Page 3 of 21
IM4.1-8 | Fever Foundations — SDL Guide (Part 3)
Heat-Related Illness: Heat Cramps, Heat Exhaustion, and Heat Stroke
Heat-related illness (IM4.8) represents the spectrum of physiological derangements caused by failure to maintain thermal homeostasis in a hot environment. It is an important cause of hyperthermia — not fever — and the management differs fundamentally from the management of febrile infections. India's monsoon and pre-monsoon months (April–June) combined with outdoor occupational exposure make heat illness a significant cause of morbidity and mortality, particularly among agricultural workers, construction labourers, and pilgrims at religious gatherings.
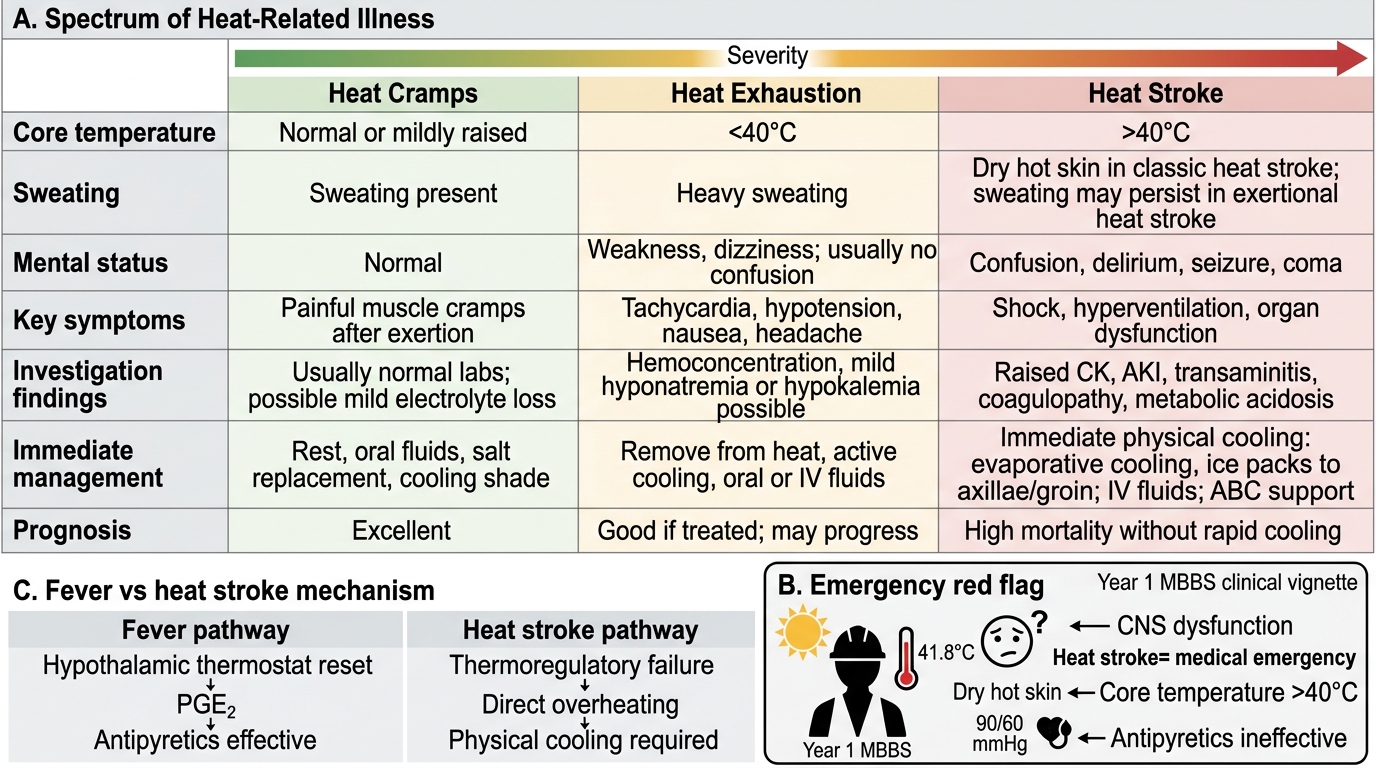
The spectrum of heat illness is best understood as a continuum of progressive thermoregulatory failure, from the relatively benign to the immediately life-threatening. Heat cramps represent the mildest form. They are painful involuntary muscle contractions occurring during or after strenuous work in a hot environment, typically affecting the calf, thigh, and abdominal muscles. The mechanism is selective electrolyte depletion — particularly sodium — due to profuse sweat-related losses that are replaced with hypotonic plain water, causing relative hyponatraemia in exercising muscles. Core temperature is normal or mildly elevated. Consciousness is fully preserved. Management: rest in a cool environment, oral rehydration with electrolyte-containing fluids (ORS or sports drinks), and avoidance of further exertion until recovery. Plain water alone may paradoxically worsen cramps by further diluting extracellular sodium.
