Page 4 of 20
IM29.{8-10,12-14,21,25} | Professional Conduct and Documentation — SDL Guide
Learning Objectives
- Demonstrate professional conduct when working in a healthcare team including respect for hierarchy and peers (IM29.8)
- Apply standards of patient privacy and confidentiality in everyday clinical practice (IM29.9, IM29.10)
- Describe and follow the principles of accurate medical record documentation including correct medicolegal use of case records (IM29.13)
- Demonstrate responsibility, work ethics, and altruism within the healthcare team and toward patients (IM29.12, IM29.25)
- Apply risk management and medical error reduction practices in clinical settings (IM29.21)
- Maintain appropriate professional grooming and presence in clinical environments (IM29.14)
INSTRUCTIONS
Professional conduct is the visible expression of the values that underpin good medical practice. This module develops the skills and attitudes required to function effectively and ethically within a healthcare team — from the precision of medical record documentation to the culture of patient safety. These are not abstract ideals but daily habits that determine the quality of care your patients receive and the trustworthiness of the institutions in which you work.
References
- NMC Code of Professional Conduct, Etiquette and Ethics Regulations 2002 (amended 2023) (guideline)
- Consumer Protection Act 2019 — medical services as consumer services (legal)
- Harrison's Principles of Internal Medicine, 21st ed., Chapter 4 — Ethical Issues in Clinical Medicine (textbook)
- World Health Organization: Patient Safety Curriculum Guide, 2011 (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr. Anand, a junior resident, is handed a case note from the morning round. The nurse has written: 'Patient complained of chest pain. Dr. A examined. Said it was okay.' A few hours later, the patient deteriorates — it was a STEMI. In the emergency, no one can find the ECG that was reportedly done. No drug doses or timing are recorded. The senior resident calls radiology to review a CT scan — only to find it had been requested under a completely different patient's name. Dr. Anand's morning examination is not documented anywhere. When the patient's family asks what happened, no one can reconstruct the timeline with confidence. Later, the Resident's Medical Officer is reviewing the record for a medico-legal complaint. The case note provides no legal protection — not because the care was bad, but because there is no record that it happened at all. Professional conduct is not just about being polite or working hard. It is about the habits of precision, accountability, and documentation that make healthcare safe — and that protect patients and clinicians alike.
WHY THIS MATTERS
As a final-year MBBS student rotating through medicine wards, you are already a functioning member of the healthcare team — you write case notes, take histories, assist in procedures, and interact with patients and families daily. The professional habits you establish now will persist through your entire career. The NMC 2024 curriculum (IM29.8–IM29.25) expects not merely knowledge of professional standards but demonstrated competency in applying them — at the Skill/Habit (SH) level. This means the examiner will not just ask you what goes in a case note; they will watch you write one, or ask you to respond to a scenario where documentation was deficient. In the Indian medico-legal landscape, a properly maintained case record is your primary legal protection under the Consumer Protection Act 2019 and before an NMC disciplinary committee. The quality of your documentation directly correlates with the quality of the care the next clinician can provide — and with your ability to defend that care if it is ever questioned.
RECALL
Activate your prior knowledge before proceeding. From your first year, recall the concept of medical negligence in Indian law — the three elements (duty of care, breach of that duty, and resulting damage). From your clinical years, recall the structure of a standard case note (history, examination, investigations, assessment, plan). From your community medicine posting, recall the principle of patient confidentiality and the concept of notifiable diseases. From your pharmacology and clinical training, recall the importance of accurate drug documentation — generic name, dose, route, frequency, and duration. Think now about the last case note you wrote or observed being written. Was every drug dose clearly recorded? Were the names of the two doctors on the ward round both legible in the record? If a colleague read it the next morning, would they be able to reconstruct exactly what was done and decided? These are the questions professional documentation answers.
Orientation: What Professional Conduct Means in Clinical Medicine
Professional conduct in clinical medicine refers to the constellation of behaviours, habits, and attitudes that reflect the norms of the medical profession — norms that exist not arbitrarily but because they directly govern the safety of patients and the functioning of healthcare teams. The NMC Code of Professional Conduct, Etiquette and Ethics Regulations 2002 (amended 2023) provides the formal regulatory standard, but professional conduct in practice is experienced as a set of daily habits: how you greet a patient, how you document a clinical finding, how you hand over information to a colleague, and how you respond when a mistake is made.
