Page 12 of 21
IM4.{13,15-17} | Febrile Syndrome Investigations — SDL Guide (Part 2)
Interpretation: Mantoux Test, Bone Marrow, and Imaging
Mantoux (PPD) test interpretation is a specific NMC competency (IM4.17) that requires mastery of technique, measurement, and context-adjusted reading. The test is performed by intradermal injection of 0.1 mL of purified protein derivative (PPD) — 5 tuberculin units (5 TU) in the Siebert (RT23) formulation used in India — into the volar forearm skin using a 26-gauge needle, producing a 6–10 mm wheal. The reaction is read at 48–72 hours by measuring the transverse diameter (width perpendicular to the long axis of the forearm) of the area of induration (palpable firmness from delayed-type hypersensitivity), NOT erythema. Induration is identified by inspection and palpation; the edges are marked with a ballpoint pen drawn toward the centre until resistance is felt (the ballpoint-pen roll method).
Interpretation thresholds (India/NTEP guidance):
- ≥10 mm induration in the general population (including BCG-vaccinated individuals) = significant (positive) reaction. In India, given the high background rate of latent TB and near-universal BCG vaccination, the 10 mm threshold is used for the general population.
- ≥5 mm induration in immunosuppressed individuals (HIV, systemic corticosteroids ≥15 mg/day prednisone equivalent, anti-TNF agents, organ transplant recipients) = significant. The threshold is lowered because the immune response is impaired and even a smaller reaction indicates sensitisation.
- <5 mm = negative (non-reactive) in immunocompetent patients.
Critical caveats for interpretation: (1) A positive Mantoux does NOT distinguish latent TB infection from active TB disease — it indicates immunological sensitisation at some point; (2) A negative Mantoux does NOT exclude active TB — anergy from malnutrition, severe immunosuppression, disseminated TB (miliary TB), or overwhelming infection can produce false-negative results; (3) BCG vaccination produces a reaction typically 6–14 mm in diameter that is indistinguishable from TB sensitisation within a few years; the IGRA (interferon-gamma release assay — QuantiFERON-TB Gold or T-SPOT.TB) does not cross-react with BCG and is therefore more specific in BCG-vaccinated populations.
Bone marrow aspiration and biopsy (IM4.15 — observe and assist in a simulated environment) is performed from the posterior superior iliac spine (PSIS) in most adult patients (anterior superior iliac crest or sternum are alternatives but PSIS is preferred for safety). Technique: patient in lateral decubitus; skin, subcutaneous, and periosteal infiltration with 1% lignocaine; introduce the Jamshidi needle (for trephine biopsy) or Illinois needle (for aspiration) with a twisting, drilling motion; once in the marrow cavity, stylet is removed and 0.5–2 mL of marrow is aspirated (large volumes dilute the marrow with peripheral blood). Aspiration yield (morphology, cytogenetics, culture): smear is stained with Giemsa or May-Grünwald for morphology; trephine core (biopsy) is fixed in formalin for histology. Complications: pain, haematoma, infection (rare), vascular or neural injury (rare at PSIS).
Indications for bone marrow in febrile syndromes: suspected haematological malignancy (leukaemia, lymphoma with bone marrow involvement), visceral leishmaniasis (Leishman-Donovan bodies = amastigotes in macrophages), miliary TB (culture of marrow positive in 30–40%), HLH (haemophagocytosis — macrophages engulfing red cells, leucocytes, and platelets — diagnostic for HLH when found in context), unexplained pancytopaenia in a febrile patient, fever with abnormal peripheral blood cells (blast cells, atypical lymphocytes).
