Page 2 of 20
IM3.1-3 | Pneumonia Foundations — SDL Guide (Part 2)
Pathogenesis, Natural History, and Complications
The pathogenesis of pneumonia follows a common sequence regardless of the specific pathogen: a breach of the lower respiratory tract's normal defences allows organisms to reach the alveoli, triggering an inflammatory cascade that produces the consolidation, exudate, and systemic response that constitute the clinical syndrome. Understanding this sequence — from infection to inflammatory response to potential complication — allows the clinician to anticipate the course and recognise deviation from the expected trajectory.
The route of access to the alveoli may be: (1) micro-aspiration of oropharyngeal secretions — the dominant route in both CAP (during sleep or transient loss of normal swallowing reflexes) and HAP; (2) inhalation of airborne droplets — the primary route for Legionella (from aerosol sources), Mycoplasma (person-to-person droplets), and Mycobacterium tuberculosis (droplet nuclei); (3) haematogenous seeding from a distant focus of infection — characteristic of S. aureus pneumonia in the context of right-sided endocarditis or bacteraemia from an IV line infection; and (4) direct extension from contiguous infection — rare (subphrenic abscess, empyema from thoracic surgery). Once organisms reach the alveoli, a four-stage pathological sequence is classically described for lobar pneumococcal pneumonia: (a) congestion (0–24 hours) — alveolar capillaries are engorged, a serous exudate fills the alveoli; (b) red hepatisation (days 2–3) — a fibrinopurulent exudate with red blood cells and polymorphonuclear leucocytes fills the alveoli, giving the lobe a solid, liver-like consistency; (c) grey hepatisation (days 4–8) — red blood cells are lysed, the exudate becomes grey-yellow with predominantly macrophages and fibrin; (d) resolution (days 8–28) — the exudate is lysed by macrophages and expectoration, and the alveolar architecture is restored. It is the red blood cells lyse in stage (c) that produce the characteristic rust-coloured sputum of pneumococcal pneumonia.
The natural history of CAP in immunocompetent patients who receive appropriate antibiotics promptly is resolution of fever within 3–5 days, resolution of tachycardia and hypoxia within 5–7 days, and radiological clearance within 4–12 weeks (radiological resolution lags clinical recovery, particularly in the elderly — this is important so that a persisting opacity at 4 weeks does not automatically trigger a concern for malignancy, but should prompt follow-up imaging at 6–8 weeks to confirm clearance). Failure to improve clinically by 48–72 hours after starting appropriate antibiotics is a red flag that demands reassessment: consider resistant organism, incorrect diagnosis (TB, malignancy with post-obstructive pneumonia, eosinophilic pneumonia, cryptogenic organising pneumonia), empyema or lung abscess requiring drainage, or immunosuppression not previously identified.
Complications of pneumonia are best understood in three categories. Local complications: parapneumonic effusion (exudative pleural fluid adjacent to the pneumonia, occurring in up to 40% of hospitalised CAP) and empyema (frank pus in the pleural space, requiring drainage — the distinction between simple parapneumonic effusion and empyema is made by pleural fluid analysis, specifically pH <7.2, glucose <2.2 mmol/L, and LDH >1000 IU/L mark complicated/empyema); lung abscess (typically in aspiration pneumonia with anaerobes or in pneumonia caused by Klebsiella — a large cavity, often with an air-fluid level, which requires prolonged antibiotics and occasionally percutaneous drainage); and pneumothorax (uncommon, but seen with Staphylococcal pneumonia forming pneumatoceles). Systemic complications: bacteraemia and septicaemia (occurring in 20–30% of hospitalised pneumococcal CAP; associated with meningitis and endocarditis); acute kidney injury (from sepsis-related hypoperfusion and inflammatory nephritis); hepatitis (mild transaminase elevation common, particularly with Legionella); and hypotension/shock from systemic cytokine release. Respiratory complications: progression to acute respiratory distress syndrome (ARDS) in the most severe cases, requiring mechanical ventilation; hypoxaemic respiratory failure requiring supplemental oxygen or non-invasive ventilation.