The reason professional conduct deserves systematic study — rather than being left to osmosis during clinical training — is that the research on clinical errors shows a striking pattern: the majority of adverse events in hospital care do not result from insufficient technical knowledge. They result from failures of communication, documentation, team function, and the institutional culture that normalises cutting corners. The WHO Patient Safety Curriculum Guide (2011) estimates that at least one in ten hospital admissions is associated with an adverse event, and that up to 50% of these events are preventable with systematic changes in professional behaviour. In India, a 2019 study published in the Journal of Patient Safety estimated that preventable adverse events contribute to over 5 million deaths annually across low- and middle-income countries — a burden that dwarfs the death toll from many communicable diseases. Understanding professional conduct is therefore a patient safety imperative, not a formality.
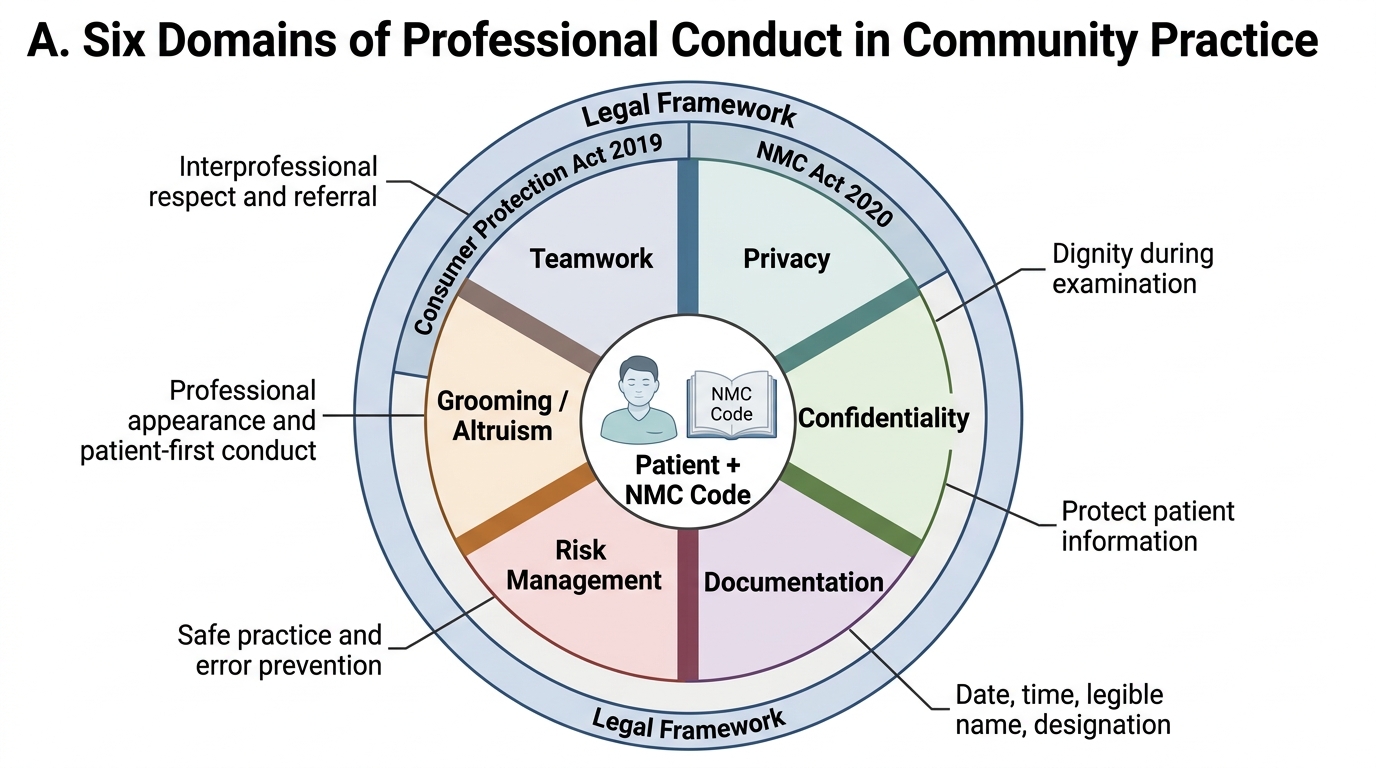
The scope of IM29.8–IM29.25 competencies covers six domains of professional behaviour that final-year students must demonstrate:
1. Teamwork (IM29.8): working effectively with peers and superiors, contributing constructively, communicating clearly across professional hierarchies
2. Privacy and confidentiality (IM29.9, IM29.10): protecting patient information in all clinical interactions, both physical and digital
3. Responsibility and work ethics (IM29.12): reliability, punctuality, honesty about clinical uncertainty, and ownership of tasks
4. Medical record documentation (IM29.13): accurate, complete, timely, and legible case records
5. Grooming and professional presence (IM29.14): the physical presentation expected in clinical environments
6. Risk management and error reduction (IM29.21) and altruism (IM29.25): the systemic and personal dimensions of a culture of safety and service
Each domain has both an ethical dimension (it is the right thing to do) and a legal dimension (failure to meet the standard may constitute professional misconduct under the NMC Act 2020, negligence under Indian tort law, or a deficiency of service under the Consumer Protection Act 2019).