Imaging in febrile syndromes is indicated for specific clinical purposes as enumerated in IM4.16. Chest X-ray is the most widely used first-line imaging in febrile syndromes: consolidation with air bronchogram = lobar pneumonia; bilateral fine nodular (miliary) pattern = miliary TB; cavitation in upper lobes = active/post-primary TB; hilar lymphadenopathy + bilateral pulmonary infiltrates = sarcoidosis, primary TB, lymphoma; bilateral ground-glass opacities in an HIV patient with CD4 <200 = PJP. Ultrasound abdomen (most widely available first-line cross-sectional imaging in India): spleen size, echogenicity, and splenic infarcts; hepatomegaly character; pericholecystic fluid (cholecystitis, acalculous cholecystitis); focal liver lesion with peripheral enhancement and hypoechoic centre = amoebic liver abscess; lymphadenopathy (mesenteric, para-aortic); free fluid (ascites, blood). CT chest/abdomen/pelvis provides superior anatomical detail for mediastinal/retroperitoneal/mesenteric lymphadenopathy, interstitial lung disease, splenic lesions, and staging of haematological malignancies. PET-CT (FDG-PET) has the highest yield for identifying occult malignancy or inflammatory foci in classic FUO — increasingly available in tertiary centres; it identifies metabolically active tissue regardless of anatomical location. Echocardiography is indicated for suspected endocarditis (vegetation, perivalvular abscess) and cardiac myxoma; transoesophageal echocardiography (TEE) has superior sensitivity compared to transthoracic (TTE) for detecting vegetations <10 mm and prosthetic valve endocarditis.
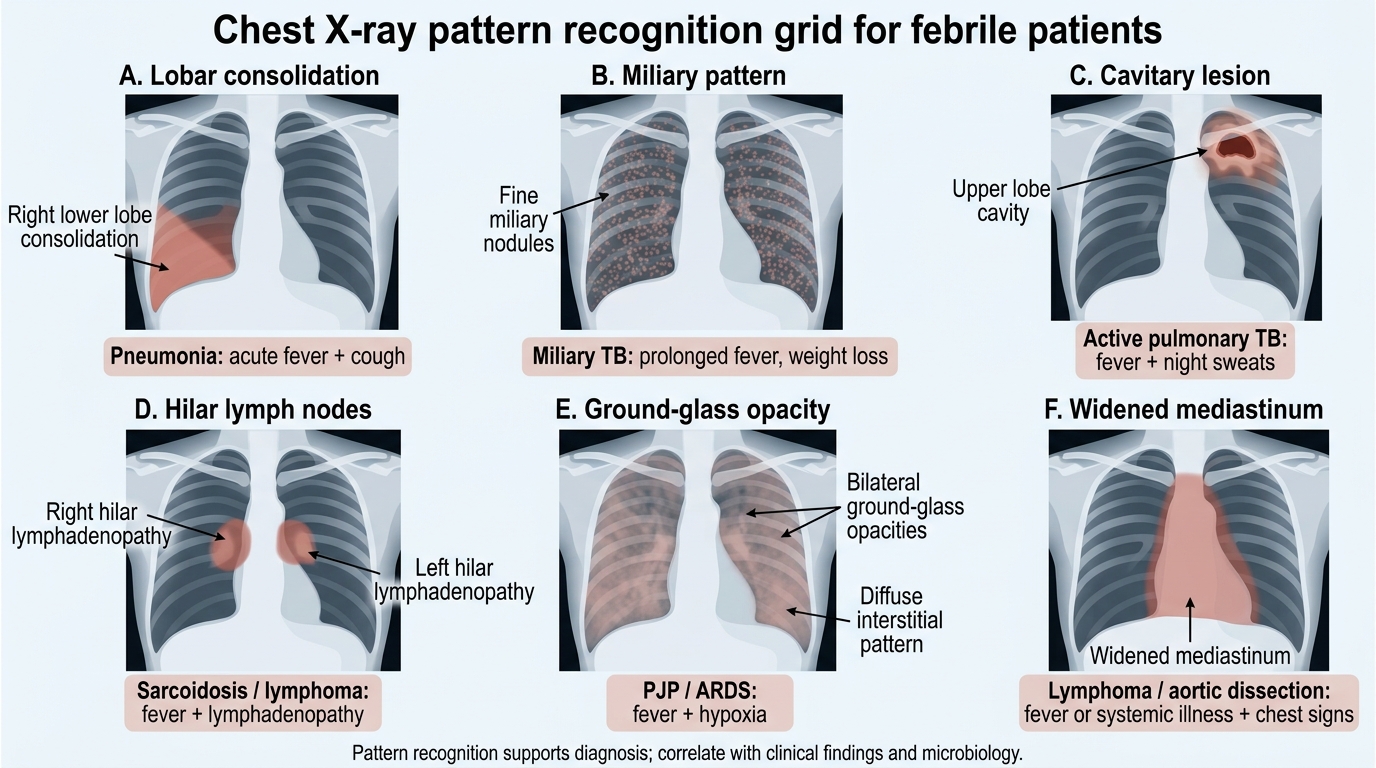
Chest X-Ray Patterns in Febrile Patients
SELF-CHECK
A 42-year-old woman on methotrexate for rheumatoid arthritis undergoes a Mantoux test as part of a TB screening before starting anti-TNF therapy. She received BCG at birth. The Mantoux reaction is read at 72 hours and shows 6 mm of induration. Which statement about the interpretation is correct?
