The resolution of this conflict is clearly established in both the ethical and legal frameworks, but acting on that resolution requires professional courage.
Provided image
The ethical framework applies the four principles as follows: non-maleficence (prevent harm to patients currently and prospectively in the impaired physician's care) and beneficence for the patient both support timely action to restrict the impaired physician's clinical activities. Beneficence for the physician supports a response that is supportive, confidential, and recovery-oriented rather than punitive — recognising that impairment is frequently a manifestation of occupational illness rather than moral failure. Autonomy supports the impaired physician's right to participate in their own rehabilitation programme and to be treated with dignity throughout the process. Justice requires that the response be consistent — applied to all impaired physicians regardless of seniority, specialty prestige, or institutional politics.
The legal framework under the NMC Act 2020 establishes that the NMC has the authority to investigate professional misconduct and to impose conditions on, suspend, or remove from the register any practitioner whose fitness to practise is impaired. The NMC's approach to impaired physicians, as articulated in the amended Code (2023), reflects the international shift toward a fitness to practise model rather than a purely punitive model: the goal is to identify impairment early, facilitate treatment and recovery, and return the physician to safe practice where possible — rather than automatically ending careers for conditions that are treatable. However, the fitness to practise model does not reduce the obligation to report: a medical professional who has reasonable grounds to believe that a colleague's impairment is creating patient risk is obligated to act. Remaining silent while aware of ongoing patient risk is itself professionally and potentially legally culpable under the NMC Act.
The Mental Healthcare Act 2017 (MHCA) is relevant because it governs the treatment of individuals with mental health conditions, including physicians. Key provisions: (a) every person has the right to access mental health treatment and is entitled to the same standard of care for mental illness as for physical illness; (b) no person shall be treated for a mental illness against their will except under specified involuntary treatment provisions; (c) discrimination on grounds of mental illness in employment — including medical practice — is prohibited; (d) the MHCA specifically protects physicians from the threat of registration loss solely on grounds of having received mental health treatment, provided they are under appropriate care and their fitness to practise is confirmed. This last provision is critically important: it means a physician who voluntarily seeks treatment for depression or alcohol dependence and is in a structured recovery programme cannot automatically be struck off the register; their fitness to practise must be assessed by a medical board with appropriate expertise.
