Page 8 of 19
IM5.11-14 | Liver Disease Diagnostic Testing — SDL Guide
Learning Objectives
- Choose and interpret appropriate liver function tests (CBC, bilirubin, ALT, AST, ALP, GGT, albumin, INR) using a pattern-based approach to identify hepatocellular vs cholestatic vs mixed vs isolated hyperbilirubinaemia
- Interpret hepatitis serology for HBV (HBsAg, anti-HBc IgM, HBeAg, HBV DNA, anti-HBs) and HCV (anti-HCV, HCV RNA) in the context of acute, chronic, and resolved infection
- Perform and interpret ascitic fluid analysis including SAAG calculation (same-day samples), PMN threshold for SBP (≥250/mm³), and cell differential for TB vs malignant vs portal hypertension ascites
- Enumerate indications for ultrasound, MRCP, and ERCP and describe key findings for each modality in common liver diseases
- Apply a stepwise diagnostic algorithm for liver disease based on LFT pattern, hyperbilirubinaemia type, serology, and imaging
INSTRUCTIONS
This is an interpretation-focused module. Work through the numerical examples and scenarios — do not just read the text passively. Calculate the SAAG from the given values, score the LFT pattern on the provided cases, and interpret the serology tables before checking the answers. The skill assessed here is SH — you are expected to interpret these results at the bedside, not merely describe how to do so.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 328 and Ch. 345 — Liver Function Tests; Approach to the Patient with Liver Disease (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 22 — Investigation of Liver Disease (textbook)
- API Textbook of Medicine, 10th ed. — Diagnostic Approach to Liver Disease (textbook)
- EASL Clinical Practice Guidelines on the Management of Ascites, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
The results printout arrives: bilirubin 4.8 mg/dL, ALT 1,240 IU/L, AST 610 IU/L, ALP 180 IU/L, albumin 3.2 g/dL, INR 1.6. The nurse has also handed you the ascitic fluid results from the diagnostic tap you assisted with earlier: total protein 12 g/L, albumin 4 g/dL, PMN count 180 cells/mm³, culture pending. You now need to answer three questions for the consultant's ward round in 30 minutes: What does this pattern of liver function tests tell you about the diagnosis? What does the ascitic fluid tell you about the cause of the ascites and whether the patient needs treatment now? And what imaging should you request, and in what order? This module is about answering exactly those questions — reading the investigations of liver disease with precision and clinical purpose.
WHY THIS MATTERS
Diagnostic testing in liver disease is the bridge between clinical suspicion and confirmed diagnosis. The competencies IM5.11–IM5.14 span from choosing and interpreting standard blood tests (LFTs, CBC, hepatitis serology, ascitic fluid analysis) to understanding the indications and findings of liver imaging (ultrasound, MRCP, ERCP) and applying a systematic diagnostic algorithm based on the biochemical pattern. These competencies are assessed at SH (skill-based interpretation) and KH (knowledge of indications) levels. Being able to correctly interpret a set of liver function tests, read ascitic fluid results, and choose the right imaging modality in the right sequence is a core final-year clinical skill that determines patient management.
RECALL
Before proceeding, recall the liver enzymes and what their elevation signifies. ALT (alanine aminotransferase) is most concentrated in the hepatocyte cytoplasm — its elevation indicates hepatocyte injury or necrosis. AST (aspartate aminotransferase) is present in hepatocytes as well as cardiac muscle, skeletal muscle, and red cells — less specific for liver. ALP (alkaline phosphatase) is found in bile canaliculi, bone, placenta, and intestine — hepatic ALP elevates with bile duct injury or cholestasis; bone ALP elevates with bone disease and growth. GGT (gamma-glutamyl transferase) is sensitive and hepatocyte/bile duct specific (not bone) — used to confirm hepatic origin of ALP elevation. Albumin and INR reflect hepatic synthetic function — they fall only when significant hepatocyte mass is lost. The reference values: ALT/AST normal ≤40–55 IU/L; ALP normal 40–130 IU/L; bilirubin normal ≤1.2 mg/dL; albumin 3.5–5.0 g/dL; INR normal 0.9–1.1.
