Page 5 of 20
IM3.4-6 | Pneumonia Clinical Evaluation — SDL Guide
Learning Objectives
- Take a structured, systematic history in a patient with suspected pneumonia, addressing onset, sputum character, severity indicators, immune status, aspiration risk, exposure history, and vaccination status
- Perform a focused physical examination identifying the signs of consolidation (bronchial breathing, increased vocal resonance, whispering pectoriloquy, dullness) and distinguish these from signs of pleural effusion
- Calculate the CURB-65 score from clinical examination findings and use it to determine the appropriate site of care
- Recognise the clinical signs of complications including parapneumonic effusion, empyema, septic shock, and respiratory failure
- Generate and prioritise a differential diagnosis for a pulmonary opacity in the Indian context, including pneumonia, TB, malignancy, pulmonary embolism, and pulmonary oedema
INSTRUCTIONS
This module develops the clinical evaluation skills essential for diagnosing, staging, and differentially diagnosing pneumonia at the bedside. The history, examination, and differential diagnosis are not performed in sequence — they operate simultaneously as an integrated clinical reasoning process. Practice these skills in every ward and emergency room encounter with a breathless febrile patient.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 121 — Pneumonia (textbook)
- API Textbook of Medicine, 10th ed. — Clinical Skills in Respiratory Medicine (textbook)
- Macleod's Clinical Examination, 14th ed. — Respiratory System (textbook)
- BTS Guidelines for the Management of Community Acquired Pneumonia in Adults, 2019 (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the first doctor to see a 58-year-old woman in the emergency department triage area. She was brought in by autorickshaw, alone. She cannot give a full history because she is breathless at rest. Her daughter is on the phone — she says her mother has had a cough and fever for five days, and 'got very bad today.' You have 90 seconds before the next patient arrives. What history points can you extract in 90 seconds? What do you look for on a 60-second clinical examination that will tell you whether she needs oxygen, whether she needs the resuscitation bay, and what the most likely diagnosis is? The clinical evaluation of pneumonia is not a luxury performed after the patient is stable — it is the act that determines whether the patient becomes stable. Every question in the history, every physical sign you elicit, carries a specific diagnostic and prognostic weight. This module teaches you to perform that history and examination not as a ritual but as a targeted clinical instrument.
WHY THIS MATTERS
The NMC competencies IM3.4, IM3.5, and IM3.6 demand skills-level (SH) proficiency in history-taking, physical examination, and differential diagnosis in pneumonia — meaning you must be able to perform and document these at the bedside, not merely describe them. In Indian clinical settings, where resources are often stretched, the clinician's history and examination are frequently the primary diagnostic tools before investigations are even ordered. A systematic approach to history and chest examination is required not only for the accurate diagnosis of pneumonia but for assessing its severity, guiding the site of care decision (outpatient vs. ward vs. ICU), and identifying complications at first presentation. The ability to construct and prioritise a differential diagnosis from clinical features — before investigations — is a competency that distinguishes a trained clinician from a practitioner who waits for the CXR before forming any opinion.
RECALL
Recall the anatomy of the chest and the physical signs of consolidation from your second-year clinical skills training. In consolidation (as in pneumonia), the alveoli are filled with fluid/exudate — the lung tissue becomes solid. This solid medium transmits sound differently from air-filled tissue: breath sounds are bronchial (harsh, hollow, with equal inspiratory and expiratory components and a pause between) because the consolidated lung now acts like a solid conductor of laryngeal breath sounds; vocal resonance is increased (the solid medium transmits voice better); whispering pectoriloquy is present (whispered sounds transmitted clearly to the stethoscope); tactile fremitus is increased (vibrations transmitted through the consolidated lung to the chest wall); percussion gives a dull note (solid tissue does not resonate). Contrast this with pleural effusion: dull to percussion but breath sounds are reduced/absent (fluid dampens transmission) and vocal resonance is reduced. This distinction between consolidation and effusion at the bedside is tested in every clinical examination and is essential for recognising parapneumonic effusion complicating pneumonia.
Clinical Indication and Context: When to Suspect Pneumonia
The clinical suspicion of pneumonia arises from a constellation of presenting symptoms that, even before formal history-taking, should trigger a structured clinical evaluation. The classic presentation — acute onset fever, productive cough, breathlessness, and pleuritic chest pain — points immediately to a lower respiratory tract infection, but the range of actual presentations in clinical practice is far broader. Recognition of this range is the first clinical skill.