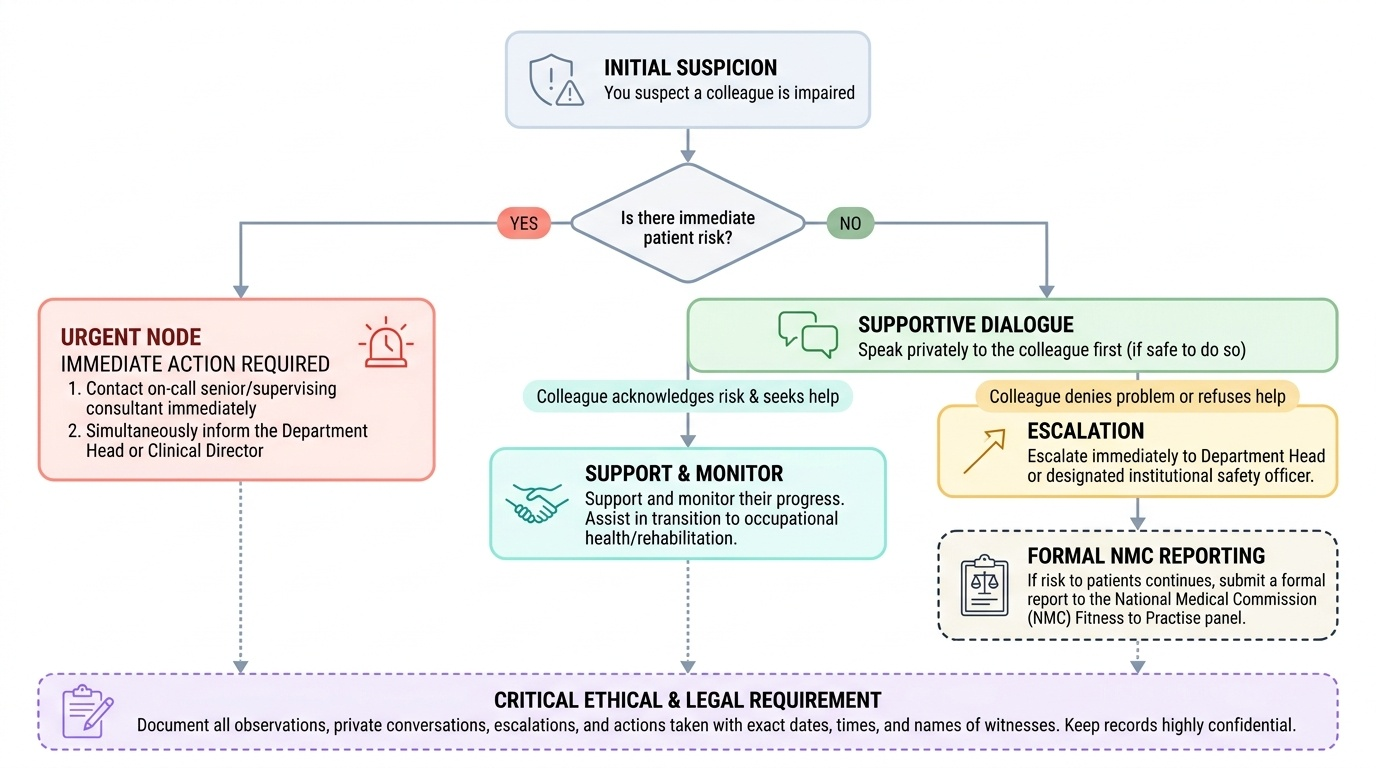
The step-by-step professional response to a suspected impaired colleague:
- Document observations: record specific, objective, dated observations — not impressions or rumours ('smelled of alcohol at 3 PM on 12 June' rather than 'he drinks')
- Assess immediate patient risk: if a patient is currently at risk because of the impaired physician's direct clinical involvement, escalate to the on-call supervising consultant and clinical director immediately — patient safety takes priority over any other consideration
- Speak to the colleague directly (if safe and the risk is not immediate): a private, non-confrontational conversation expressing concern for their wellbeing, describing specific observed behaviours, and encouraging them to seek occupational health or medical help. This conversation should be documented.
- Escalate if the colleague does not respond: if the direct conversation produces no change in behaviour or if the colleague denies and continues to work, the obligation shifts to formal escalation — to the department head, the medical director, or the institution's clinical governance officer
- Report to the NMC (as a last resort if institutional escalation fails): the NMC has a statutory duty to receive fitness to practise concerns; the reporting clinician is protected from retaliation under NMC procedures provided the report is made in good faith
- Support recovery: when the impaired physician has been withdrawn from clinical duties and is receiving appropriate treatment, the role of the clinical team is supportive — facilitated return to practice through a structured programme, phased re-entry, and ongoing supervision
The hardest scenario is when the impaired physician is a senior colleague or direct supervisor. The same obligations apply, but the practical pathway is different: it is not appropriate for a junior clinician to attempt a direct confrontation with a senior consultant; the correct escalation path is to the head of the department or to the clinical director, bypassing the immediate supervisor if necessary. The NMC Code makes clear that professional hierarchy does not override the duty to protect patients.
SELF-CHECK
Dr. Arun, a consultant physician, has been showing signs of possible impairment over the past two months — his clinical decisions are inconsistent, he appears fatigued and irritable, and a senior nurse has mentioned she thought she smelled alcohol on his breath twice. He is not under direct supervision. You are a junior registrar. He is about to see a patient with an acute myocardial infarction unsupervised. What is the MOST appropriate immediate action?