Clinical Indication and Selection of Diagnostic Tests
Choosing appropriate investigations for liver disease requires matching the diagnostic question — derived from the clinical evaluation — with the specific test that most efficiently answers it. A poorly chosen investigation panel wastes resources, generates incidental results that distract from the diagnosis, and delays definitive testing. The key to appropriate test selection is understanding what each test measures and under what circumstances it is informative. This module addresses the four categories of investigation specified by the NMC IM5.11–IM5.14 competencies: full blood count and liver function tests, hepatitis serology, ascitic fluid examination, and liver imaging. Each category answers a different diagnostic question — LFTs tell you the pattern and severity of hepatic injury; serology tells you the viral aetiology; ascitic fluid tells you the mechanism of ascites and whether it is infected; imaging tells you the structural anatomy. No single category is sufficient alone, and the skill lies in selecting them in the right sequence for the clinical presentation at hand.
The clinical contexts that trigger each category of investigation:
- Full blood count (CBC) and liver function tests (LFTs): First-line in any patient presenting with jaundice, right upper quadrant pain, unexplained fatigue, known liver disease monitoring, or incidental abnormal LFTs. The CBC provides complementary diagnostic information: macrocytosis (MCV >100 fL) in alcoholic liver disease (folate deficiency, alcohol directly suppressing erythropoiesis, and liver disease); thrombocytopaenia as an early marker of hypersplenism in portal hypertension; anaemia (haemolytic in Wilson disease or autoimmune hepatitis, or from GI bleeding in cirrhosis); leucocytosis in ascending cholangitis, liver abscess, or SBP. The LFTs must always be interpreted as a panel, never in isolation — the pattern of elevation (hepatocellular vs cholestatic vs mixed) is more informative than any single value.
- Hepatitis serology: Ordered when the LFT pattern suggests acute or chronic hepatocellular injury without an obvious non-viral aetiology (no alcohol history, no hepatotoxic drug, no obstructive features). Also ordered for all patients with cirrhosis of unknown cause, for screening in high-risk populations, and for disease monitoring in known chronic hepatitis.
- Ascitic fluid examination (diagnostic paracentesis): Indicated in any patient with new-onset ascites, any existing cirrhotic with ascites who develops fever, abdominal pain or tenderness, worsening encephalopathy, or rapid clinical deterioration — clinical scenarios where SBP must be actively excluded. Diagnostic paracentesis is safe, minimally invasive, and provides diagnostically essential information that cannot be obtained non-invasively.
- Imaging (ultrasound, MRCP, ERCP, CT): Indicated for aetiological workup, assessment of portal hypertension and structural complications, characterisation of focal lesions, and guided intervention. Ultrasound is almost always the first imaging modality in liver disease — it is widely available, inexpensive, does not use ionising radiation, and provides high-yield information about hepatic echotexture, biliary dilatation, portal vein diameter, and ascites.
