Page 6 of 21
IM4.{9,14,18} | Fever of Unknown Origin — SDL Guide (Part 2)
Developing a Prioritised Diagnostic Plan for FUO
The art of FUO management lies not in knowing what tests exist, but in building a sequential, hypothesis-driven diagnostic plan that is tailored to the individual patient's clinical picture, host context, and epidemiological background. NMC competency IM4.18 requires the student to demonstrate exactly this skill: to develop and present an appropriate diagnostic plan based on clinical presentation, most likely diagnosis, in a prioritised and cost-effective manner. The following framework operationalises this competency.
Step 1 — Exclude treatable causes that require urgent action regardless of diagnostic certainty. Before any stepwise investigation, ask: could this patient have infective endocarditis (new murmur + bacteraemia risk factors + embolic features)? Could this be TB meningitis (fever + headache + signs of meningism)? Could this be neutropenic sepsis (check the ANC)? Could this be HIV (universal screen)? These conditions are dangerous enough that empiric or urgent intervention may be needed before the full diagnostic workup is complete. HIV should be checked in every single FUO patient without exception — there is no threshold of perceived risk below which HIV screening can be omitted.
Step 2 — Review the clinical clues systematically. Before ordering additional investigations, examine every available piece of clinical data with fresh eyes: (a) the fever pattern — continuous, remittent, intermittent, or quotidian? Step-ladder fever with relative bradycardia = typhoid until proved otherwise; quotidian double-spike = Still's disease; hectic/sweating fever with rigors = abscess or endocarditis; (b) the physical examination — every lymph node station, every murmur, every skin lesion (rose spots, eschar of scrub typhus, Janeway lesions, Osler nodes), fundoscopy (choroidal tubercles, Roth spots of endocarditis, cotton-wool spots of HIV retinopathy), hepatosplenomegaly magnitude and character, and joint examination; (c) the prior investigation results — are blood cultures truly adequate (3 sets, 5–14 days incubation)? Was the Mantoux read at 48–72 hours? Was the echocardiogram transoesophageal if transthoracic quality was inadequate?
Step 3 — Generate a hypothesis-ranked differential diagnosis. Based on the clinical review, rank the top 3–5 diagnoses in order of (a) probability (most likely given the epidemiological context), (b) danger (most life-threatening if missed), and (c) treatability (those with effective targeted therapy take investigative priority). In an Indian patient: TB (probability + treatability), kala-azar (endemic zone + probability), lymphoma (danger), and Still's disease (probability + treatability) would typically lead the differential in a non-specific presentation.
Step 4 — Design a tiered investigation plan. Investigations should be organised into tiers: Tier 1 (broadly available, inexpensive, safe, and informative regardless of specific hypothesis) → Tier 2 (more specific, higher cost or risk, ordered when Tier 1 is non-diagnostic and a specific hypothesis remains) → Tier 3 (invasive, expensive, or available only at tertiary centres — bone marrow biopsy, PET-CT, liver biopsy, temporal artery biopsy). Tier 1 includes: complete blood count with differential and peripheral smear, CRP/ESR/LDH/ferritin/albumin, blood cultures × 3 (held ≥5 days), urine analysis and culture, chest X-ray (both PA and lateral), ultrasound abdomen and pelvis (identifies organomegaly, lymphadenopathy, abscesses), HIV Ag/Ab, and thyroid function tests (thyroiditis can cause fever). Tier 2 includes: CT chest/abdomen/pelvis with contrast (lymphadenopathy, occult malignancy, abscess), echocardiography (endocarditis, atrial myxoma), ANA/anti-dsDNA/ANCA/RF panel, serology panel (Brucella SAT, Widal, EBV VCA IgM, CMV IgM, rK39), IGRA/Mantoux, and bone marrow aspirate and biopsy if haematological malignancy, TB, or kala-azar is suspected.
