Page 1 of 21
IM4.1-8 | Fever Foundations — SDL Guide
Learning Objectives
- Distinguish fever from hyperthermia based on pathophysiology and clinical significance
- Describe the febrile response cascade from pyrogen to prostaglandin-mediated thermostat reset
- Enumerate the common causes of fever and hyperthermia across the Indian geographic and epidemiological context
- Explain how host immune status, comorbidities, age, and special populations alter the febrile response
- Describe the inflammatory, malignant, and infectious categories of fever aetiology
- Outline the approach to the acutely febrile patient including immediate danger-sign recognition
- Describe the pathophysiology, clinical continuum, and management of sepsis syndrome
- Describe the spectrum of heat-related illness: heat cramps, heat exhaustion, and heat stroke
INSTRUCTIONS
Fever is among the most common presenting complaints in internal medicine wards across India, yet it conceals a diagnostic spectrum from viral self-limiting illness to life-threatening sepsis. This module builds your conceptual architecture around the febrile response — from molecular mechanisms to bedside pattern recognition — and equips you to recognise when fever signals danger. Read each section actively, connect the pathophysiology to the clinical pictures, and test yourself with the embedded questions.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 10 — Fever and Hyperthermia (textbook)
- API Textbook of Medicine, 10th ed., Ch. 3 — Fever (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 9 (textbook)
- Surviving Sepsis Campaign International Guidelines 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old agricultural worker from Odisha is admitted on a hot June afternoon with a temperature of 41.2°C, heart rate 132 bpm, and blood pressure 88/56 mmHg. He is confused, his skin is hot and completely dry. His fellow workers say he had been harvesting paddy for six hours in 43°C heat without shade or water. Now consider a contrasting admission the same evening: a 35-year-old woman from the same district, temperature 40.8°C, rigors, hepatosplenomegaly, and a peripheral blood smear that reveals ring-form trophozoites in red cells. Both patients have extreme pyrexia, both are critically ill — yet the mechanisms, treatments, and outcomes are entirely different. The first patient has hyperthermia — his hypothalamic thermostat is normal, overwhelmed by exogenous heat load, and his sweating mechanism has failed. The second patient has fever — her thermostat has been deliberately reset upward by cytokines released in response to a pathogen. Getting this distinction right in the first ten minutes determines whether you reach for ice packs and cool IV fluids or antimalarials. This module gives you the intellectual framework to make that distinction every time.
WHY THIS MATTERS
In India, fever is the presenting complaint in more than 40% of all outpatient and emergency department visits. It is the gateway syndrome behind malaria (an estimated 6 million cases annually), dengue (400,000–500,000 confirmed cases annually with large under-reporting), enteric fever, leptospirosis, rickettsial infections, and tuberculosis — all of which differ in their optimal treatment and carry significant mortality if mismanaged. As a final-year student and future clinician, you will encounter febrile patients every single day. The NMC competencies IM4.1 through IM4.8 represent the foundational knowledge expected of a competent junior doctor: you must understand the mechanisms well enough to recognise danger, categorise the cause, and initiate evidence-based management. This module is also the bridge to IM4.9–IM4.20, which deal with fever of unknown origin, investigations, and treatment communication — skills you cannot apply without the mechanistic bedrock laid here.
RECALL
Activate what you already know from physiology and microbiology. The hypothalamus contains the thermoregulatory centre in the preoptic area, which maintains core body temperature at 36.5–37.5°C through a tightly regulated set-point. Heat is generated by shivering thermogenesis (skeletal muscle), brown adipose tissue, and metabolic processes; heat is dissipated through radiation, convection, evaporation (sweating), and conduction. The innate immune system responds to pathogens via pattern-recognition receptors (Toll-like receptors, NOD-like receptors) that detect pathogen-associated molecular patterns (PAMPs) on bacterial cell walls, viral nucleic acids, and fungal glucans. This activation triggers a cytokine cascade dominated by TNF-α, IL-1β, and IL-6. Also recall that prostaglandin E2 (PGE2) is a key lipid mediator synthesised from arachidonic acid via cyclooxygenase-2 (COX-2), and that non-steroidal anti-inflammatory drugs (NSAIDs) and paracetamol work by inhibiting this pathway. You will need these connections throughout this module.