The classic presentation of bacterial (particularly pneumococcal) CAP includes: sudden-onset rigors followed by high fever (39–40°C), a productive cough with purulent (yellow or green) or rust-coloured sputum, pleuritic chest pain (sharp, worse on deep inspiration or cough, localised to the affected side — reflecting inflammation of the parietal pleura adjacent to the consolidation), breathlessness (from ventilation-perfusion mismatch in the consolidated lung and systemic inflammatory mediators reducing respiratory drive), and general systemic symptoms of infection (anorexia, myalgia, malaise). In older adults, the presentation is frequently atypical — the classical triad of fever, cough, and consolidation may be absent; instead, confusion, falls, reduced oral intake, worsening of chronic disease, or simply 'not being right' may be the presenting complaint. The absence of fever in older adults with pneumonia does not exclude severe infection — it may reflect impaired thermoregulation in the elderly.
Atypical presentations are associated specifically with atypical pathogens. Mycoplasma pneumoniae typically presents with a prodrome of headache, sore throat, and myalgia over several days before respiratory symptoms appear; the cough is characteristically dry and persistent rather than productive; fever is low-grade. The patient may be ambulatory despite having pneumonia — the 'walking pneumonia' picture. Legionella may present with prominent gastrointestinal symptoms (nausea, vomiting, diarrhoea), neurological features (confusion, headache), and notable hyponatraemia — the combination of a severe respiratory illness with neurological and GI features in an older male in the context of a water cooling system (hospital, hotel, industrial building) should immediately raise Legionella suspicion.
Occupational and exposure history provides direct clues to unusual pathogens: pigeon or bird contact (psittacosis/Chlamydophila psittaci), farm animal contact (Q fever/Coxiella burnetii), endemic area residence (TB, melioidosis in parts of North-East India), recent travel (Legionella at hotel water systems, Histoplasma in endemic areas), or animal carcass exposure. Immune status must be assessed at first contact — HIV testing history, CD4 count if known, any immunosuppressive medications, haematological malignancy, solid organ transplant, or long-term steroids.
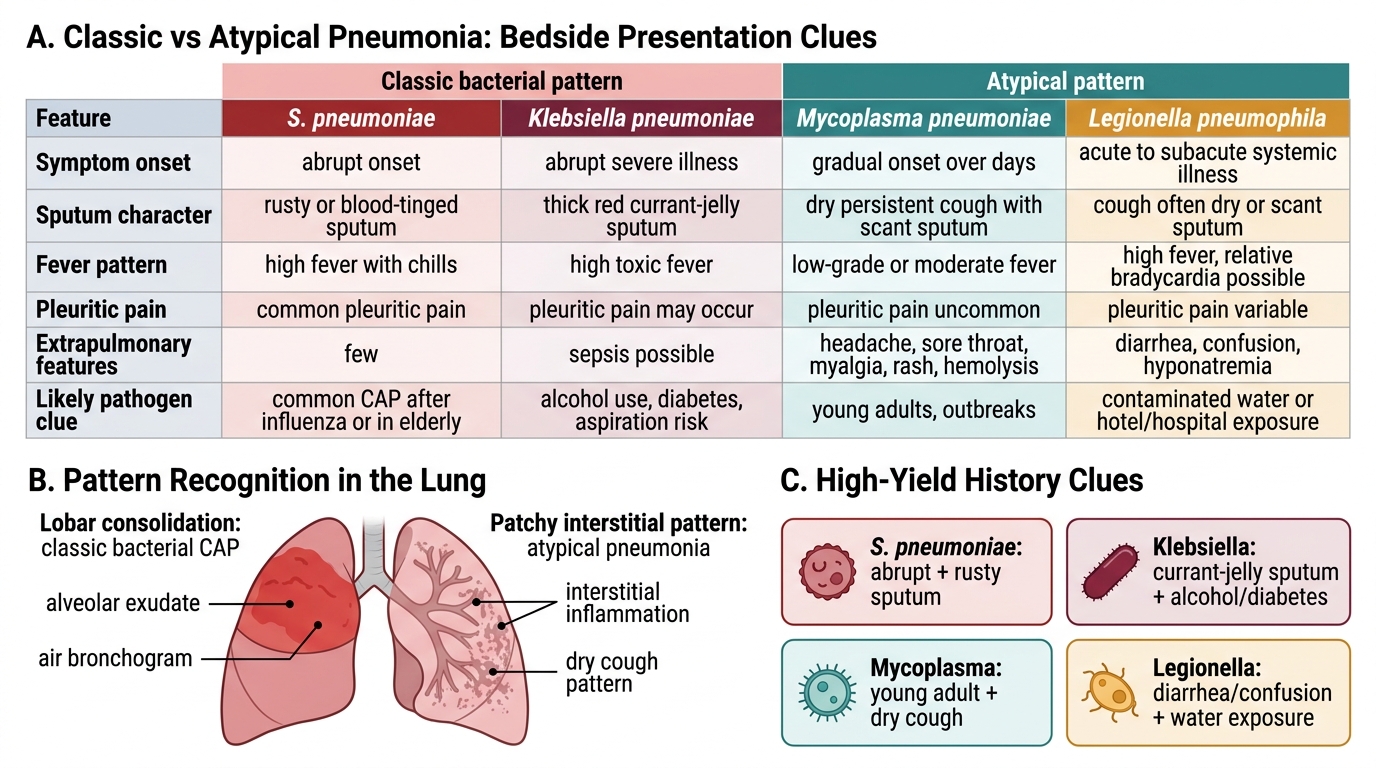
Classic vs Atypical Pneumonia: Presentation Clues
History-Taking in Pneumonia: A Systematic Approach
A structured history in pneumonia serves three simultaneous goals: confirming the pneumonia diagnosis, identifying the most likely pathogen, and assessing severity and risk factors that determine the site of care. These three goals should be consciously held in mind during the history, so that every question contributes to at least one of them rather than simply cataloguing symptoms. The following framework operationalises this approach for the bedside.