Step 5 — Avoid empiric antibiotic or steroid therapy until a diagnosis is established. This is the cardinal principle of FUO management. Empiric broad-spectrum antibiotics (without a microbiological target) mask cultures, generate resistance, and delay the true diagnosis. Empiric corticosteroids for suspected autoimmune FUO are particularly dangerous — if the cause is in fact TB or kala-azar, steroids will suppress the immune response and cause catastrophic worsening. The exception is clinical deterioration demanding immediate empiric action (e.g., suspected temporal arteritis with imminent visual loss, or TB meningitis with rapidly deteriorating consciousness). Where empiric anti-TB therapy must be started before microbiological confirmation, a formal decision and documentation justifying this step is required, because the therapeutic response (defervescence within 2 weeks on anti-TB therapy) becomes part of the diagnostic logic.
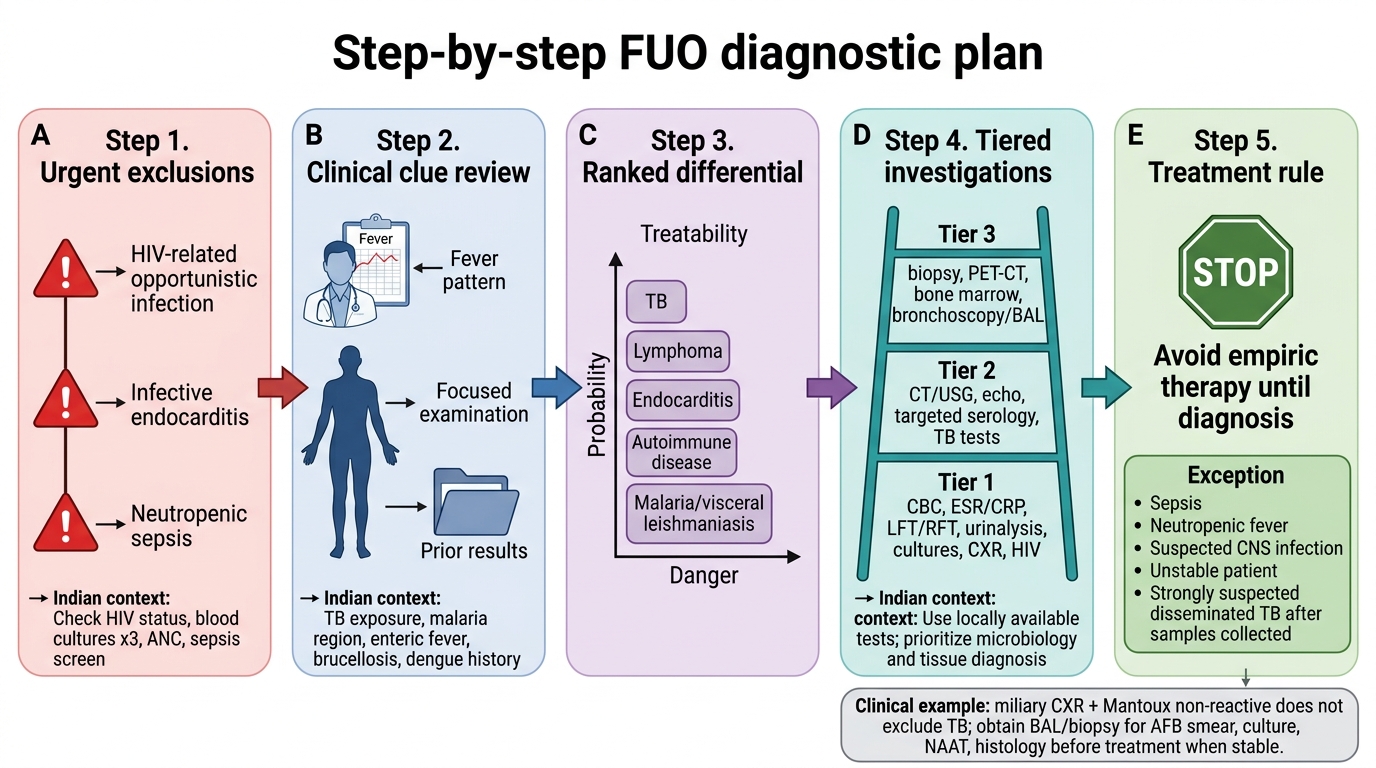
Five-Step Diagnostic Plan for Fever of Unknown Origin
SELF-CHECK
A 55-year-old immunocompetent man has had fever for 5 weeks (38.5–39.5°C), weight loss of 6 kg, and night sweats. ESR is 110 mm/hour, CRP 78 mg/L, LDH 420 U/L, and haemoglobin 9.8 g/dL. Blood cultures × 3 sets (held 7 days) are negative. Chest X-ray shows bilateral fine nodular shadowing described as 'miliary pattern'. Mantoux test is 3 mm (non-reactive). The MOST appropriate next step is:
A. Prescribe empiric anti-TB therapy (2HRZE) and review in 2 weeks
B. Order ANA and anti-dsDNA to evaluate for SLE
C. Bronchoscopy with BAL for AFB smear/culture and transbronchial biopsy
D. Proceed to echocardiography for infective endocarditis
Reveal Answer
Answer: C. Bronchoscopy with BAL for AFB smear/culture and transbronchial biopsy