Fever vs Hyperthermia: Definitions and Pathophysiology
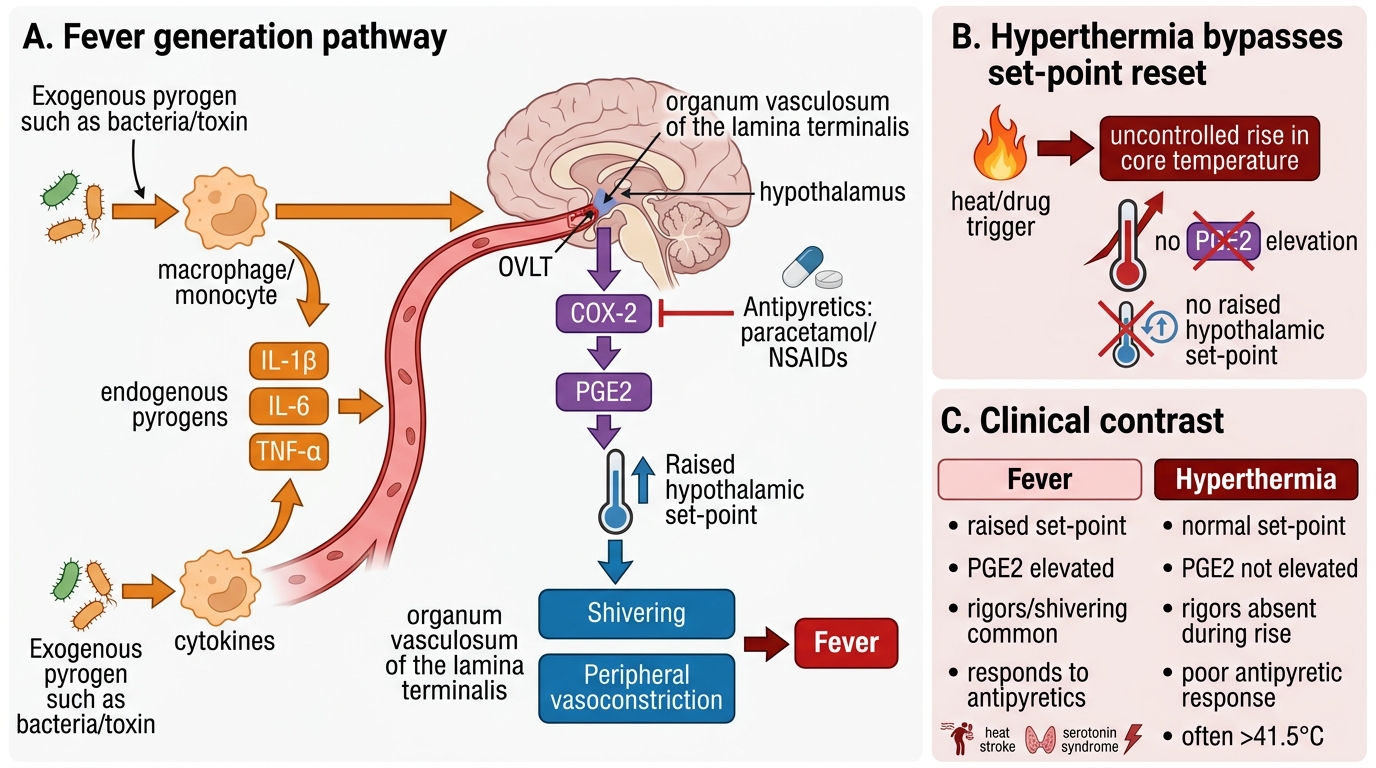
Fever (also called pyrexia) is a controlled elevation of core body temperature in which the hypothalamic set-point has been raised by endogenous pyrogens. The key distinction from hyperthermia is that in fever the thermoregulatory mechanism is intact but operating at a higher target temperature; in hyperthermia the thermoregulatory mechanism is overwhelmed or dysfunctional and temperature rises beyond any set-point. This distinction has profound clinical implications: fever responds to antipyretics (which lower the set-point back toward normal) and to treatment of the underlying cause; hyperthermia does not respond meaningfully to antipyretics and requires physical cooling as a priority.
Fever is defined as a core body temperature exceeding 38.3°C (101°F) when measured by a reliable method. Temperatures between 37.5°C and 38.3°C represent low-grade fever and warrant clinical context before labelling — they may reflect normal diurnal variation (temperature physiologically peaks at 4–6 PM), recent physical exercise, or mild inflammatory stimulus. The terms hyperpyrexia (>41°C) and extreme pyrexia (>41.5°C) denote temperatures at which direct cellular damage begins to occur, particularly in neurons, and they demand urgent attention regardless of aetiology.