Six Domains of Professional Conduct
Medical Record Documentation: Standards, Structure, and Medico-Legal Significance
Medical record documentation (IM29.13) is one of the most important professional skills a clinician acquires — and one of the most undervalued. The case record serves four simultaneous functions: a clinical communication tool (enabling continuity of care across shifts, specialties, and institutions), a medicolegal document (providing the primary evidence of what was done and why), a quality improvement resource (basis for audit and retrospective review), and a billing and administrative record (the foundation of hospital reimbursement under insurance and government schemes including Ayushman Bharat PM-JAY). Deficiencies in documentation, therefore, have clinical, legal, financial, and institutional consequences.
The NMC Code (Chapter 2) and standard medicolegal teaching in India specify the following requirements for valid case note documentation:
Every entry must include:
- Date and time — written in the 24-hour clock or with AM/PM clearly noted, because in a medico-legal context the exact sequence of events can be determinative
- The legible full name and designation of the author — a signature alone is legally insufficient if it cannot be identified; the NMC has upheld disciplinary actions where records were signed but not legibly attributed
- A specific, complete history — including the chief complaint in the patient's own words where possible, history of the presenting illness with temporal detail, relevant past medical and surgical history, drug history (including traditional/herbal medicines and allergies), and social history relevant to the clinical picture
- Physical examination findings documented in full — not 'normal' as a single word, but each system examined recorded as found; a 'normal' CNS in a patient presenting with headache is a different clinical statement from an unexamined CNS
- Medications prescribed must be documented by generic name (not trade name), dose in milligrams (not abbreviated), route, frequency, and duration; verbal orders must be countersigned within the same shift
- Investigation results — abnormal results noted with a clinician's acknowledgement signature, because a laboratory report that was received but not actioned is a common source of negligence claims