The clinical and radiological picture (prolonged fever, constitutional symptoms, miliary CXR pattern, anaemia, markedly elevated ESR) is highly consistent with miliary tuberculosis. The non-reactive Mantoux does NOT exclude TB — in miliary TB (and other forms of severe/disseminated TB), anergy (immune exhaustion) commonly produces a false-negative tuberculin test because the CD4+ T-cell response is overwhelmed by the bacillary load. Bronchoscopy with BAL for AFB smear and culture plus transbronchial biopsy (demonstrating caseating granulomas) is the appropriate next step to obtain a tissue diagnosis before starting anti-TB therapy. Empiric anti-TB without microbiological confirmation should be avoided unless the patient is clinically deteriorating and invasive diagnosis cannot be obtained promptly. SLE rarely causes a miliary CXR pattern. Endocarditis is not the primary consideration.
Self-Assessment: FUO Diagnostic Reasoning
These clinical scenarios test your ability to apply the FUO framework — definition, differential, and diagnostic plan — developed in this module. For each, read the vignette, formulate a ranked differential, identify the key investigation, and then review the analysis. This is the clinical reasoning skill that NMC competency IM4.18 demands.
Scenario A: A 44-year-old man from Uttar Pradesh has had fever for 7 weeks (38.5–40°C), progressive hepatosplenomegaly (liver 4 cm, spleen 16 cm below the costal margin), haemoglobin 7 g/dL, WBC 2,800 cells/mm³ (neutrophils 60%), platelets 88,000/mm³, total protein 10.2 g/dL (albumin 2.4 g/dL, globulin 7.8 g/dL). He is from an area where kala-azar was endemic until recently. The rK39 rapid test is performed and is positive. What is the diagnosis, what additional test confirms it, and what is the first-line treatment in India?