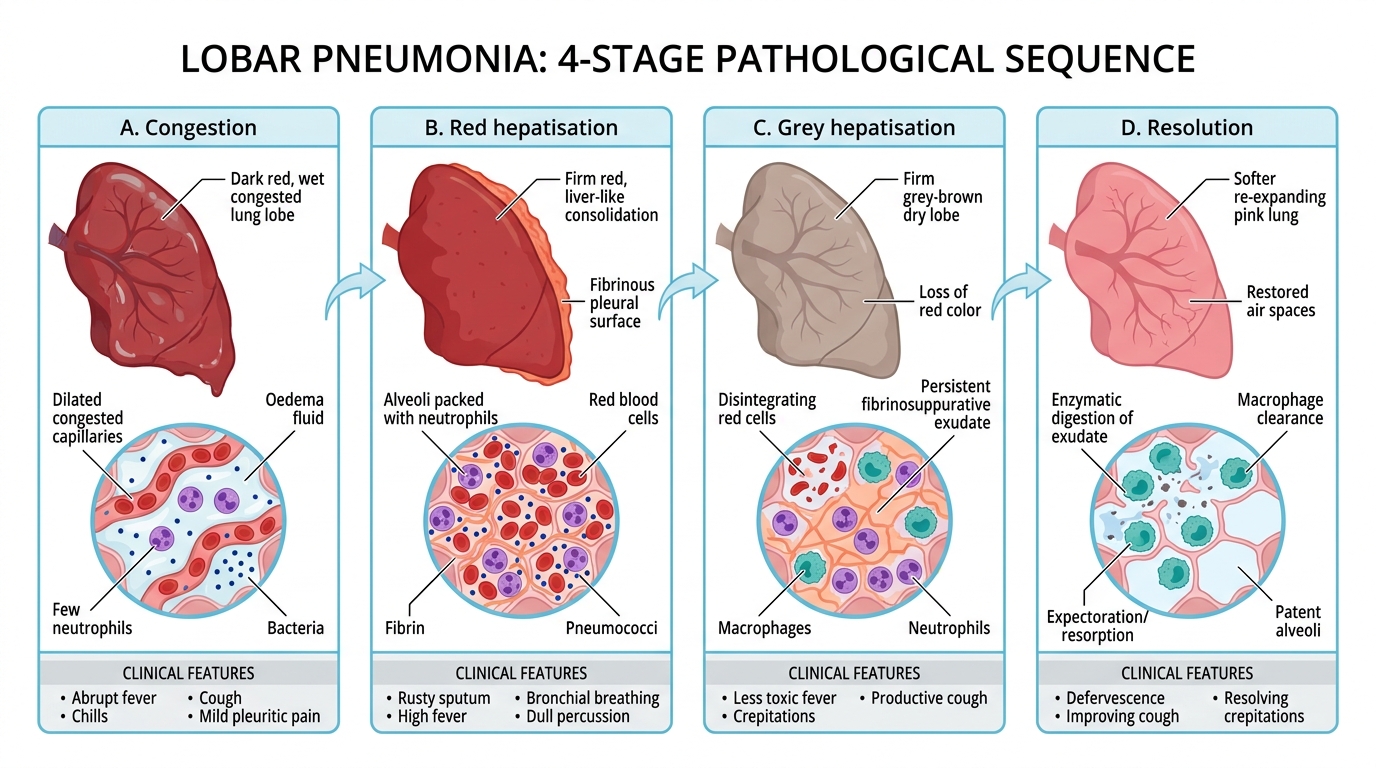
Four Stages of Lobar Pneumonia
Host Immune Status and Its Effect on Pneumonia Aetiology
The immune status of the host is the single most important modifier of the pneumonia pathogen spectrum beyond the acquisition setting. A pneumonia in an immunocompetent adult follows a predictable bacteriological pattern that permits rational empirical therapy; the same radiological opacity in a profoundly immunocompromised patient may be caused by organisms that would be handled without difficulty by an intact immune system. Recognising the host's immune context at the first clinical encounter is therefore as important as taking a respiratory symptom history, and it is explicitly required by NMC competency IM3.2 ('aetiologies of various kinds of pneumonia depending on the setting and immune status of the host').
Four categories of immunosuppression alter the pneumonia pathogen spectrum in clinically important ways. First, HIV/AIDS — the most numerically important cause of immunodeficiency in India in the context of pneumonia. At CD4 counts >200 cells/mm³, HIV-positive patients are susceptible to the same organisms as HIV-negative adults (pneumococcus dominant), though at higher rates. As CD4 falls below 200 cells/mm³, Pneumocystis jirovecii (formerly carinii) pneumonia (PCP) becomes the dominant opportunistic infection — an interstitial pneumonia characterised by progressive dyspnoea, dry cough, and bilateral perihilar ground-glass infiltrates on chest X-ray and HRCT, with marked hypoxia often disproportionate to the X-ray findings. LDH is typically elevated. At CD4 <100 cells/mm³, disseminated bacterial infections (non-typhoidal Salmonella, Mycobacterium avium complex) and fungal infections (cryptococcal pneumonia, endemic fungi) are added to the differential. In India, pulmonary tuberculosis is the most important co-infection in HIV — the two conditions interact bidirectionally, with HIV accelerating TB reactivation and TB accelerating HIV progression. NACO guidelines recommend TB screening in all HIV-positive patients and ART initiation within 2–8 weeks of starting anti-TB treatment (with earlier ART — within 2 weeks — in severely immunocompromised patients, i.e., CD4 <50 cells/mm³).