- Assessment and plan — a clinical impression (not a differential list of 10 diagnoses) and a specific plan with named actions
The clinical significance of documentation is best understood through the lens of errors. The Joint Commission (USA) and NABH (India) data consistently identify illegible medication orders, absent allergy documentation, and missing critical value acknowledgements as the three leading documentation-related causes of adverse drug events. In the Indian inpatient setting, the additional challenges of high patient-to-nurse ratios and cross-speciality ward coverage make a complete handover note — written at the end of every shift — an absolute requirement for patient safety.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
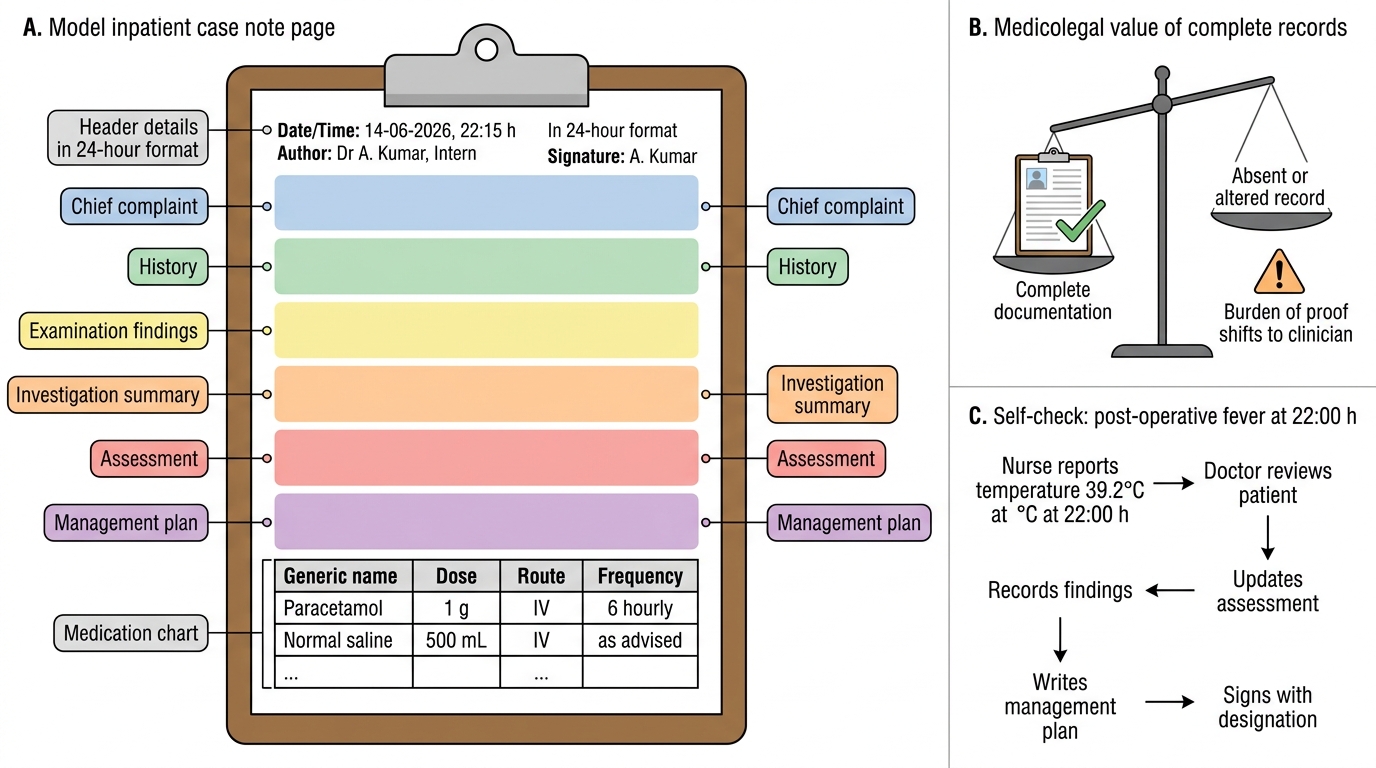
Model Inpatient Case Note: Required Documentation Elements
The medicolegal weight of documentation in India is defined by the Consumer Protection Act 2019 and the Indian Evidence Act. Under the Consumer Protection Act, medical services are 'services' and patients are 'consumers'; a deficiency of service — including negligent or incomplete documentation — is actionable before consumer courts. The principle established in multiple National Consumer Disputes Redressal Commission (NCDRC) rulings is that the burden of proof shifts to the clinician when documentation is absent, incomplete, or altered. If a patient claims they were not warned of a surgical risk and the consent form does not record the specific risk discussed, the court will typically give the benefit of the doubt to the patient. If a medication error is alleged and the prescription was not clearly written, the clinician bears the burden of proving the correct dose was prescribed. 'If it wasn't written, it didn't happen' is not merely a clinical aphorism; it is how Indian consumer courts and disciplinary committees apply the evidentiary standard.
SELF-CHECK
A nurse reports to you that a patient's post-operative temperature is 39.2°C at 22:00. You assess the patient, find it is likely superficial wound inflammation, and advise paracetamol. The nurse documents 'Patient febrile, doctor called, paracetamol given.' You do not write a note in the case record. Two days later, the patient develops a deep surgical site infection requiring return to theatre. The family considers a medico-legal complaint. What is the PRIMARY documentation failure in this scenario?