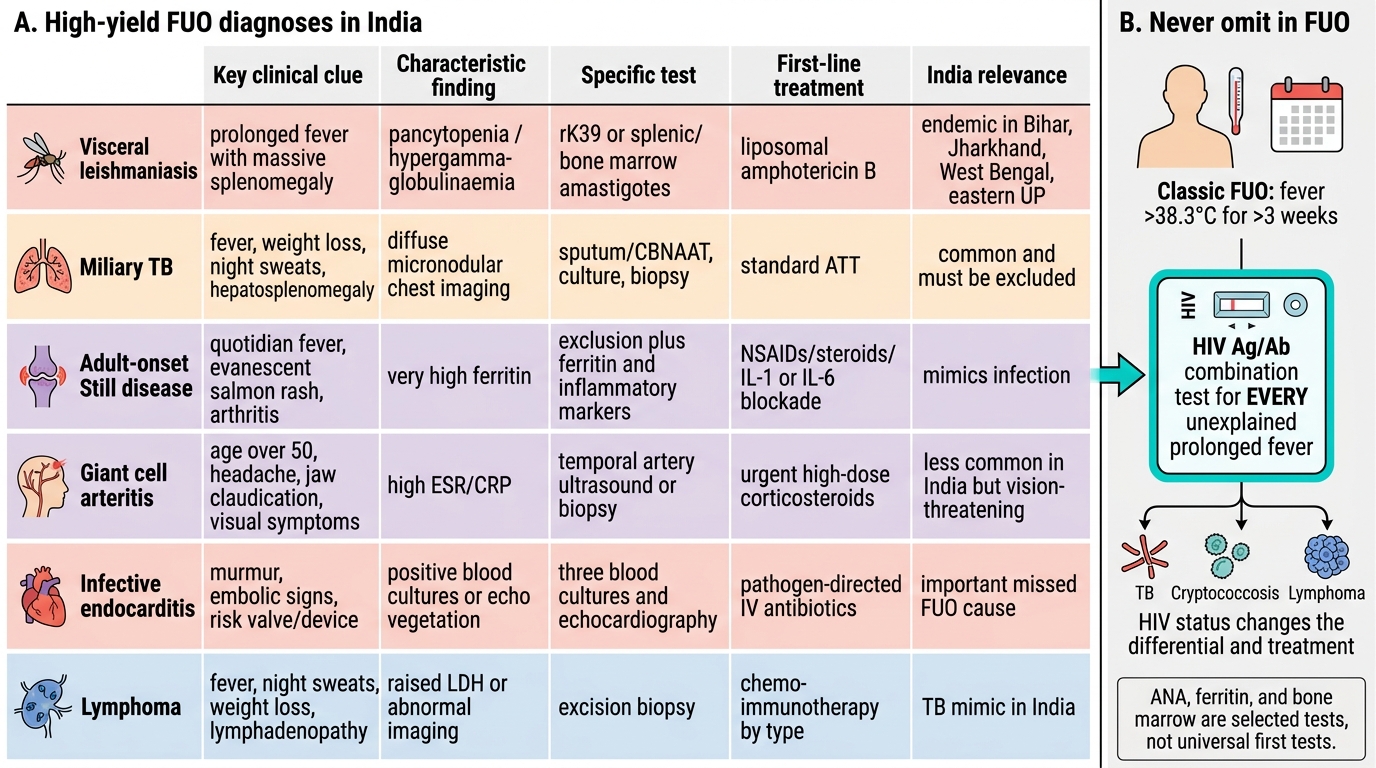
Analysis: This is visceral leishmaniasis (kala-azar) — the triad of prolonged fever, progressive massive splenomegaly, and pancytopaenia with polyclonal hypergammaglobulinaemia in an endemic-zone patient is pathognomonic. The rK39 positive result clinches the diagnosis serologically. Bone marrow aspiration for Leishman-Donovan body (amastigotes in macrophages) is the confirmatory investigation and remains the gold standard. First-line treatment in India under the NVBDCP (National Vector Borne Disease Control Programme) kala-azar elimination programme: liposomal amphotericin B (a single infusion of 10 mg/kg; the preferred first-line agent due to its high cure rate and tolerability) replacing the older miltefosine and paromomycin. Miltefosine (oral) is also effective as an alternative.
Scenario B: A 28-year-old woman has had fever for 4 weeks with arthralgia in the wrists and knees, a salmon-coloured urticarial rash appearing in the evenings during fever spikes, sore throat, and lymphadenopathy. WBC 22,000/mm³ with 88% neutrophils. Serum ferritin is 14,200 ng/mL. ANA is negative. RF is negative. Blood cultures and malaria RDT are negative. What is the likely diagnosis and how is it established?