A. This is a negative result (below the 10 mm threshold) and TB screening is complete
B. This is a positive result because the threshold for immunosuppressed patients is ≥5 mm
C. BCG vaccination makes the Mantoux uninterpretable; repeat with IGRA
D. A reaction of 6 mm is always due to BCG vaccination and not TB sensitisation
Reveal Answer
Answer: B. This is a positive result because the threshold for immunosuppressed patients is ≥5 mm
This patient is immunosuppressed (methotrexate use; planned anti-TNF therapy). In immunosuppressed patients — those on corticosteroids ≥15 mg/day, anti-TNF agents, transplant recipients, HIV-positive patients — the Mantoux threshold for a positive (significant) result is ≥5 mm, not the standard 10 mm used for the general population. A 6 mm induration in this immunosuppressed woman is therefore a POSITIVE result and indicates TB sensitisation requiring further evaluation before anti-TNF therapy is started. BCG vaccination can produce reactions that overlap with true TB sensitisation (typically 6–15 mm), and in a BCG-vaccinated immunosuppressed patient, IGRA is preferred for greater specificity — but the key point is that 6 mm in this context IS positive at the ≥5 mm threshold.
Applied Practice: Selecting and Interpreting Investigations in Clinical Scenarios
This section presents integrated clinical scenarios that require you to select the appropriate investigation panel based on the differential diagnosis, then interpret the results. This directly tests the NMC IM4.13, IM4.15, IM4.16, and IM4.17 competencies in the applied context.
Scenario A — Fever with cytopenias: A 55-year-old from West Bengal has had fever for 5 weeks, massive splenomegaly (spleen 14 cm below the left costal margin), haemoglobin 7.2 g/dL, WBC 2,400/mm³ (differential: neutrophils 58%, lymphocytes 38%, monocytes 4%), platelets 62,000/mm³. The pancytopaenia pattern with massive splenomegaly in an endemic-zone patient suggests visceral leishmaniasis. The rK39 rapid test is positive. What is the role of bone marrow aspiration, and what would you expect to find?
Analysis: The rK39 positive result in this clinical context is sufficient for diagnosis and treatment initiation. Bone marrow aspiration is indicated to confirm the diagnosis if the rK39 is equivocal or negative, if there is suspicion of concurrent lymphoma (the presentation can overlap), or for baseline assessment before treatment. On bone marrow aspirate: Leishman-Donovan bodies — 2–4 μm amastigotes with a round nucleus and kinetoplast (appearing as two dark dots) within the cytoplasm of macrophages (histiocytes) — are diagnostic. The bone marrow also shows erythroid hyperplasia (from haemolytic anaemia) and hypercellularity. NB: in some cases, liver or splenic aspiration may be higher yield than bone marrow, but splenic aspiration carries significant haemorrhage risk and is performed only in specialised centres.