The pathophysiology of fever proceeds through four sequential stages that are worth committing to memory as a narrative chain. First, an exogenous pyrogen — typically a microbial product such as lipopolysaccharide (LPS, the endotoxin of gram-negative bacteria), peptidoglycans (gram-positive), lipoteichoic acid, viral RNA, or fungal beta-glucan — is recognised by pattern-recognition receptors on monocytes, macrophages, and dendritic cells. This recognition triggers the second stage: production of endogenous pyrogens — primarily IL-1β, IL-6, TNF-α, and interferons. These cytokines reach the hypothalamus either by crossing the blood-brain barrier at specialised circumventricular organs (area postrema, organum vasculosum laminae terminalis) or by stimulating hypothalamic endothelial cells directly. In the third stage, hypothalamic COX-2 is upregulated, generating prostaglandin E2 (PGE2), which acts on EP3 receptors in the preoptic area to raise the thermoregulatory set-point. In the fourth stage, the body responds to the new (elevated) set-point through heat-conserving and heat-generating mechanisms: peripheral vasoconstriction (reduces heat loss), shivering (increases heat generation), and piloerection — the subjective sensation of chills and rigors. Once body temperature reaches the new set-point, shivering ceases and the patient feels hot rather than cold. When the stimulus resolves (or an antipyretic lowers the set-point), the body dissipates heat through sweating and vasodilation, producing the defervescence that the patient experiences as drenching sweats.
Fever Generation and Hyperthermia Contrast
Hyperthermia, by contrast, is an uncontrolled rise in core temperature due to failure of heat dissipation or overwhelming heat load, without any resetting of the hypothalamic set-point. PGE2 is NOT elevated. Causes include heat stroke (see below), malignant hyperthermia (triggered by volatile anaesthetics in genetically susceptible individuals — a mutation in the ryanodine receptor causing uncontrolled Ca²⁺ release from sarcoplasmic reticulum), neuroleptic malignant syndrome (idiosyncratic reaction to antipsychotics characterised by rigidity, hyperthermia, autonomic instability, and elevated creatine kinase), serotonin syndrome, and thyroid storm. In clinical practice, the critical differentiating features of hyperthermia from fever are: absence of response to antipyretics, absence of rigors during the temperature rise, extremely high temperatures (>41.5°C is more common with hyperthermia), and a specific causative context (heat exposure, anaesthetic, drug).
Common Causes of Fever in India: Regional and Epidemiological Context