A. The nurse should not have documented without the doctor co-signing
B. There is no physician-authored record of the clinical assessment, differential diagnosis, or plan at the time of the adverse symptom
C. Paracetamol should have been documented only in the medication chart, not the case record
D. The documentation failure is minor — the nurse's note provides sufficient legal protection
Reveal Answer
Answer: B. There is no physician-authored record of the clinical assessment, differential diagnosis, or plan at the time of the adverse symptom
The critical failure is that there is no physician-authored case note recording the clinical assessment at 22:00. A nurse's note recording 'doctor called' establishes that the doctor was informed, but does not document what the doctor found on assessment, what the differential diagnosis was, or what the management plan was. In a subsequent medico-legal proceeding, the absence of this note means the physician cannot demonstrate that a competent clinical assessment was performed. Under the Consumer Protection Act 2019, the burden shifts to the physician to prove appropriate care was given — and without documentation, that is extremely difficult. The nurse's note provides no legal protection for the physician's clinical decision.
Teamwork, Privacy, Confidentiality, and Professionalism in the Healthcare Team
Teamwork (IM29.8) in a healthcare setting is not simply the ability to be pleasant to colleagues. It is the structured ability to communicate clinical information precisely, to function within a hierarchy without compromising patient safety, and to recognise when the behaviour of a team member — including a superior — represents a risk to patients. This last point is the hardest professionally, and it is the one the NMC curriculum specifically tests at the SH (Skill/Habit) level.
Effective healthcare teamwork has several behavioural components that are systematically taught in the crew resource management literature (adapted from aviation safety), now widely applied in medical education. These include: closed-loop communication (the receiver repeats back the message to confirm accuracy before acting — particularly important for verbal medication orders), situational awareness (every team member maintains a mental model of the patient's status and the team's workload), call-out and check-back (explicit verbal confirmation of critical steps, such as before administering a high-alert medication), and structured handover using a standardised format. The most widely used handover framework in Indian and international hospitals is the SBAR format: Situation (what is happening right now), Background (relevant clinical history and context), Assessment (what you think is going on), Recommendation (what you need the next clinician to do). An SBAR handover is faster, safer, and more complete than an unstructured verbal handover — and its adoption across a ward significantly reduces the rate of handover-associated adverse events.
Patient privacy (IM29.9) goes beyond keeping clinical information secret. It encompasses the physical and spatial privacy of the patient during examination and discussion. Pulling a curtain before examining a patient, lowering your voice when discussing a diagnosis within earshot of other patients, not reviewing a patient's records in a public area such as a canteen or lift, and not photographing a patient's condition with a personal mobile phone without explicit consent — these are all dimensions of privacy that final-year students are expected to demonstrate reflexively. The NMC Code Chapter 2 explicitly addresses the duty to protect patient information and the physical dignity of patients.
Confidentiality (IM29.10) as a professional habit requires active discipline, especially in the digital age. The growth of WhatsApp-based clinical communication, telemedicine platforms, and electronic health records creates new vectors for confidentiality breach. Sending a patient's case note as a WhatsApp photograph to a colleague — even for a clinically legitimate consultation — is a confidentiality breach unless the platform is encrypted and the patient has consented to digital communication of their records. India's Digital Personal Data Protection Act 2023 (DPDPA) extends the protection of personal information — including health data, which is classified as sensitive personal data — to digital environments. A practising physician who forwards patient information through an unsecured channel may be liable under both the DPDPA 2023 and the Consumer Protection Act 2019 in addition to the NMC Code.