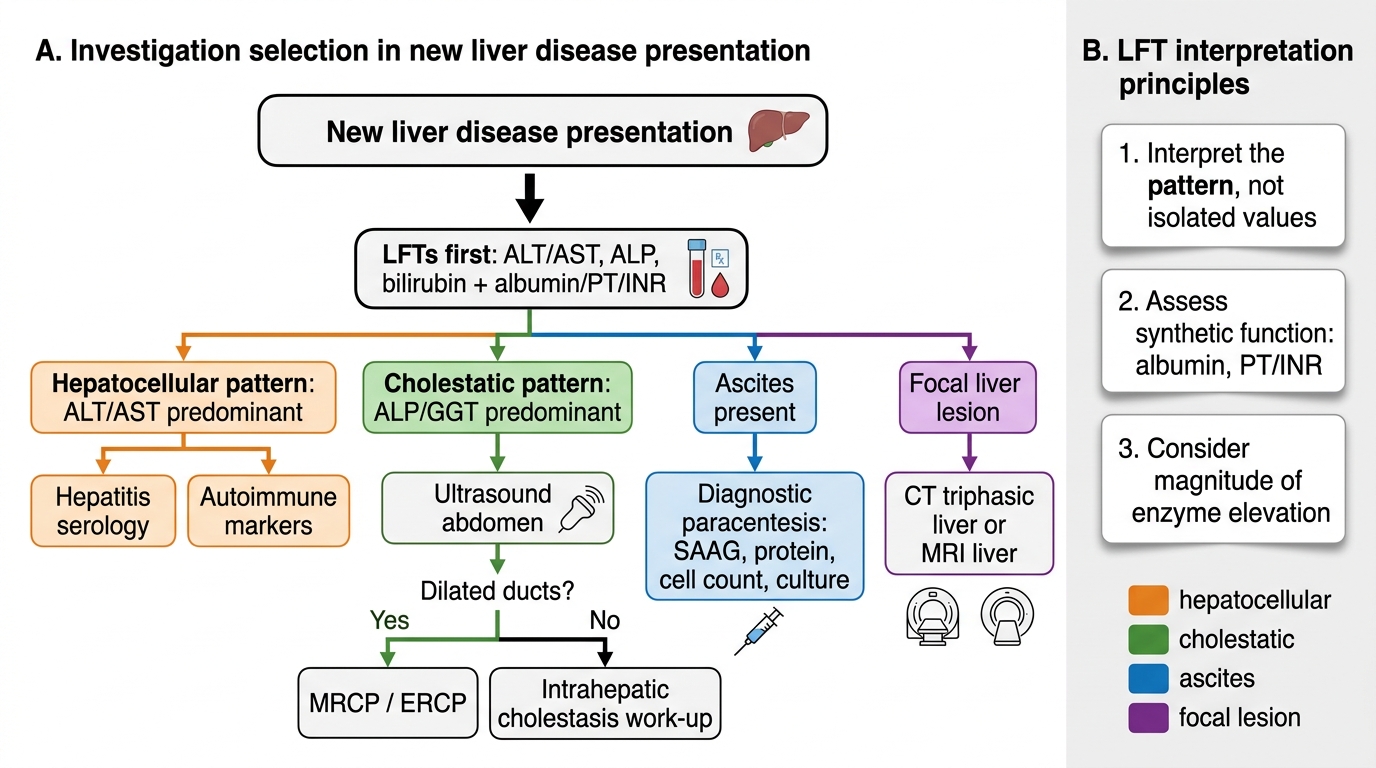
Investigation Pathway for New Liver Disease Presentation
Governing Principles of Liver Function Test Interpretation
The liver function test panel is not a single measurement but a multi-dimensional biochemical map of hepatic health. Three governing principles make this map readable: first, interpret the pattern of LFT abnormalities rather than individual values; second, always assess synthetic function alongside the enzyme pattern because synthetic failure changes the urgency of every management decision; and third, consider the magnitude of enzyme elevation alongside the pattern because the degree of elevation carries prognostic and aetiological weight.