Analysis: This is adult-onset Still's disease (AOSD). The classic features are all present: quotidian fever spiking to >39°C, evanescent salmon-coloured urticarial rash appearing synchronously with fever, arthritis/arthralgia, sore throat, lymphadenopathy, leucocytosis with neutrophilia, and — most specifically — markedly elevated serum ferritin (>10,000 ng/mL). AOSD is diagnosed by the Yamaguchi criteria (major: fever ≥39°C for ≥1 week, arthralgia ≥2 weeks, typical rash, leucocytosis ≥10,000/mm³ with ≥80% granulocytes; minor: sore throat, lymphadenopathy, hepatosplenomegaly, abnormal LFTs, negative ANA and RF) — diagnosis requires 5 criteria (at least 2 major) after excluding infections, malignancy, and other autoimmune diseases. Treatment: NSAIDs for mild disease; methotrexate and corticosteroids for moderate-severe; IL-1 blockers (anakinra, canakinumab) for refractory cases.
Scenario C: A 67-year-old man has had fever for 3 weeks, new temporal headache, jaw claudication, and shoulder girdle aching. ESR is 96 mm/hour, CRP 44 mg/L. Visual acuity is normal. What is the diagnosis, what investigation confirms it, and what must be done immediately if this diagnosis is confirmed?
Analysis: This is giant cell arteritis (GCA) — temporal arteritis. The classic triad of temporal headache, jaw claudication, and polymyalgia rheumatica (shoulder girdle aching) in a >50-year-old with markedly elevated ESR is characteristic. The key danger is ischaemic optic neuropathy leading to blindness — which can occur abruptly without warning. Confirmatory investigation: temporal artery biopsy (demonstrating transmural granulomatous inflammation with giant cells); however, biopsy should NOT delay treatment. Immediate management: high-dose corticosteroids (prednisolone 40–60 mg/day, or IV methylprednisolone 1g/day × 3 days if visual symptoms are present or threatened) must be started immediately to prevent visual loss. The biopsy can still be positive for up to 1–2 weeks after starting steroids.
High-Yield FUO Diagnoses in India
SELF-CHECK
In the diagnostic workup of a 40-year-old with classic FUO (fever 38.5°C for 4 weeks, undiagnosed after 3 outpatient visits), which single investigation should NEVER be omitted regardless of perceived risk profile?
A. Anti-nuclear antibody (ANA)
B. Serum ferritin
C. HIV Ag/Ab combination test
D. Bone marrow aspiration
Reveal Answer
Answer: C. HIV Ag/Ab combination test
HIV Ag/Ab combination test (or HIV ELISA) must be performed in EVERY patient with unexplained prolonged fever, without exception and without risk stratification. HIV is prevalent, treatable, and — critically — profoundly changes the differential diagnosis and management of FUO. Missing HIV co-infection in a patient with TB, cryptococcosis, or lymphoma can result in fatally inadequate treatment. ANA is appropriate when autoimmune aetiology is clinically suspected but is not universally mandatory. Serum ferritin is a useful adjunct but not a universal mandatory test. Bone marrow aspiration is a second-tier investigation with specific indications (suspected haematological malignancy, miliary TB, kala-azar, HLH) — not universally required in every FUO.
CLINICAL PEARL
In India, the three diagnoses that must be actively excluded in every patient with classic FUO — regardless of how atypical the presentation appears — are tuberculosis (especially extrapulmonary), visceral leishmaniasis (in endemic zones), and HIV disease. These three causes are common, have effective targeted treatments, and are fatally easy to miss if not specifically sought. A non-reactive Mantoux does NOT exclude TB in a severely ill patient with miliary shadowing — anergy from immunological exhaustion is well-documented in disseminated TB. Similarly, a negative rK39 test does not exclude kala-azar in a low-parasitaemia patient — bone marrow aspiration may be needed. And there is no clinical risk profile below which HIV testing can be considered unnecessary.