Heat exhaustion is more significant: a syndrome of volume depletion and electrolyte loss from heavy sweating in a hot environment, with core temperature elevated but generally below 40°C. The thermoregulatory mechanism — particularly sweating — is still functioning but is overwhelmed. Clinical features include profuse sweating (skin is cool and moist, distinguishing it from heat stroke where sweating may be absent), weakness, dizziness, nausea, headache, muscle cramps, and tachycardia. Hypotension is present due to volume depletion. Sensorium is intact (the distinguishing feature from heat stroke). Laboratory findings show haemoconcentration (elevated haematocrit), hypernatraemia or hyponatraemia depending on the replacement pattern, and occasionally mild elevation of creatinine. Management: remove from heat, supine positioning, cool compresses, IV isotonic saline (0.9% NaCl) for moderate-severe cases, and oral rehydration for mild cases. Full recovery is expected within hours with appropriate treatment.
Heat stroke is a medical emergency defined by two mandatory features: (1) core temperature >40°C and (2) central nervous system (CNS) dysfunction — confusion, delirium, seizures, or coma. It represents complete failure of the thermoregulatory mechanism. Two forms are recognised: classic (non-exertional) heat stroke occurs in passive individuals — the elderly, infants, those with chronic illness — during sustained ambient heat waves (this form is characterised by absent sweating as the sweat glands are exhausted or atrophied); and exertional heat stroke (EHS) occurs in young, otherwise healthy individuals performing intense physical work in a hot, humid environment (this form often has sweating present since the heat load exceeds the capacity of an intact sweat mechanism). In both forms, at temperatures >41.5°C, direct cellular injury occurs: rhabdomyolysis (skeletal muscle breakdown with myoglobinuria and acute kidney injury), hepatocellular necrosis (elevated AST, ALT, coagulopathy), DIC, and cerebral oedema. Mortality from untreated heat stroke can exceed 50%; with immediate cooling, mortality is substantially reduced. Management is a race against time: immediate physical cooling is the priority — evaporative cooling (undressing, continuously spraying tepid water and fanning), ice packs to neck/axillae/groin, cold IV saline, or ice water immersion (most effective but requires infrastructure). Target is to reduce core temperature below 38.5°C within 30 minutes. Simultaneous supportive care: IV fluids, management of rhabdomyolysis (aggressive hydration to protect renal tubules), monitoring for DIC and hepatic failure, airway protection in unconscious patients. Antipyretics (paracetamol, NSAIDs) are NOT effective in heat stroke because the mechanism does not involve raised PGE2 or a reset set-point.
Spectrum of Heat-Related Illness
SELF-CHECK
A 60-year-old construction worker is brought to the emergency department during a June heat wave with a temperature of 41.8°C, confusion, dry hot skin, and no response to 1g IV paracetamol given by the referring clinic. His blood pressure is 90/60 mmHg. The MOST appropriate immediate intervention is:
A. IV broad-spectrum antibiotics covering gram-negative organisms
B. Immediate physical cooling (evaporative cooling, ice packs to axillae/groin)
C. Repeat IV paracetamol 1g and intravenous fluids
D. Lumbar puncture to exclude bacterial meningitis
Reveal Answer
Answer: B. Immediate physical cooling (evaporative cooling, ice packs to axillae/groin)
This is heat stroke (temperature >40°C + CNS dysfunction + dry skin = classic non-exertional heat stroke). The mechanism is NOT PGE2-mediated thermostat reset — it is direct thermoregulatory failure. Antipyretics (paracetamol, NSAIDs) are therefore ineffective, as this patient's lack of response to paracetamol already demonstrates. The priority is immediate physical cooling to reduce core temperature below 38.5°C within 30 minutes. Antibiotics are appropriate if sepsis is the cause of confusion and fever, but the combination of heat-wave context, dry skin, and failure to respond to antipyretics points to heat stroke first. Lumbar puncture is not the immediate first step in an unconscious patient before airway and temperature are stabilised.
Self-Assessment: Fever Pattern Recognition and Syndrome Integration
This self-assessment section consolidates the pathophysiology, aetiology, clinical approach, sepsis recognition, and heat illness concepts developed throughout this module. Three clinical scenarios are presented; for each, apply the framework you have learned to diagnose the syndrome and outline the initial management. Then review the analysis to check your reasoning. This mirrors the clinical-reasoning task required at the KH and SH levels of the NMC IM4.1–IM4.8 competencies — knowing the facts is necessary but not sufficient; you must be able to apply them to an unstructured patient presentation.