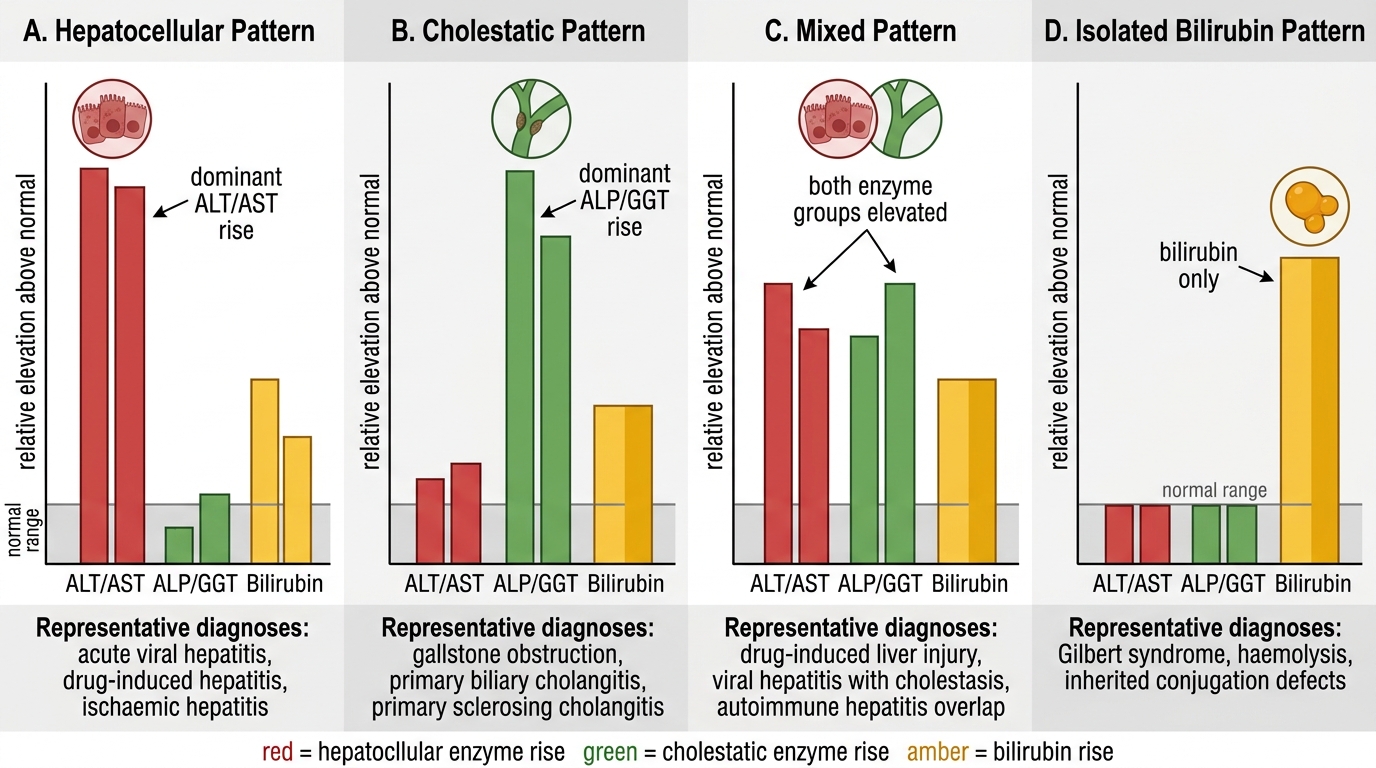
The pattern-based approach distinguishes four archetypal LFT patterns, each pointing toward a different category of liver pathology:
1. Hepatocellular pattern: Predominantly elevated ALT and AST (typically >3× ULN, often much higher); ALP ≤3× ULN; bilirubin elevated in proportion to severity of hepatocyte loss. This pattern reflects direct hepatocyte injury and is caused by viral hepatitis (acute — ALT often 10–100× ULN; chronic — ALT 1–5× ULN), alcoholic hepatitis (AST:ALT >2:1, both typically 2–10× ULN), NAFLD (ALT mildly elevated, AST:ALT usually <1), paracetamol toxicity (ALT dramatically elevated, >100× ULN is not uncommon in severe overdose), ischaemic hepatitis (ALT may reach 50–100× ULN acutely, then falls rapidly), autoimmune hepatitis (marked elevation), and Wilson disease.