Scenario B — Fever with miliary CXR: A 38-year-old male clerk presents with 6 weeks of fever, 8 kg weight loss, night sweats, and a chest X-ray showing bilateral fine nodular shadows in a miliary pattern. WBC is 5,200 (normal), haemoglobin 10.5 g/dL. Mantoux test is read at 72 hours: 0 mm induration. How do you interpret the Mantoux result, and what is the next investigation?
Analysis: The Mantoux is 0 mm in a patient with miliary TB — this is a false-negative result due to anergy. In miliary TB, the massive disseminated bacillary load overwhelms the cellular immune response, causing a state of immunological anergy in which the delayed-type hypersensitivity reaction is suppressed. The negative Mantoux must NOT be used to exclude TB in this clinical context. The next steps are: (1) bronchoscopy with BAL — for AFB smear (sensitivity 40–60% in miliary TB), CBNAAT/Xpert MTB/RIF (sensitivity 70–80%), and culture; (2) bone marrow biopsy — culture of bone marrow is positive in 30–40% of miliary TB cases; (3) fundoscopy — to look for choroidal tubercles (pale lesions in the choroid — pathognomonic of miliary TB when present); (4) IGRA (QuantiFERON-TB Gold) — more specific than Mantoux; however, IGRA can also be negative in severe immunosuppression. Treatment should be started empirically if the clinical and radiological picture is compelling and the patient is deteriorating, even if microbiological confirmation is awaited.
Scenario C — Fever with altered consciousness: A 19-year-old college student develops fever (39.2°C), severe headache, and neck stiffness over 12 hours. Fundoscopy shows no papilloedema. A lumbar puncture is performed. CSF findings: appearance turbid, opening pressure 28 cm H₂O (elevated), WBC 2,600 cells/mm³ with 92% neutrophils, protein 180 mg/dL, glucose 28 mg/dL (serum glucose 96 mg/dL, ratio 0.29). Gram stain shows Gram-negative diplococci. What is the diagnosis, and what immediate treatment is indicated?