Second, haematological malignancy and chemotherapy — particularly patients with prolonged neutropenia (absolute neutrophil count <500/mm³) from induction chemotherapy for acute leukaemia, stem cell transplantation, or intensive chemotherapy for lymphoma. In this context, fungal pneumonias — particularly invasive pulmonary aspergillosis (IPA) — become the dominant opportunistic infection. IPA presents with fever not responding to broad-spectrum antibiotics, pleuritic chest pain, haemoptysis, and a nodular CXR opacity; the pathognomonic HRCT finding is the halo sign (a nodule surrounded by a ground-glass halo of haemorrhage). Diagnosis is by serum galactomannan (Aspergillus antigen) and HRCT; treatment is with voriconazole (first-line) or isavuconazole. Bacterial Gram-negative pneumonias (particularly Pseudomonas) are also common in neutropenia.
Third, solid organ transplant recipients on long-term immunosuppression (calcineurin inhibitors, steroids, mycophenolate) — at risk for Pneumocystis (requires ongoing prophylaxis with co-trimoxazole), CMV pneumonitis (particularly in the 1–6 months post-transplant 'window'), invasive fungal infections, and community-acquired pathogens at amplified risk.
Fourth, diabetes mellitus — while not causing the same degree of immunosuppression as the above, diabetes is the most common underlying condition in CAP presentations in Indian hospitals. Diabetic patients are specifically at elevated risk for Klebsiella pneumoniae pneumonia — a severe, often bilateral, necrotising pneumonia with the characteristic 'currant jelly sputum' (blood-tinged, gelatinous, from the highly viscous capsular polysaccharide) and a propensity for abscess formation; and for bacteraemic pneumococcal pneumonia with high severity scores.
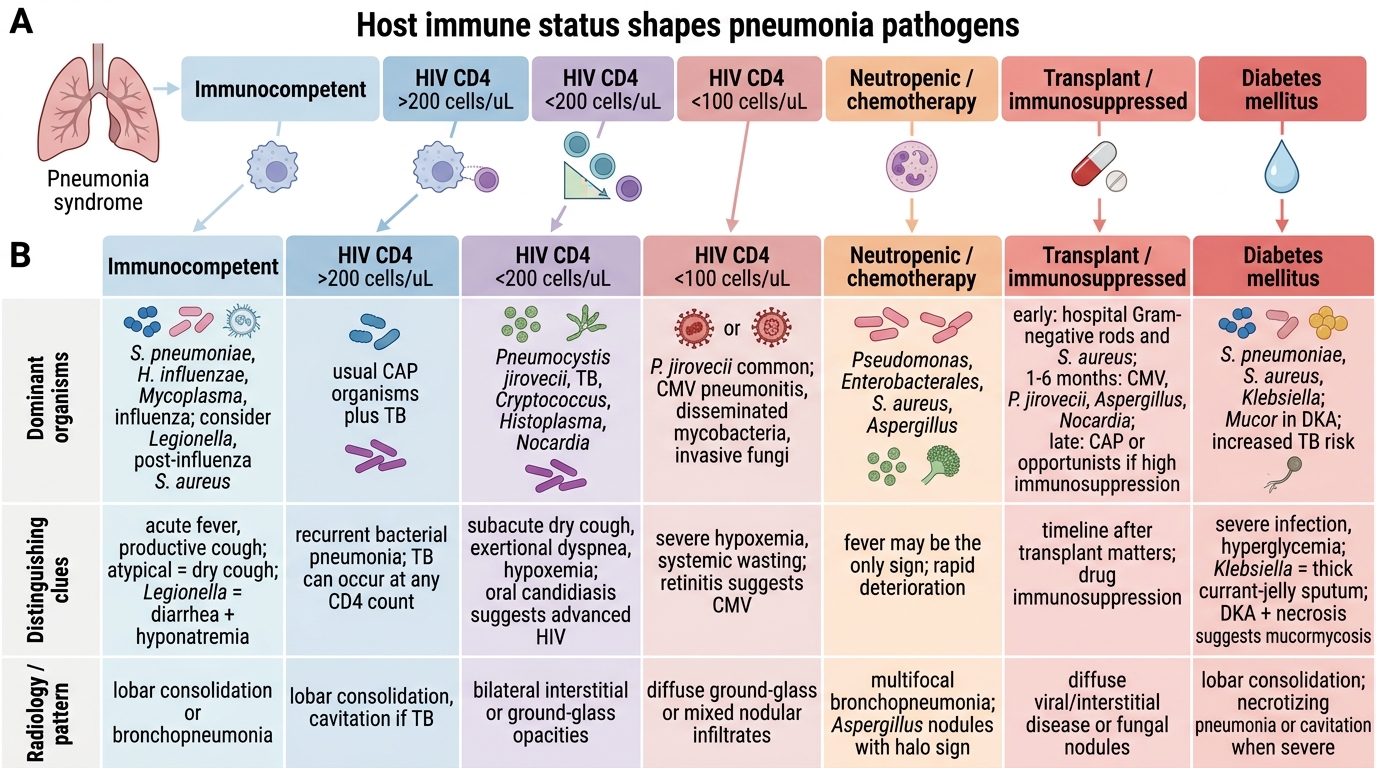
Host Immune Status and Pneumonia Pathogens
SELF-CHECK
A 36-year-old HIV-positive man (CD4 count 150 cells/mm³, not on ART) presents with 3 weeks of progressive breathlessness, a dry cough, and fever. His SpO2 is 82% on room air, but his chest X-ray shows only faint bilateral perihilar haziness. LDH is 620 IU/L. What is the MOST likely diagnosis?