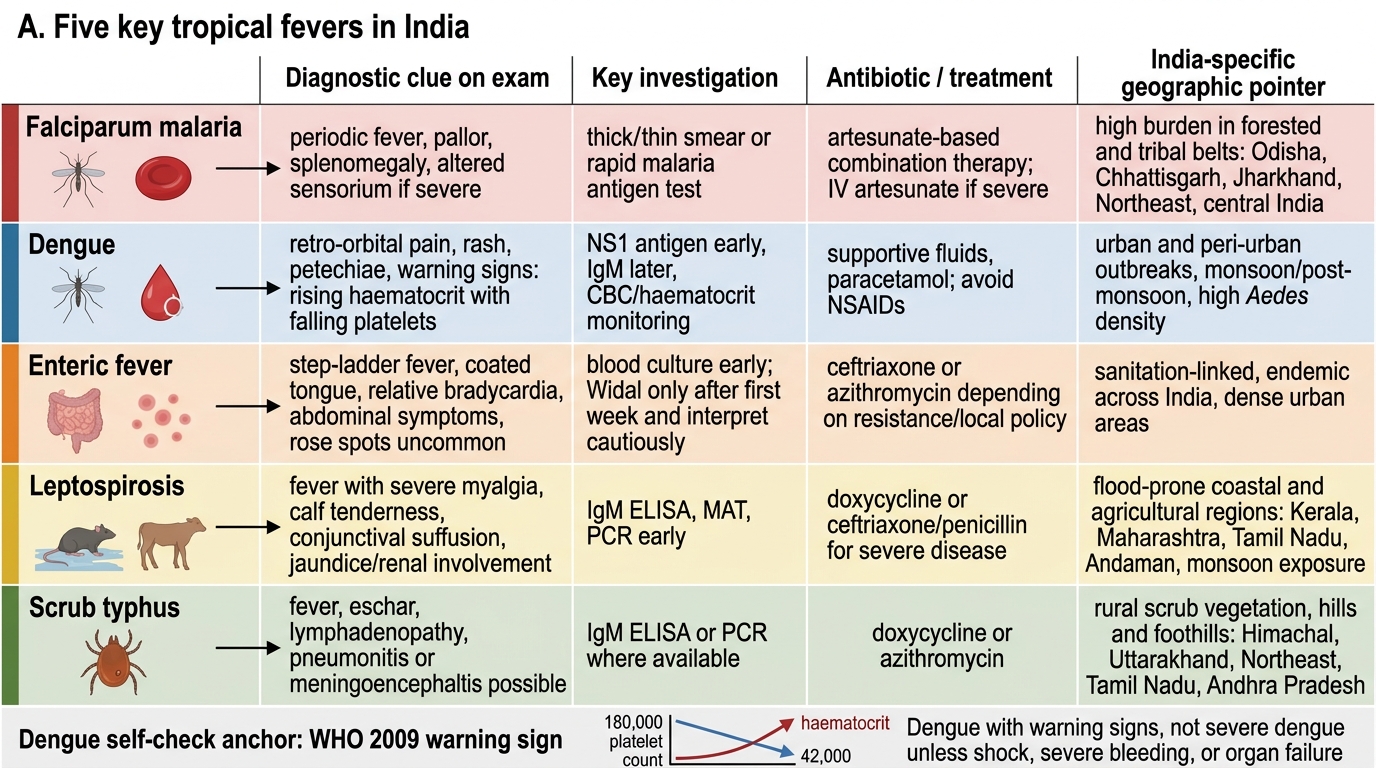
Scenario A: A 45-year-old rice farmer from Chhattisgarh presents with three episodes of high fever, each preceded by rigors and followed by drenching sweats, occurring every 48 hours for the past 10 days. He appears jaundiced with a palpable spleen 4 cm below the costal margin. His haemoglobin is 8 g/dL and peripheral smear shows ring-form trophozoites with some double-ring and banana-shaped gametocytes in red blood cells. What is the diagnosis, likely species, and immediate management priority?
Analysis: The 48-hour cycle (tertian pattern), rigors-fever-sweat cycle, splenomegaly, anaemia, and peripheral smear with multiple ring-forms per cell and banana-shaped gametocytes confirms Plasmodium falciparum malaria. The gametocytes (banana shape = P. falciparum specific), double ring forms, and the high-transmission zone (Chhattisgarh) are diagnostic. This is severe malaria (jaundice + anaemia + from a high-burden area) — the World Health Organization criteria for severe malaria include jaundice with parasitaemia. Management: IV artesunate (first-line for severe falciparum malaria; oral ACT if mild/moderate), blood transfusion for haemoglobin <7 g/dL, close monitoring for cerebral malaria, renal failure, and respiratory distress. Report to NVBDCP.