Analysis: This is bacterial meningitis — the CSF findings are unambiguous: turbid appearance, markedly elevated WBC with neutrophilic predominance, elevated protein, and critically low glucose (CSF:serum ratio 0.29, well below the 0.5 threshold). The Gram stain showing Gram-negative diplococci is consistent with Neisseria meningitidis (meningococcal meningitis). Immediate treatment: IV benzylpenicillin 2.4 g four-hourly (or IV ceftriaxone 2 g twice daily, which is preferred in India for broader coverage) plus IV dexamethasone 0.15 mg/kg four-hourly for 4 days (reduces hearing loss and neurological sequelae in bacterial meningitis by suppressing cytokine-mediated inflammation). Simultaneously, notify public health authorities — meningococcal disease is a notifiable disease in India. Close contacts should receive ciprofloxacin or rifampicin prophylaxis.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
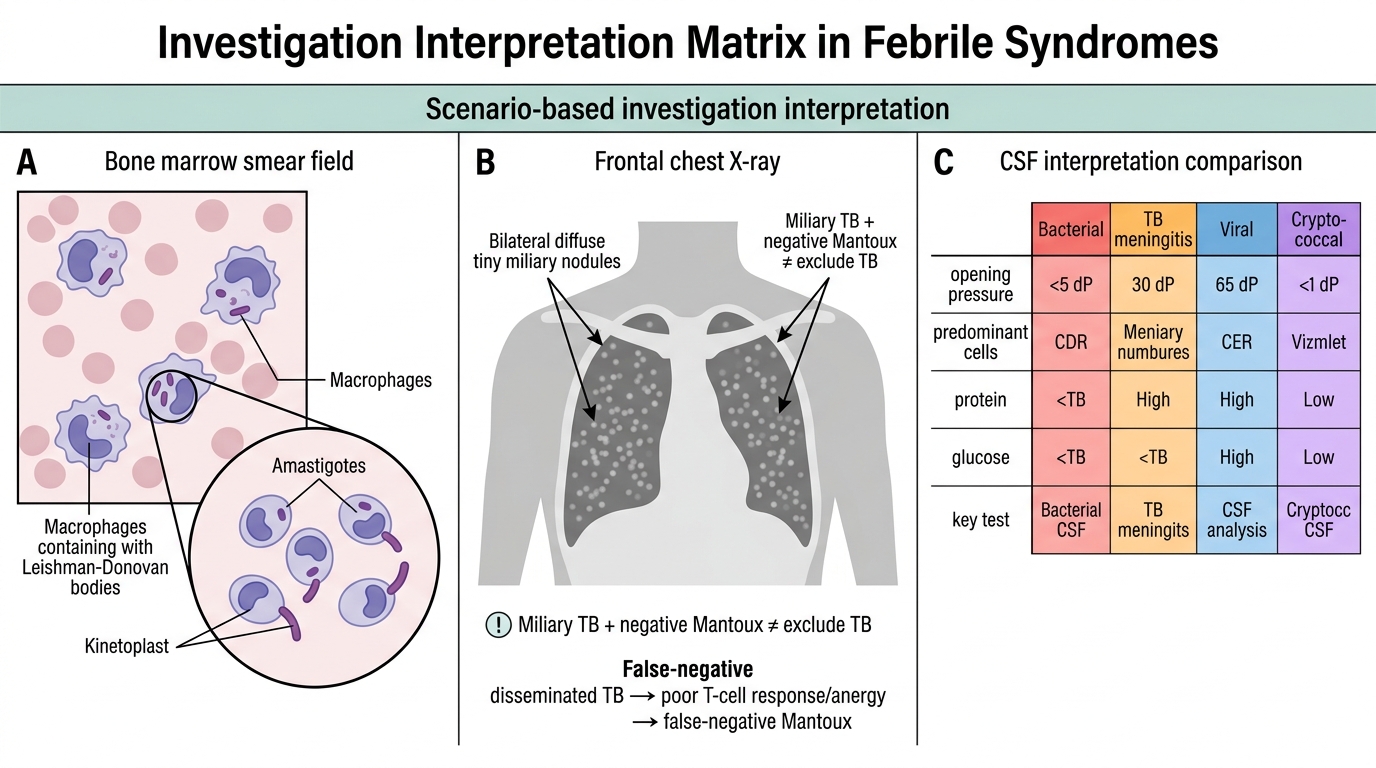
Investigation Interpretation Matrix in Febrile Syndromes
Self-Assessment: Investigation Competency Consolidation
This self-assessment consolidates the investigation competencies developed in this module. Four focused questions test your ability to select, perform, and interpret key investigations in febrile syndromes. Work through each question independently before reading the analysis.
Q1 — Blood culture technique: You are about to draw blood cultures in a febrile patient suspected of having infective endocarditis. You have three culture bottle sets available. Outline the correct technique to maximise yield, and specify the single most important determinant of blood culture sensitivity.
Analysis: Draw 3 sets from 3 different venepuncture sites at 20–30 minute intervals. Decontaminate each site with 2% chlorhexidine or povidone-iodine + alcohol; allow to dry before inserting the needle. Inoculate 10 mL per bottle (20 mL per set — 60 mL total). The single most important determinant of blood culture sensitivity is blood volume per culture set (10 mL per bottle), not the timing relative to fever spikes. Common errors: inadequate volume (most common), using the same venepuncture site for multiple bottles, and failure to allow the disinfectant to dry.
Q2 — Mantoux technique: You are asked to perform a Mantoux test on a 10-year-old child who is a close household contact of a newly diagnosed smear-positive TB case. The child received BCG at birth. Describe the technique, the reading time, and how you would interpret the result.