A. Lobar pneumococcal pneumonia
B. Pulmonary tuberculosis
C. Pneumocystis jirovecii pneumonia (PCP)
D. Invasive pulmonary aspergillosis
Reveal Answer
Answer: C. Pneumocystis jirovecii pneumonia (PCP)
The classic PCP presentation: HIV-positive with CD4 <200 (150 here), subacute onset over weeks, dry cough, hypoxia disproportionately severe compared to the relatively subtle bilateral perihilar/interstitial CXR findings, and elevated LDH (a marker of pneumocyte damage in PCP). Lobar pneumococcal pneumonia has acute onset with lobar consolidation, not perihilar haze. TB would be more subacute/chronic with apical infiltrates or miliary pattern, not bilateral perihilar ground glass. Aspergillosis requires profound neutropenia (ANC <500) and shows nodules with halo sign, not perihilar haziness; it also occurs at CD4 <100 in HIV.
Diagnostic Principles in Pneumonia: A Foundational Overview
The investigation of pneumonia serves two goals that operate in parallel: confirming the diagnosis of lower respiratory tract infection (as opposed to alternative causes of the same radiological or clinical picture) and identifying the specific pathogen so that empirical therapy can be refined to directed, narrow-spectrum treatment. These two goals have different timelines — the diagnosis must be established and empirical treatment begun within hours, while pathogen identification from cultures typically requires 48–72 hours. Understanding this temporal gap is why the foundational knowledge of syndrome classification and likely pathogens (covered in earlier sections) directly drives the empirical antibiotic decision, and why cultures are obtained not to guide initial therapy but to refine or de-escalate it.
The diagnostic cornerstone of pneumonia is the chest X-ray — a new infiltrate or consolidation on the PA chest X-ray, in the right clinical context (fever, cough, breathlessness, and signs of consolidation on examination), confirms the diagnosis and localises the affected segment. The radiological pattern itself provides diagnostic clues: lobar homogeneous consolidation suggests pneumococcal CAP; bilateral patchy infiltrates suggest atypical pathogens or HAP; gravity-dependent opacity in dependent lung segments suggests aspiration; bilateral perihilar ground-glass suggests PCP; nodules with halo signs suggest invasive aspergillosis. However, CXR is neither sensitive nor specific in isolation — a patient with severe pneumonia and early consolidation may have a near-normal CXR (as in PCP or early neutropenic pneumonia), while an apparent consolidation may represent pulmonary oedema, pulmonary haemorrhage, or a malignancy.
The complete blood count (CBC) supports the diagnosis and gauges severity: a neutrophilia (WBC >12,000/mm³ with left shift) is typical of bacterial pneumonia; a leucopenia (WBC <4,000/mm³) is an adverse prognostic sign; lymphopenia raises concern for PCP or viral pneumonia. C-reactive protein (CRP) and procalcitonin are inflammatory markers that support the diagnosis and can guide antibiotic stewardship decisions — procalcitonin rises rapidly in bacterial infection and falls with effective treatment, making it a useful tool for deciding when to stop antibiotics. Sputum Gram stain and culture must be obtained before the first dose of antibiotics in hospitalised patients — though the yield is limited by contamination with oral flora, a good-quality sputum (>25 neutrophils, <10 squamous epithelial cells per low-power field) with a dominant Gram-positive diplococcus strongly supports pneumococcal aetiology. Blood cultures are obtained in all hospitalised patients before antibiotics — positive in 20–30% of bacteraemic pneumococcal CAP and essential for confirming bacteraemia and guiding de-escalation.