2. Cholestatic pattern: Predominantly elevated ALP and GGT (ALP >3× ULN); ALT and AST ≤3× ULN; bilirubin elevated (mainly direct/conjugated). This pattern reflects obstruction to bile flow — either within the liver (intrahepatic cholestasis: primary biliary cholangitis, drug-induced cholestasis, sclerosing cholangitis) or in the bile ducts (extrahepatic obstruction: choledocholithiasis, pancreatic head carcinoma, cholangiocarcinoma). GGT is important here: if ALP is elevated but GGT is normal, the source is likely bone, not liver.
3. Mixed pattern: Both transaminases and ALP elevated significantly; seen in acute viral hepatitis with cholestatic component, drug reactions, early biliary obstruction before transaminases resolve, and certain infiltrative diseases (sarcoidosis, lymphoma).
4. Isolated hyperbilirubinaemia with normal enzymes: Bilirubin elevated but ALT, AST, ALP all normal. This pattern suggests: (a) unconjugated (indirect) hyperbilirubinaemia with normal direct fraction = pre-hepatic cause (haemolysis — check CBC with reticulocyte count, peripheral blood film, haematological screen) or Gilbert syndrome (mild unconjugated hyperbilirubinaemia worsening with fasting/illness — benign UGT1A1 polymorphism, no treatment); (b) isolated direct hyperbilirubinaemia with normal enzymes = Dubin-Johnson syndrome or Rotor syndrome (benign conjugated transport defects).
Synthetic function assessment: Two parameters must always be included: serum albumin (t½ ~20 days — reflects longer-term synthetic capacity; low in cirrhosis or prolonged severe hepatitis) and INR/prothrombin time (t½ of clotting factors II, VII, IX, X = hours to days — reflects acute synthetic function; prolongs early in acute liver failure). A patient with elevated enzymes but normal albumin and INR has preserved synthetic function and is much less concerning than one with the same enzyme elevation plus low albumin and prolonged INR.
LFT Pattern Reference Diagram
Hepatitis Serology: Interpretation of HBV and HCV Markers
Hepatitis serology is the key aetiological investigation for viral liver disease, but its interpretation requires understanding the temporal dynamics of each serological marker — when it appears, when it peaks, and when it clears — because the pattern of markers present at any given time determines the diagnosis, stage, and infectivity status. The two clinically critical serological sequences to master are for HBV (a DNA virus with multiple antigens and antibodies) and HCV (an RNA virus where the distinction between past and active infection depends on a specific test sequence). The common error in hepatitis serology interpretation is treating any single marker in isolation: HBsAg positivity without HBeAg and HBV DNA tells you infection exists but not whether it is replicating; anti-HCV positivity without HCV RNA tells you the patient was exposed but not whether they are currently infected. Every serological result must be interpreted as part of a panel, and the temporal context — acute presentation versus incidental finding — determines which markers matter most in that encounter.
HBV serological markers and their interpretation:
- HBsAg (hepatitis B surface antigen): The first marker to appear in acute HBV infection (from ~week 2–6 post-exposure) and the defining marker of current HBV infection. Present in both acute and chronic HBV. Its persistence beyond 6 months = chronic HBV infection. Its clearance = HBV resolution (followed by appearance of anti-HBs). A critical principle: HBsAg positivity means the person is currently infected and potentially infectious, regardless of how they feel.
- Anti-HBc (antibody to hepatitis B core antigen): The core antigen (HBcAg) is an intracellular antigen of HBV — it is never measured directly in blood, but the antibody to it is detectable in serum. Anti-HBc IgM appears early in acute HBV (weeks 1–2 of symptoms) and is the most sensitive marker of acute HBV infection — it remains positive for 6–12 months. It is the diagnostic marker to order when acute HBV is suspected but HBsAg may be in the 'window period' (declining) or already cleared. Anti-HBc IgG (total anti-HBc) persists lifelong after HBV infection — its presence indicates prior or current HBV exposure. It is positive in acute HBV, chronic HBV, and resolved HBV (combined with anti-HBs). Isolated total anti-HBc (with negative HBsAg and negative anti-HBs) = either remote resolved infection with waned anti-HBs, or occult HBV infection — a low-level HBV state that may reactivate with immunosuppression.