Presenting complaint and history of presenting illness: Begin with the onset — sudden (pneumococcal, aspiration) versus gradual over days to weeks (atypical, TB, post-obstructive from malignancy). Duration of symptoms: >1 week with gradual worsening suggests atypical pathogen or TB; acute onset within 24–48 hours is typical of bacterial CAP. Nature of cough: productive with purulent sputum (bacterial), dry persistent (Mycoplasma), blood-tinged/rusty (pneumococcal), viscous gelatinous red-tinged (Klebsiella). Haemoptysis — even small amounts — in the context of pneumonia should prompt specific TB screening (particularly in India) and consideration of lung abscess or post-obstructive pneumonia from a bronchogenic carcinoma. Fever pattern: high with rigors (bacterial, particularly pneumococcal), low-grade prolonged (atypical, TB). Pleuritic chest pain — sharp, localised, worse on inspiration and cough — is highly suggestive of pleural involvement adjacent to consolidation and is a classic feature of pneumococcal CAP. Breathlessness severity: graded by functional limitation — can the patient complete a sentence, walk to the toilet, lie flat?
Systemic and extrapulmonary symptoms: Confusion or altered mental status — both a symptom to document and a CURB-65 severity point. Gastrointestinal symptoms (nausea, vomiting, diarrhoea) and neurological symptoms (headache, altered consciousness) raise concern for Legionella. A rash, joint pains, or ear pain (bullous myringitis) with respiratory symptoms points toward Mycoplasma. Weight loss, night sweats, and prolonged low-grade fever with cough in India must invoke TB as a differential until excluded.
Risk factors and past medical history: Specifically document: (1) Immune status — HIV status (offer testing if unknown in appropriate risk groups), current or recent corticosteroid use, disease-modifying antirheumatic drugs (DMARDs), chemotherapy, haematological malignancy, diabetes mellitus, asplenia; (2) Structural lung disease — COPD, bronchiectasis, cystic fibrosis (each predisposes to specific pathogens: COPD → H. influenzae; bronchiectasis → Pseudomonas); (3) Aspiration risk factors — swallowing disorder (stroke, motor neuron disease, oesophageal disease), reduced consciousness (alcohol, sedatives, epilepsy), gastro-oesophageal reflux, recent general anaesthesia; (4) Prior pneumonias — recurrent pneumonia in the same lobe suggests anatomical obstruction (tumour, foreign body); recurrent bilateral pneumonias suggest systemic immune deficiency; (5) Recent hospitalisation or long-term care — the 90-day window that distinguishes CAP from HAP/healthcare-associated pneumonia (HCAP). Document all medications including previous antibiotic courses within 90 days (a risk factor for drug-resistant pathogens).