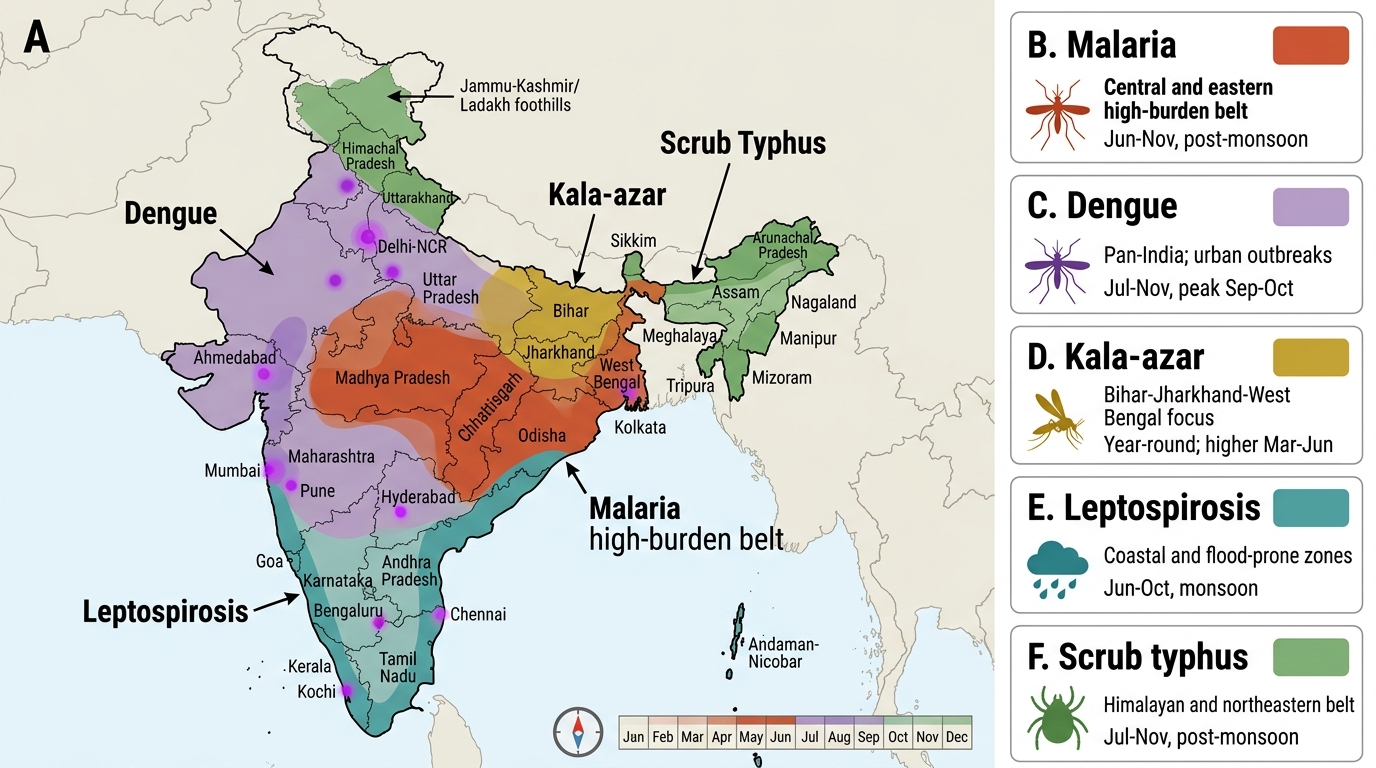
India's disease ecology creates a distinctly different spectrum of febrile illnesses compared to high-income countries. The combination of tropical and subtropical climate, variable sanitation, large agricultural workforce, and urban-rural diversity means that infectious causes dominate the differential diagnosis in a way that is not true in temperate settings. Understanding the regional distribution and seasonal patterns of fever-causing illnesses is a core competency (IM4.3) because it directly informs the probability weighting of your differential diagnosis when you examine a patient.
The most important infectious causes of fever in India, organised by category, are as follows. Among vector-borne diseases: malaria (Plasmodium vivax predominates in most of India; P. falciparum is prevalent in Odisha, Jharkhand, Chhattisgarh, northeastern states — the high-burden belt; P. malariae and P. ovale are rare but present); dengue fever (four serotypes DENV-1–4, aedes-borne, urban and periurban, monsoon and post-monsoon peak, found pan-India with Chennai, Delhi, Mumbai, Kolkata recording highest burden); chikungunya (aedes-borne, south India and Gujarat dominant historically); scrub typhus (Orientia tsutsugamushi, trombiculid mite, endemic in Himalayas, Tamil Nadu, northeastern India — significantly under-diagnosed); leptospirosis (Leptospira interrogans, flooding/occupational/animal contact, coastal India particularly Kerala, coastal Maharashtra, Gujarat, and northeastern states); rickettsial spotted fevers (tick-borne, Himalayan foothills); Kala-azar or visceral leishmaniasis (Leishmania donovani, sandfly-borne, endemic in Bihar, Jharkhand, Uttar Pradesh, West Bengal — the WHO target-elimination zone).
Among enteric and gastrointestinal causes: enteric fever (typhoid: Salmonella typhi; paratyphoid: S. Paratyphi A, B, C — endemic pan-India, fecal-oral, step-wise fever with relative bradycardia, rose spots, hepatosplenomegaly); acute viral hepatitis (hepatitis A and E cause febrile hepatitis; A and E are waterborne and endemic in low-hygiene settings); acute pyogenic diarrhoea (Salmonella, Shigella, Campylobacter). Among respiratory causes: tuberculosis (TB — NTEP; a significant cause of prolonged fever in all regions), community-acquired pneumonia (Streptococcus pneumoniae, Klebsiella, atypicals). Among non-infectious causes that must not be missed: autoimmune and inflammatory conditions (adult-onset Still's disease, SLE, rheumatoid arthritis, vasculitis), haematological malignancies (lymphoma, leukaemia), and solid tumours with paraneoplastic fever.