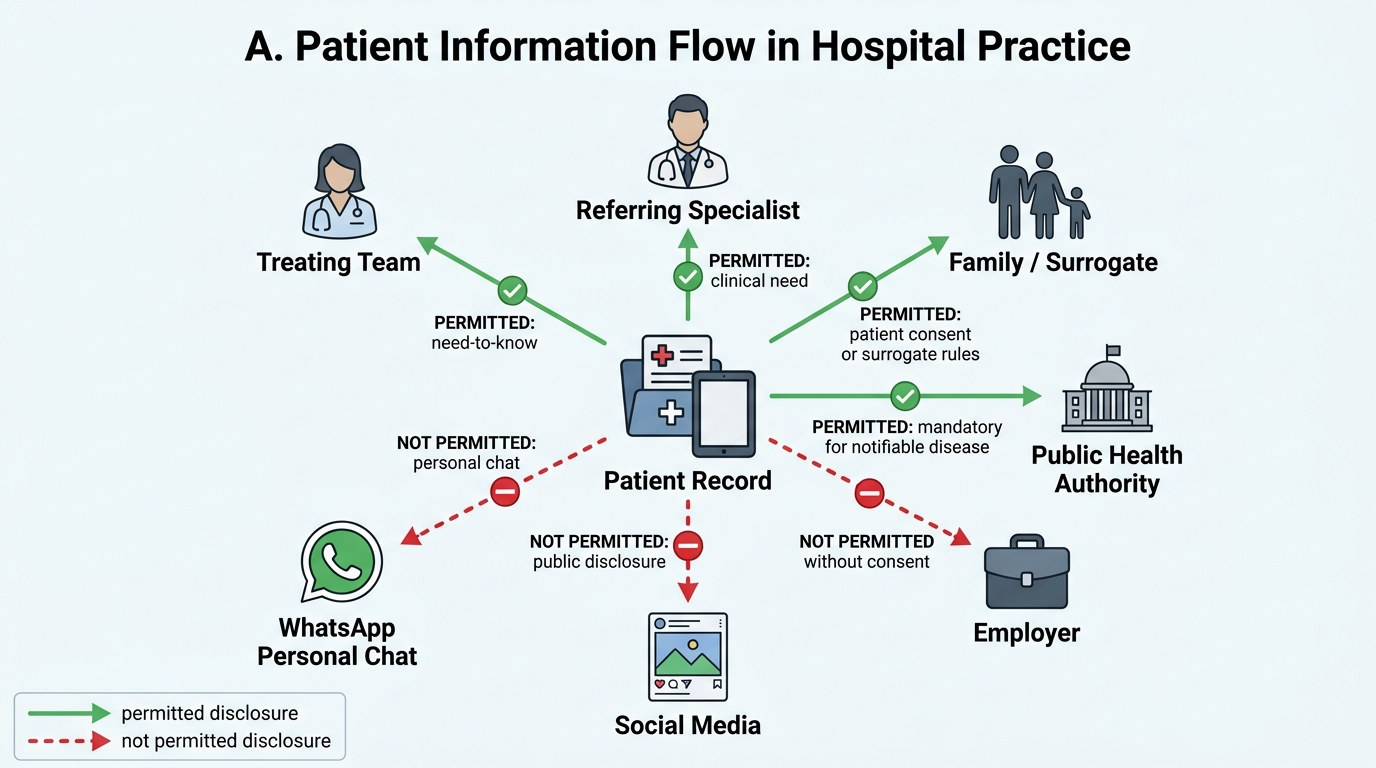
Permitted and Non-Permitted Patient Information Flows
Responsibility and work ethics (IM29.12) at the SH level includes: arriving prepared for ward rounds having reviewed overnight events and investigation results; completing assigned tasks by agreed deadlines and communicating if this is not possible; acknowledging and reporting errors rather than concealing them; being transparent about clinical uncertainty with seniors rather than guessing or improvising; and providing continuity of care through accurate written handover. Responsibility also includes knowing your limits — a core element covered in detail in the next module (IM29.16).
Altruism (IM29.25) as a professional quality is the disposition to prioritise the patient's welfare over personal convenience, financial interest, or status considerations. In concrete terms it means: staying late because the patient needs you, not because you will be credited; being willing to learn from a nurse or paramedical colleague who has observed something clinically significant; and advocating for a patient's needs even when it is uncomfortable to do so within the institutional hierarchy. The NMC Act 2020 expects registered practitioners to maintain these standards; the NMC Code makes explicit that financial interest must never override clinical judgment, and that participation in corporate-driven over-investigation or over-treatment is unethical and subject to disciplinary action.
Professional grooming (IM29.14) in clinical settings serves a specific infection control and professional communication function beyond aesthetics. Clinical environments are infection-risk environments, and the physical presentation of clinical staff directly affects cross-contamination risk. Bare below the elbows (BBE) practice — no watch, no jewellery, no long sleeves in clinical areas — was formally recommended by the NHS and subsequently adopted in NABH guidelines as part of hand hygiene protocol. Long, unkempt fingernails have been implicated in transmission of gram-negative pathogens including Pseudomonas aeruginosa and Klebsiella species in ICU settings. White coat length and cleanliness have been associated in patient perception studies with assessments of physician competence and trustworthiness — reflecting the social communication function of clinical dress. The practical standard in India: clean white coat over formal clothing, nails short and clean, hair tied back if long, identification badge visible, no strong perfume or cologne (which can cause nausea in ill patients), and closed-toe shoes in clinical areas.