Social history: Smoking (major risk for pneumonia and for underlying COPD/cancer); alcohol use (risk for aspiration pneumonia and Klebsiella); occupation (see exposure history above); travel history; household contacts with similar illness; living conditions (overcrowding increases TB transmission risk in India); vaccination status — pneumococcal vaccine and influenza vaccine are specifically relevant and must be recorded.
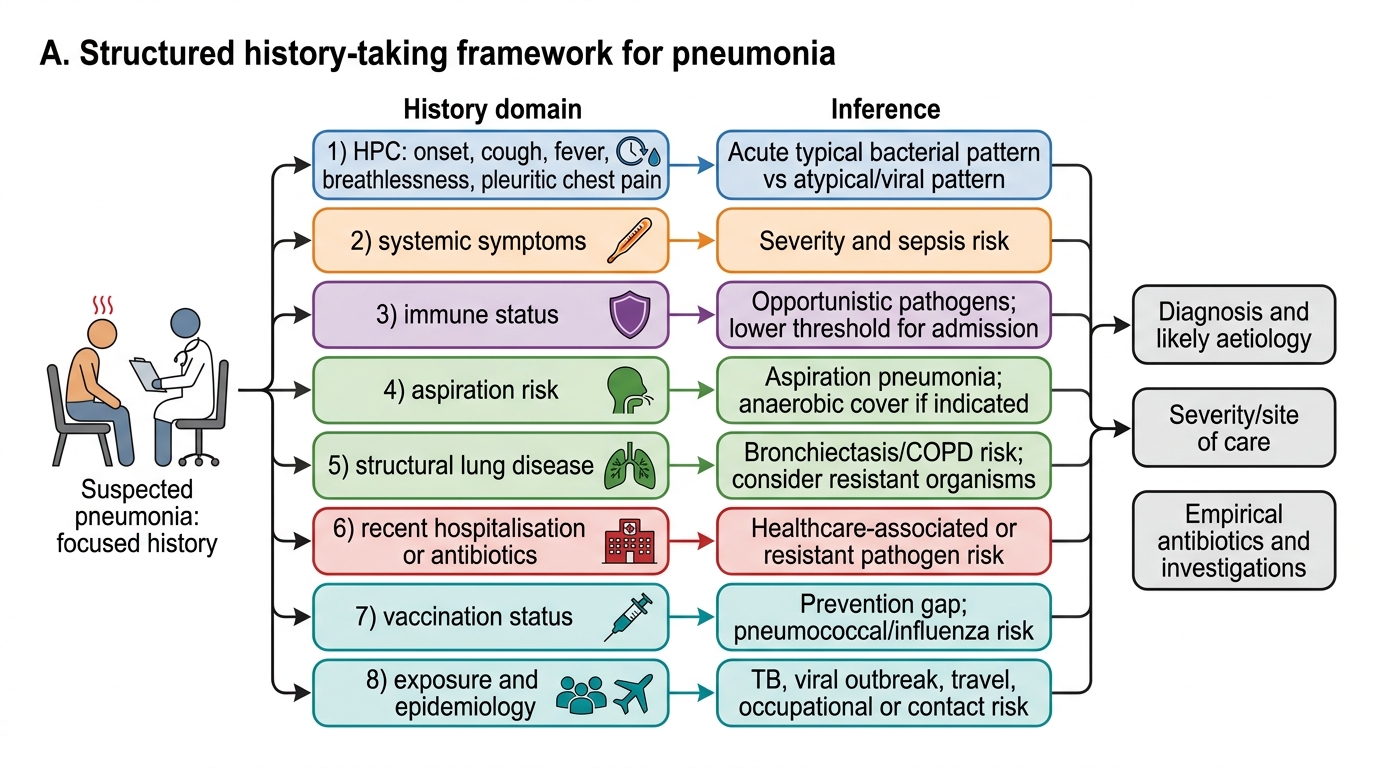
History-Taking Framework for Pneumonia
Physical Examination: Establishing Diagnosis, Severity, and Complications
Physical examination in pneumonia must be systematic but also purposeful — the findings you seek are those that confirm the diagnosis of consolidation, estimate severity (vital signs, oxygenation, mental status), localise the affected segment, and identify complications (pleural effusion, pneumothorax, septic shock, empyema). A normal chest examination in a breathless febrile patient does not exclude pneumonia — early consolidation may precede physical signs, and atypical and interstitial pneumonias may present with few auscultatory findings — but a characteristic constellation of signs remains one of the most reliable bedside diagnostic tools when present.