Scenario B: A 70-year-old diabetic man is brought by his family with a 3-day history of confusion, mild cough, and a temperature of 37.9°C. His family says he 'doesn't seem right'. Examination: respiratory rate 28 breaths/min, blood pressure 98/60 mmHg, oxygen saturation 88% on room air. CXR shows right lower lobe consolidation. Blood glucose is 400 mg/dL. What syndrome do you diagnose and what is the initial management hour-1 bundle?
Analysis: Despite a temperature of only 37.9°C (blunted febrile response in an elderly diabetic), this patient fulfils criteria for sepsis with pneumonia as the source: organ dysfunction (confusion, hypoxia, tachypnoea = respiratory failure, hypotension) in the context of infection. The blunted fever is a classic elderly trap. Hour-1 bundle: obtain blood cultures × 2; administer empiric antibiotics (IV co-amoxiclav + azithromycin for CAP, or based on local protocol); administer 30 mL/kg IV crystalloid (cautiously in elderly); measure and re-measure lactate; start noradrenaline if MAP remains <65 mmHg despite fluids. Insulin infusion for hyperglycaemia. CURB-65 score: 3 (confusion, urea likely elevated, RR 28, age ≥65) → hospitalisation with high-dependency consideration.
Scenario C: A 25-year-old woman returns from a monsoon trek in Uttarakhand with fever, severe myalgia, conjunctival suffusion, and jaundice appearing 10 days after her trip. She recalls wading through flooded fields. Her serum bilirubin is 4 mg/dL (predominantly direct), AST/ALT mildly elevated, creatinine 2.1 mg/dL. Chest X-ray shows bilateral patchy infiltrates. Which diagnosis is most likely, what investigation confirms it, and what antibiotic is indicated?
Analysis: Flood/water exposure + myalgia + conjunctival suffusion + hepatorenal syndrome (jaundice + rising creatinine) = leptospirosis (Weil's disease, the icteric severe form). The triad of hepatitis, nephritis, and pulmonary infiltrates in a flood-exposed individual is pathognomonic. Confirmatory investigation: MAT (microscopic agglutination test) is the gold standard; paired serology (IgM ELISA is more widely available and useful acutely). Blood and urine culture (leptospires may be cultured but slow). Antibiotic: IV benzylpenicillin 1.5 MU six-hourly, or IV ceftriaxone 1g daily (both effective for severe leptospirosis); oral doxycycline 100 mg twice daily for mild disease.
Five Key Tropical Fevers in India
SELF-CHECK
A patient presents with fever, arthralgia, retro-orbital pain, and a petechial rash appearing on day 5 of illness. His platelet count has fallen from 180,000 to 42,000 over 3 days. Haematocrit is rising. He is otherwise alert. According to WHO 2009 dengue classification, this patient is best classified as:
A. Dengue without warning signs
B. Dengue with warning signs
C. Severe dengue
D. Dengue haemorrhagic fever Grade III
Reveal Answer
Answer: B. Dengue with warning signs
WHO 2009 classification uses three categories: dengue without warning signs, dengue with warning signs, and severe dengue. Warning signs include abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation (ascites, pleural effusion), mucosal bleed, lethargy/restlessness, liver enlargement >2 cm, and laboratory: increasing haematocrit concurrent with rapid decrease in platelet count. This patient has rising haematocrit + falling platelets — a warning sign — and petechial rash (mucosal bleed is a warning sign; petechiae on skin are less clearly a warning sign but the overall picture with rising haematocrit and thrombocytopaenia = dengue with warning signs. Severe dengue requires severe plasma leakage with shock or respiratory distress, severe bleeding, or severe organ impairment. The older DHF grading (Grades I–IV) is from the 1997 classification, which has been superseded by the 2009 WHO classification.
CLINICAL PEARL
The single most dangerous mistake in evaluating a febrile patient is to treat the temperature number rather than the patient. An elderly diabetic with a temperature of 37.9°C and confusion can be in septic shock; a marathon runner with a temperature of 40.5°C after a race may simply have exertional hyperthermia requiring cooling and hydration. The clinical context — the host, the mechanism, the accompanying organ dysfunction — determines both the urgency of the response and the correct therapeutic target. Antipyretics are appropriate for fever (PGE2-mediated set-point reset) but are NOT effective and may waste critical time in hyperthermia (direct thermoregulatory failure). Always ask: is this fever, or is this hyperthermia? The answer changes everything about your management.