Geographic Distribution of Major Febrile Infections in India
The non-infectious causes of fever deserve special emphasis because they are systematically under-considered in busy fever clinics. Inflammatory and autoimmune fevers arise from the same cytokine cascade as infectious fever — IL-1β, IL-6, and TNF-α are elevated in both rheumatoid arthritis flares and bacterial infections. The clinical clue is the pattern of accompanying features: joint swelling, rash, serositis, renal involvement, and lymphadenopathy without a clear infective source should prompt autoimmune screening. Malignant fever is discussed in the next section. Drug fever is an important iatrogenic cause — sulfonamides, beta-lactams, antiepileptics, allopurinol, and many others can cause fever as part of a hypersensitivity reaction, sometimes (but not always) accompanied by rash and eosinophilia.
Inflammatory and Malignant Causes of Fever
Beyond infection, two broad non-infectious categories of fever — inflammatory/autoimmune and malignant — account for a significant proportion of hospitalised febrile patients, and both are disproportionately represented in the prolonged fever or fever of unknown origin (FUO) population. Understanding their pathophysiology explains not only the fever mechanism but also many of the accompanying systemic features that help make the diagnosis.
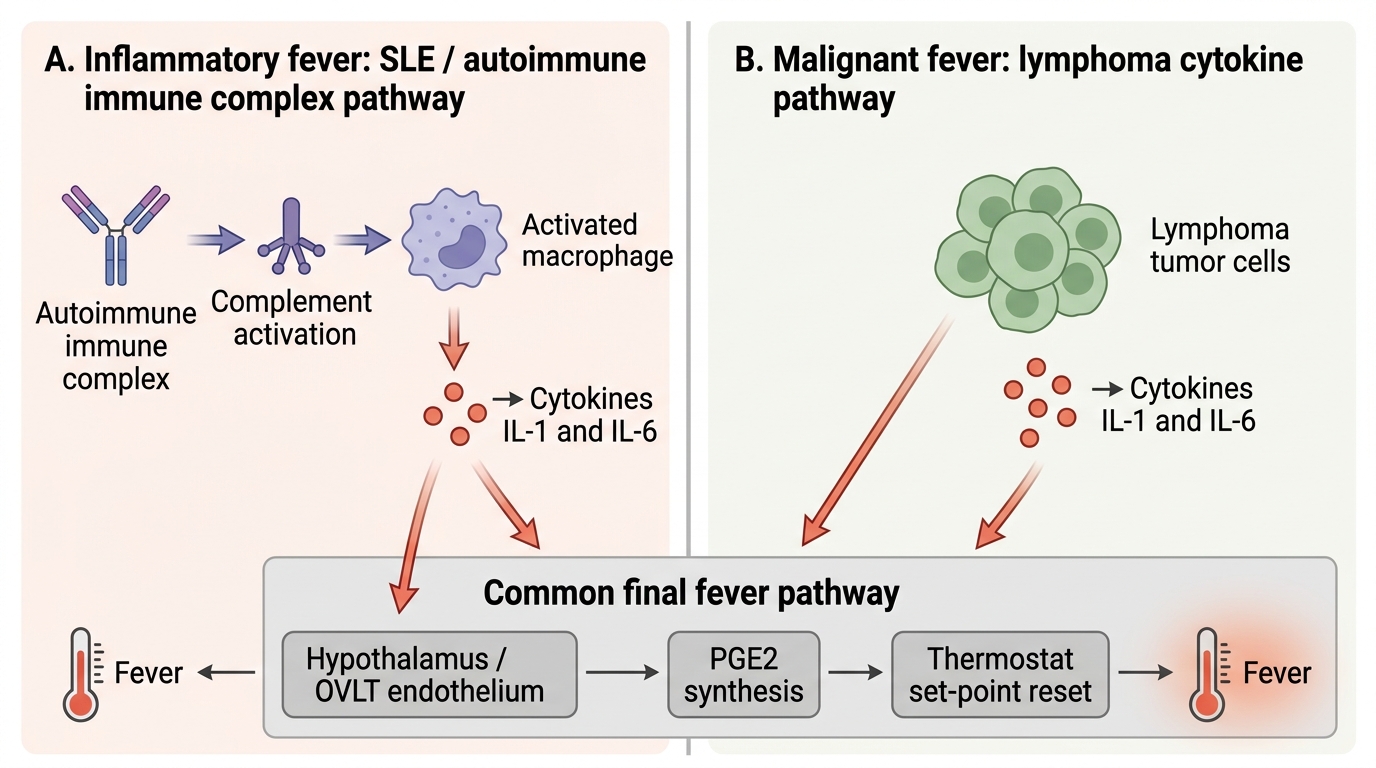
Inflammatory fever is generated by the same cytokine network as infectious fever, but the trigger is endogenous tissue damage or immune dysregulation rather than a foreign pathogen. In systemic lupus erythematosus (SLE), immune complex deposition activates complement and triggers macrophage release of IL-1β and IL-6; fever occurs during flares and may be the presenting feature before the classic malar rash and serositis become apparent. In adult-onset Still's disease (AOSD), the key cytokine driver is IL-18 in addition to IL-1β and IL-6, and the clinical triad of quotidian fever (spiking once or twice daily to >39°C and returning to normal between spikes), evanescent salmon-coloured urticarial rash (appearing during fever spikes), and arthritis is pathognomonic when present. In vasculitis (giant cell arteritis, polyarteritis nodosa, ANCA-associated vasculitis), vessel wall inflammation driven by CD4+ T-cell and macrophage activation generates a persistent febrile state that is often accompanied by constitutional weight loss, night sweats, and organ-specific ischaemic features. Fever is also prominent in haemophagocytic lymphohistiocytosis (HLH) — a life-threatening cytokine storm syndrome driven by uncontrolled macrophage and CD8+ T-cell activation, with extremely high ferritin (>10,000 ng/mL is the classical threshold), cytopenias, and multi-organ failure.