General examination and vital signs are the immediate priority and should be completed within the first 60 seconds. Document: temperature (fever ≥38°C; hypothermia <36°C in severe sepsis is an adverse sign), pulse rate (tachycardia ≥100/min — a universal marker of systemic illness and a CURB-65 surrogate via blood pressure), respiratory rate (≥30/min = CURB-65 point; the single most sensitive vital sign for severity), blood pressure (systolic <90 or diastolic ≤60 = CURB-65 point; hypotension signals septic shock), SpO2 (oxygen saturation on room air: <94% in non-COPD patients warrants supplemental oxygen; <90% is a red-flag requiring urgent assessment for respiratory failure). Mental status: new-onset confusion or AMTS ≤8 = CURB-65 'C' point; assess with a brief orientation-and-memory test at the bedside. BMI and nutritional status: cachexia raises TB concern. Pallor, icterus: haemolytic anaemia in Mycoplasma (cold agglutinins); hepatocellular dysfunction in Legionella or severe sepsis.
Peripheral examination (before chest): Cyanosis (central cyanosis in the mouth/tongue = severe hypoxia); digital clubbing (suggests chronic suppurative lung disease — bronchiectasis, lung abscess, empyema; its presence with acute pneumonia raises the possibility of a chronic underlying lung disease); lymphadenopathy (mediastinal lymphadenopathy on examination is absent but hilar lymphadenopathy on CXR may be seen in TB, sarcoidosis, or lymphoma presenting with 'pneumonia'); evidence of immunodeficiency (oral candidiasis, severe weight loss suggesting HIV/AIDS); herpes labialis (seen with pneumococcal pneumonia).
Chest examination follows the standard sequence: inspection → palpation → percussion → auscultation. Inspection: reduced movement of the affected side (guarding due to pleuritic pain); use of accessory muscles of respiration (sternocleidomastoid, scalene) in severe respiratory distress; intercostal recession in children (and in severe adult cases). Palpation: tracheal position — central in uncomplicated consolidation; may deviate TOWARD the side of consolidation if it is large and the opposite lung is normal; deviates AWAY from a large effusion or tension pneumothorax — this distinction is critical for detecting complications. Tactile vocal fremitus is increased over the area of consolidation (solid lung transmits the vibration of the laryngeal voice). Reduced or absent fremitus over an effusion (fluid damps vibrations). Percussion: dullness over the consolidated area — classic finding in lobar pneumonia. The percussion note over a pleural effusion is typically more stony-dull and extends to a broader area, often with a curved upper border (Damoiseau's line). Normal resonance persists over aerated lung. Auscultation: over the consolidated segment, bronchial breath sounds are the most specific finding — a harsh, hollow, blowing quality with equal inspiratory and expiratory phases and a pause between them, transmitted from the main airways through the solidified lung. Crepitations (coarse, late-inspiratory crackles) are often the earliest and most sensitive sign, audible before bronchial breathing establishes. Aegophony (a nasal 'bleat' quality when the patient says 'e' and the examiner hears 'a') and whispering pectoriloquy (whispered words transmitted clearly through the stethoscope over consolidation) confirm consolidation. Reduced or absent breath sounds over a pleural effusion.