Severity assessment at diagnosis is an integral part of the diagnostic process — it determines the site of care (outpatient vs ward vs ICU), the route of antibiotic administration (oral vs IV), and the urgency of monitoring. The CURB-65 score is the most widely used CAP severity tool in clinical practice. CURB-65 assigns one point for each of: Confusion (new-onset, AMTS ≤8), Urea >7 mmol/L (blood urea nitrogen >19 mg/dL), Respiratory rate ≥30/min, Blood pressure (systolic <90 or diastolic ≤60 mmHg), 65 years or older. Total score ranges 0–5. Score 0–1: low severity, suitable for outpatient treatment. Score 2: intermediate severity, consider brief hospitalisation or close outpatient monitoring. Score ≥3: high severity, hospital admission strongly recommended; score ≥4 or 5: consider ICU.
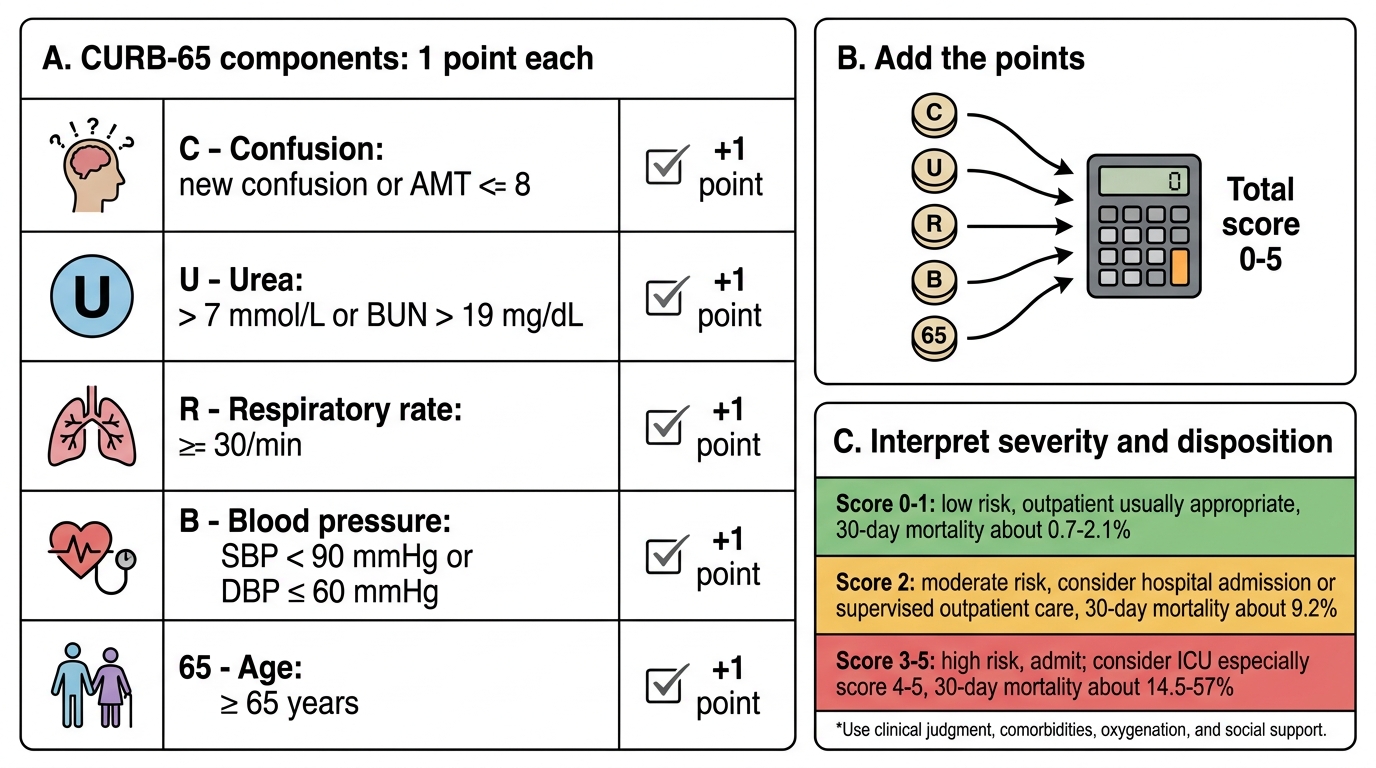
CURB-65 Score for Pneumonia Severity