A. Document your concerns in the patient's case record and wait to see if an error occurs
B. Speak privately to Dr. Arun after his clinic ends today to express your concern
C. Contact the on-call medical director or clinical director immediately to report a potential immediate patient risk, and ensure a competent clinician sees the AMI patient
D. Report directly to the NMC online portal — the situation warrants immediate formal reporting
Reveal Answer
Answer: C. Contact the on-call medical director or clinical director immediately to report a potential immediate patient risk, and ensure a competent clinician sees the AMI patient
The patient with an acute myocardial infarction is in immediate clinical risk if seen by a potentially impaired clinician without competent supervision. In a situation of immediate patient risk, the correct action is to contact the on-call supervisor, clinical director, or medical director immediately — bypassing normal professional hierarchies — to ensure patient safety. This takes priority over everything else, including the more considered approach of a private conversation with Dr. Arun. Documenting and waiting (option A) leaves the immediate patient at risk. Speaking to Dr. Arun after clinic (option B) is the appropriate approach for non-immediate concerns but not when a patient with an AMI is about to be seen. Directly reporting to the NMC (option D) is appropriate only after institutional mechanisms have been exhausted — the NMC is not an emergency response body.
Administering Research Consent: Principles and Practice
Research consent administration (IM29.26) is designated at the Skill/Habit (SH) level in the NMC curriculum — meaning the final-year student is expected to be able to perform this in a simulated environment, not merely describe it. The scenario-based nature of the competency reflects its critical importance: inadequate research consent is one of the most common and most consequential ethical failures in clinical research, with direct consequences for participant safety, scientific validity, and institutional credibility.
The distinction between therapeutic consent and research consent is fundamental and must be clearly understood before proceeding to the practical skill. In clinical practice, consent is obtained for a procedure or treatment that is intended to benefit the individual patient. In research, consent is obtained for participation in a study whose primary purpose is to generate generalisable knowledge — the participant may benefit, but the benefit is not guaranteed, and they are being asked to accept risks or burdens (additional blood draws, investigational drugs, follow-up visits) in the service of science. This distinction creates an asymmetry: the research participant is entitled to a higher standard of disclosure than the clinical patient, because they are being asked to accept burdens for the benefit of others, not primarily for their own benefit. This higher standard is embedded in the ICMR National Ethical Guidelines for Biomedical and Health Research Involving Human Participants 2017 (updated 2023), which is the primary Indian regulatory document governing research consent.