- HBeAg (hepatitis B e-antigen): A marker of active viral replication and high infectivity. Present during the high-replication phase of acute HBV and in HBeAg-positive chronic HBV. Its clearance (HBeAg seroconversion to anti-HBe) marks transition to a lower-replication phase in chronic HBV — a therapeutic goal for antiviral treatment. Anti-HBe positivity = seroconverted, lower replication state (though HBe-negative chronic HBV can still have high HBV DNA through precore/core promoter mutations).
- HBV DNA (quantitative PCR): The gold standard for measuring viral replication in chronic HBV. Expressed in IU/mL. High HBV DNA indicates active viral replication; used to guide treatment decisions and monitor antiviral therapy response.
- Anti-HBs (surface antibody): Appears after HBsAg clearance (resolved infection) or after successful HBV vaccination. Its presence alone (without anti-HBc) = vaccine-induced immunity. Anti-HBs >10 mIU/mL = protective.
Diagnostic pattern summary for HBV:
| HBsAg | Anti-HBc IgM | Total Anti-HBc | Anti-HBs | HBeAg | Interpretation |
|---|---|---|---|---|---|
| + | + | + | − | +/− | Acute HBV infection |
| + | − | + | − | + | Chronic HBV, high replication |
| + | − | + | − | − | Chronic HBV, low replication (check HBV DNA) |
| − | − | + | + | − | Resolved/past HBV infection |
| − | − | − | + | − | Vaccination (anti-HBc absent) |
| − | − | + | − | − | Isolated anti-HBc (occult HBV or waned anti-HBs) |
HCV serological sequence:
- Anti-HCV (ELISA/CMIA): A screening test for exposure to HCV. It detects antibodies to HCV antigens (core, NS3, NS4, NS5). It becomes positive 4–10 weeks after acute HCV exposure (seroconversion window). Crucially, anti-HCV remains positive lifelong — both in active HCV infection AND in past resolved HCV infection. Anti-HCV positivity therefore cannot distinguish current from past infection.
- HCV RNA (quantitative RT-PCR): The definitive test for active HCV infection. HCV RNA is detectable within 1–2 weeks of acute infection — earlier than anti-HCV. It is the confirmatory test for all anti-HCV positive patients. HCV RNA positive = active infection (requires treatment). HCV RNA negative + anti-HCV positive = past resolved infection (no antiviral treatment needed). This two-step sequence (anti-HCV → confirm with HCV RNA) is the universal standard for HCV diagnosis.
- There is no HCV antigen/antibody that indicates chronicity by itself; the distinction between chronic (>6 months of RNA positivity) and acute (<6 months) is made by serial testing rather than a single marker.