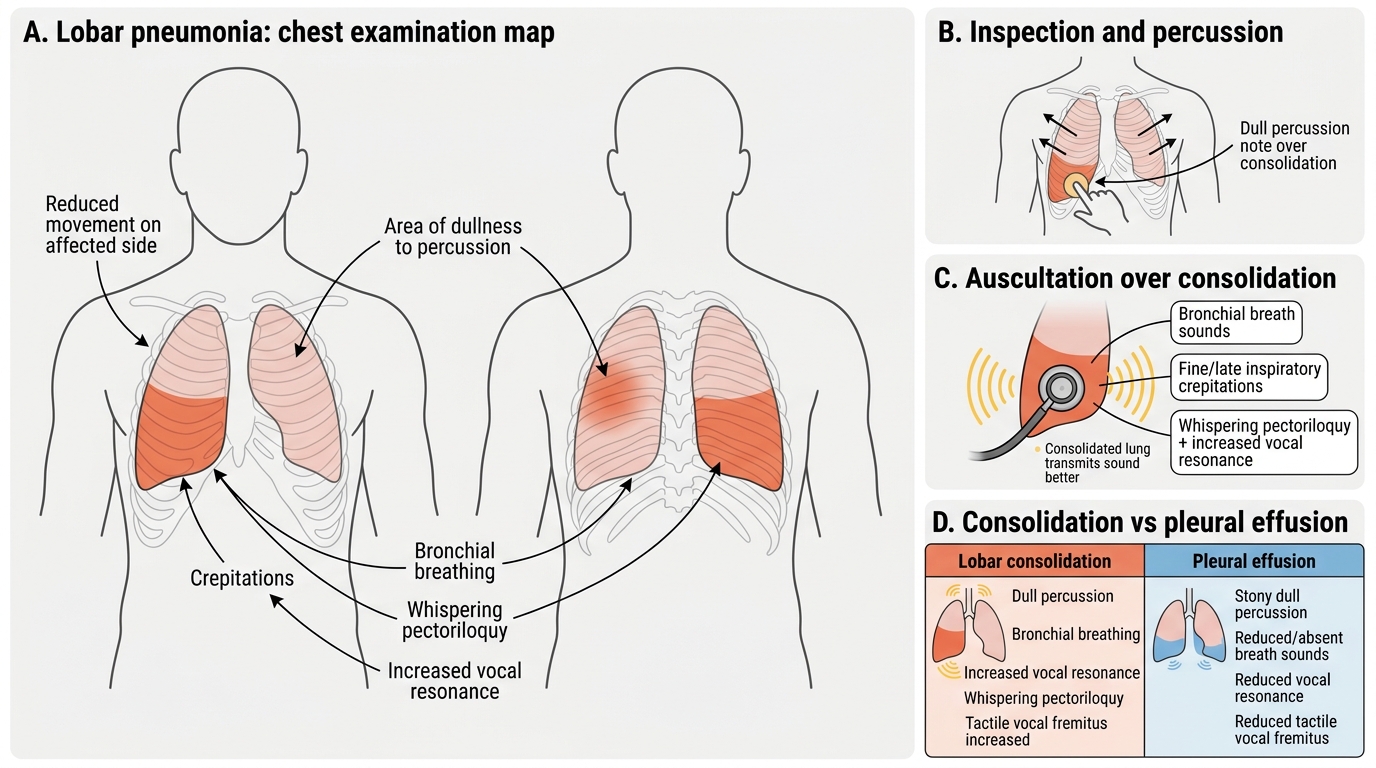
Chest Examination Findings in Lobar Pneumonia
SELF-CHECK
On auscultating the right lower zone of a 65-year-old man with fever, cough, and breathlessness, you hear bronchial breath sounds with increased vocal resonance, whispering pectoriloquy, and dull percussion note. Which finding BEST confirms the diagnosis of consolidation rather than pleural effusion?
A. Dull percussion note
B. Reduced breath sounds
C. Bronchial breath sounds with increased vocal resonance
D. Reduced tactile vocal fremitus
Reveal Answer
Answer: C. Bronchial breath sounds with increased vocal resonance
Both consolidation and pleural effusion produce a dull percussion note, so dullness alone does not distinguish them. The KEY distinction: consolidation transmits sound BETTER (bronchial breathing, increased vocal resonance, whispering pectoriloquy, increased tactile fremitus) because the solid medium conducts sound efficiently. Pleural effusion DAMPENS sound transmission (reduced/absent breath sounds, reduced vocal resonance, reduced tactile fremitus). Bronchial breath sounds with increased vocal resonance are specific to consolidation. Reduced breath sounds and reduced tactile vocal fremitus point to effusion.