The elements of valid research consent under ICMR Guidelines and aligned with the GCP (Good Clinical Practice) framework include the following, which must be communicated clearly to the participant before any study-related procedures begin:
- Explanation that this is research, not standard treatment — many participants in India conflate research participation with receiving the best available medical care; this misunderstanding (called therapeutic misconception) must be explicitly corrected
- Description of the study purpose — in non-technical language appropriate to the participant's literacy and background
- Description of all study procedures — including which are experimental and which are standard clinical care
- Foreseeable risks and discomforts — both from the investigational intervention and from any study-specific procedures
- Anticipated benefits — to the participant (if any) and to society; if there is no direct benefit to the participant, this must be stated clearly
- Disclosure of alternative treatments or procedures — participants must know what care they would receive outside the trial
- Confidentiality of records — how the participant's data will be protected, who will have access, and any limits to confidentiality
- Compensation and treatment for injury — participants must be informed of arrangements for compensation or treatment if study-related harm occurs (Indian GCP requires that study sponsors provide free treatment for research-related injury)
- Voluntariness and the right to withdraw — participation is voluntary; the participant can withdraw at any time without affecting their access to standard clinical care; no penalty or loss of benefits will result from withdrawal
- Contact information — who to contact for questions about the study and for research-related injuries; the name and contact of the IEC Chair for independent concerns
The consent process is a conversation, not a form-signing event. The ICMR Guidelines explicitly state that the consent process must include adequate time for the participant to ask questions, and that the participant's comprehension of the key elements must be assessed before the consent document is signed. Common errors in research consent practice that the final-year student must recognise and avoid:
- Handing the consent form to a participant without personally explaining the study
- Allowing a research assistant (non-physician) to conduct the consent process for studies involving medical procedures
- Failing to assess comprehension — asking 'Do you understand?' and accepting a head nod as adequate
- Obtaining consent immediately before a study procedure begins, giving the participant no time to reflect or consult family
- Not documenting the consent conversation in the participant's research file
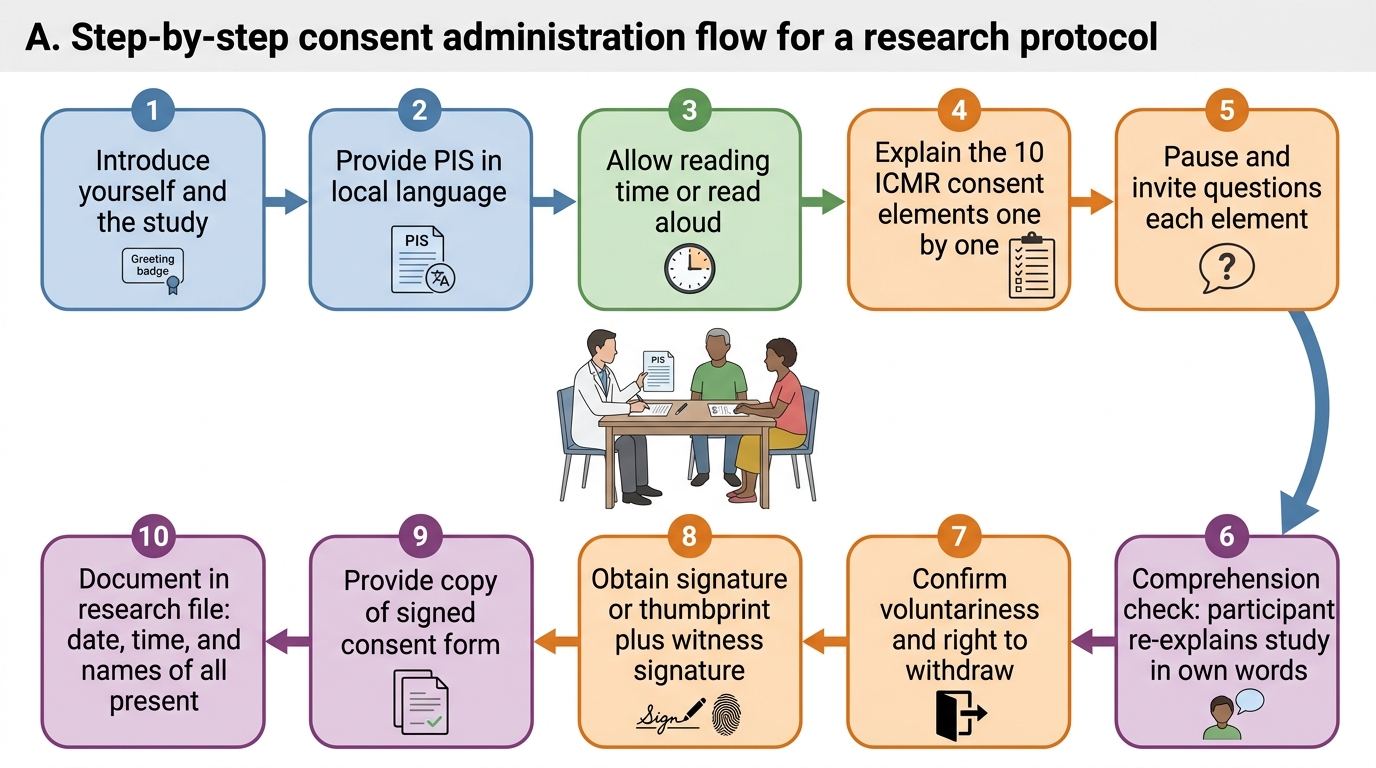
Consent Administration Flow for a Research Protocol