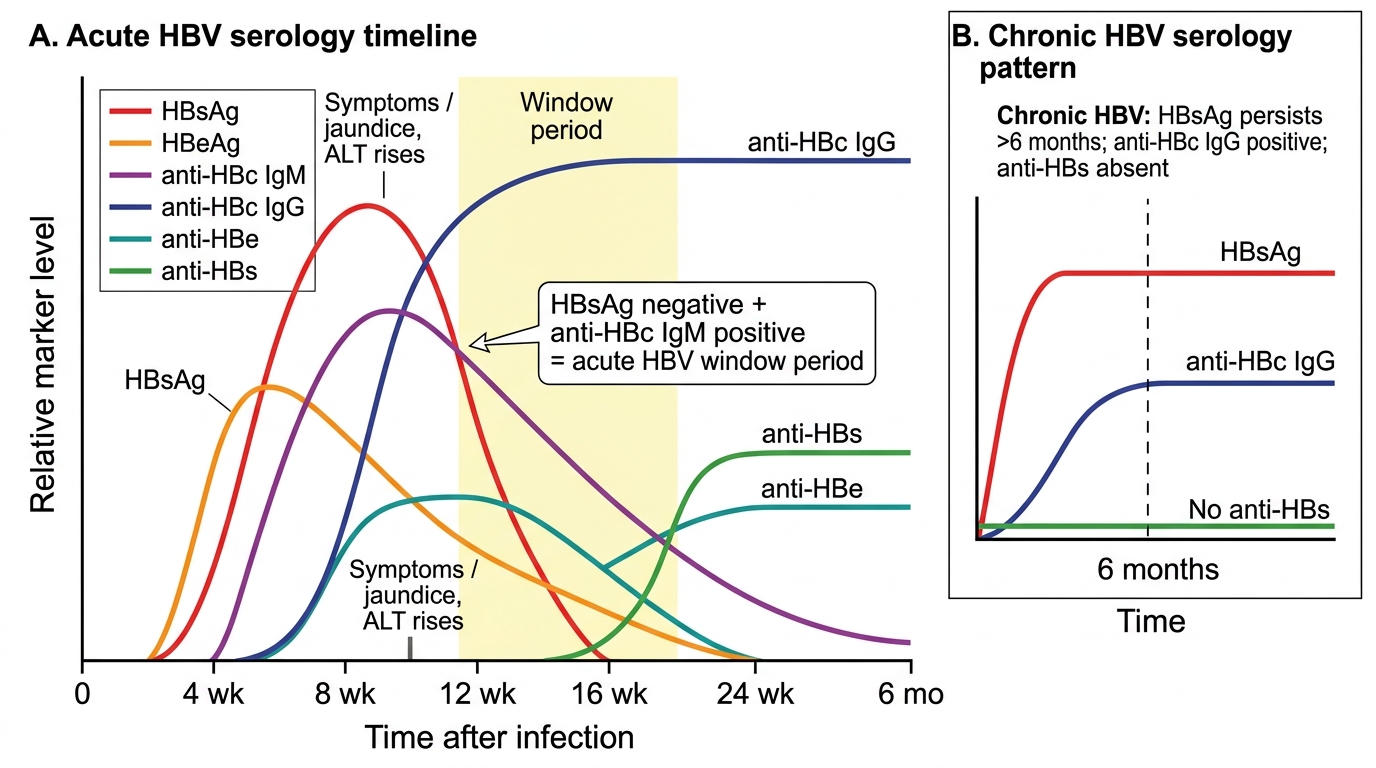
HBV Serology Timeline: Acute Infection and Chronic Pattern
SELF-CHECK
A 32-year-old healthcare worker presents with acute jaundice and markedly elevated ALT (1,100 IU/L). Her HBsAg is NEGATIVE, but her anti-HBc IgM is POSITIVE. HCV RNA is negative. What is the correct interpretation?
A. She has no hepatitis B infection — HBsAg negative rules it out
B. She has chronic hepatitis B — anti-HBc IgM indicates chronicity
C. She has acute hepatitis B in the window period — HBsAg may have declined, but anti-HBc IgM confirms acute infection
D. She has resolved hepatitis B — anti-HBc with negative HBsAg means past infection
Reveal Answer
Answer: C. She has acute hepatitis B in the window period — HBsAg may have declined, but anti-HBc IgM confirms acute infection
Anti-HBc IgM is the diagnostic marker of acute HBV infection. In the window period of acute HBV, HBsAg may have already declined to undetectable levels while anti-HBs has not yet appeared — yet anti-HBc IgM is strongly positive. This is the classic window period pattern. Anti-HBc IgM is NOT a marker of chronicity (that is anti-HBc IgG/total anti-HBc). Past resolved infection would show total anti-HBc positive with anti-HBs also positive. Negative HBsAg does NOT rule out acute HBV — window period must always be considered with acute hepatitis and positive anti-HBc IgM.