Analysis: Technique: intradermal injection of 0.1 mL of 5 TU PPD RT23 into the volar surface of the left forearm with a 26-gauge needle to produce a 6–10 mm bleb. Read at 48–72 hours (72 hours preferred for maximum sensitivity). Measure the transverse diameter of induration (not erythema) using a transparent ruler or the ballpoint-pen roll method. In a household TB contact, the threshold for a positive result is ≥10 mm — because close contacts have a higher pre-test probability of TB exposure, the standard 10 mm threshold applies. A positive result in a child who is a household contact does not distinguish latent TB from early active disease — the child needs a chest X-ray and clinical evaluation to exclude active TB before deciding between preventive therapy (isoniazid preventive therapy, IPT) or active TB treatment.
Q3 — Imaging indication: A 42-year-old woman has prolonged fever (5 weeks), cervical and axillary lymphadenopathy, and an LDH of 380 U/L. Chest X-ray shows bilateral hilar lymphadenopathy. Blood cultures, malaria smear, and Widal are all negative. What imaging investigation is most appropriate next, and what is its specific indication?
Analysis: The most appropriate next imaging investigation is contrast-enhanced CT chest/abdomen/pelvis (CECT). The indication is characterisation and staging of lymphadenopathy — the combination of bilateral hilar lymphadenopathy, cervical and axillary node involvement, elevated LDH, and prolonged fever with constitutional symptoms raises lymphoma as the primary diagnostic concern. CECT defines the distribution of nodal disease (mediastinal, retroperitoneal, mesenteric), identifies organomegaly, and may reveal lesions suitable for CT-guided biopsy. The next step after CT is lymph node biopsy (excisional preferred over FNAC for lymphoma — FNAC provides cytology but not the architectural pattern needed for lymphoma subtyping). PET-CT would provide functional staging if lymphoma is confirmed.
Q4 — Stool examination: A 35-year-old returns from Rajasthan with fever and four to five bloody mucoid stools per day for 5 days with lower abdominal cramps. WBC is 14,000 with 82% neutrophils. Outline the stool investigations and what you expect to find.
Analysis: Stool investigations for bloody diarrhoea with fever: (1) Stool routine examination (microscopy): look for red blood cells (indicate mucosal damage), pus cells (polymorphonuclear leucocytes — indicate mucosal inflammation, present in bacterial and amoebic dysentery), and Entamoeba histolytica trophozoites — a pear-shaped motile amoeba with ingested RBCs in the cytoplasm (pathognomonic of invasive amoebiasis; must be examined in a fresh warm stool specimen as trophozoites lose motility rapidly). (2) Stool culture on MacConkey and SS agar for Salmonella, Shigella, Campylobacter, and E. coli O157:H7 — incubation at 37°C for 24–48 hours; relevant sensitivity is 60–80% for Shigella in acute bloody diarrhoea. (3) Stool antigen test for Entamoeba histolytica (ELISA-based) is more sensitive than microscopy and differentiates E. histolytica from the non-pathogenic E. dispar. In this patient, the bloody mucoid stool with fever and WBC leucocytosis suggests bacillary dysentery (Shigella) as the most probable cause; invasive amoebiasis is also possible. The travel history to Rajasthan is non-specific. Key differentiator: amoebic dysentery tends to have lower fever, fewer stools, less systemic toxicity, and trophozoites on microscopy; Shigella dysentery causes higher fever, more frequent stools, significant systemic illness, and absence of trophozoites.

Bone Marrow Aspiration and Trephine Biopsy from the PSIS
CLINICAL PEARL
The Mantoux test has two critical pitfalls that are responsible for diagnostic errors every day in Indian medicine. The first is reading the erythema (redness) instead of the induration (palpable firmness) — the induration may be only 6 mm while the erythema is 20 mm, and the erythema is clinically irrelevant. Use the ballpoint-pen roll technique and measure only what you can feel. The second pitfall is applying the 10 mm threshold to immunosuppressed patients — in HIV-positive, transplant, anti-TNF-treated, or corticosteroid-treated patients, the threshold is ≥5 mm. A 6 mm induration in an HIV-positive patient is a positive test requiring evaluation; the same 6 mm in a healthy young person is negative. Context changes the cut-point completely.