Malignant fever arises through multiple mechanisms, which is why not all malignancies cause fever equally. In haematological malignancies — particularly Hodgkin's lymphoma, non-Hodgkin's lymphoma, and acute leukaemia — fever has three contributing mechanisms: (1) direct tumour-cell production of IL-1, IL-6, and TNF-α (tumour-derived endogenous pyrogens), (2) secondary infection due to neutropenia (either from disease-mediated marrow failure or chemotherapy-induced myelosuppression), and (3) transfusion reactions or medication reactions in treated patients. The classic Pel-Ebstein fever of Hodgkin's lymphoma — alternating weeks of high fever and afebrile periods — is historically described but rare in practice. Renal cell carcinoma (RCC), hepatocellular carcinoma (HCC), and atrial myxoma are the solid tumours most classically associated with fever as a presenting or dominant feature. Fever in these solid tumours is driven by tumour necrosis, IL-6 production by tumour cells, and, in the case of atrial myxoma, repeated cytokine release from the myxoma into the circulation. Lymphadenopathy in the context of fever — particularly cervical, axillary, or mediastinal lymphadenopathy — always warrants biopsy-based investigation to exclude lymphoma before attributing fever to an infectious cause.
Inflammatory vs Malignant Fever: Common Final Pathway
A practical point: drug fever (a subset of drug hypersensitivity reactions) should always be considered in a hospitalised patient who develops or maintains fever despite appropriate antimicrobial therapy. The mechanism is T-cell mediated hypersensitivity generating IL-2, IL-4, and interferon-gamma — essentially a delayed-type (Type IV) hypersensitivity response. Fever from a causative drug typically appears 7–10 days after starting the drug (shorter on re-challenge), is not explained by the infection being treated, and may be the only manifestation (no rash in 50% of drug fever cases). Stopping the offending drug results in defervescence within 48–72 hours, which is both diagnostic and therapeutic.
SELF-CHECK
A 28-year-old patient on anti-tuberculosis therapy (isoniazid, rifampicin, pyrazinamide, ethambutol) for 3 weeks develops a temperature of 39.4°C. Sputum cultures remain positive for M. tuberculosis, but no new organisms are identified on blood culture. Serum ferritin and LDH are mildly elevated. The most likely cause of his new fever is:
A. Acquired multi-drug resistance to rifampicin
B. Drug hypersensitivity (drug fever) to one of the anti-TB medications
C. Paradoxical reaction (immune reconstitution)
D. Occult bacteraemia superimposed on TB
Reveal Answer
Answer: B. Drug hypersensitivity (drug fever) to one of the anti-TB medications
Drug fever from anti-TB medications (most commonly pyrazinamide, then rifampicin, then isoniazid) is a well-recognised complication typically appearing 7–14 days after initiation. It is driven by a Type IV (delayed) hypersensitivity reaction. The absence of new organisms on culture, absence of clinical deterioration in TB, and timing after 3 weeks make drug fever the most likely diagnosis. Paradoxical reactions (immune reconstitution inflammatory syndrome or IRIS) occur more commonly after starting antiretroviral therapy in HIV co-infection, not typically after 3 weeks of standalone anti-TB therapy without ART. The next step is sequential drug withdrawal to identify the culprit.