Page 12 of 19
IM5.15-17 | Liver Disease Management — SDL Guide (Part 2)
Management of Viral Hepatitis
The management of viral hepatitis encompasses supportive care for acute self-limiting infections and targeted antiviral therapy for chronic or severe disease. The physician must know the full spectrum — from the young student with HAV requiring only rest and hydration, to the pregnant woman with HEV requiring urgent tertiary referral, to the cirrhotic patient with HBV replication requiring lifelong TDF. Understanding which presentations require specific antiviral intervention and which require only supportive care is the core management decision at the IM5.15 KH level.
Provided image
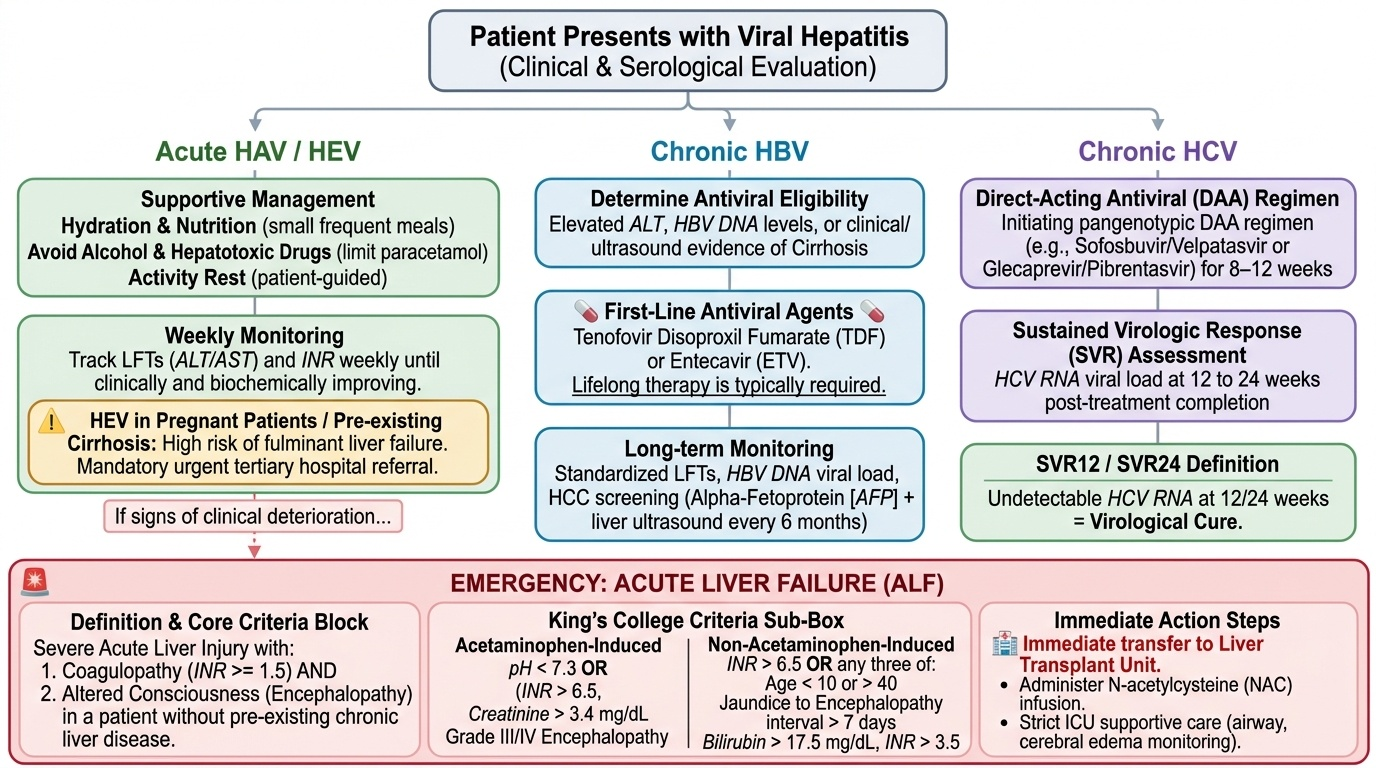
Acute viral hepatitis — supportive management principles:
For all acute hepatitis (HAV, HBV, HCV, HEV in non-pregnant patients), the default management is supportive. There is no evidence that activity restriction accelerates recovery in uncomplicated acute hepatitis, though patients with profound fatigue naturally limit activity themselves. Specific supportive measures: maintain oral hydration and nutrition (small frequent meals, avoid fatty foods which worsen nausea); avoid all alcohol and hepatotoxic drugs (paracetamol in standard doses is acceptable if the patient is not malnourished or alcoholic — common misconception that all analgesics are contraindicated); monitor liver function tests and INR weekly until improving; provide infection control counselling (HAV and HEV — faecal-oral precautions, hand washing, safe food/water; HBV/HCV — safe sex, no needle sharing, no blood donation until cleared). Criteria for hospital admission in acute viral hepatitis: INR >1.5, bilirubin >10 mg/dL, inability to maintain oral intake, altered consciousness (suggests acute liver failure), and any patient with pre-existing liver disease (much higher risk of acute-on-chronic liver failure and fulminant hepatitis, especially HEV in cirrhosis).
Acute liver failure (ALF) — emergency management: When acute hepatitis progresses to fulminant hepatic failure — defined as coagulopathy (INR >1.5) and encephalopathy within 26 weeks of symptom onset in a patient without prior chronic liver disease — the management escalates urgently. Transfer to a liver unit with transplant capability is mandatory. N-acetylcysteine (NAC) is indicated in paracetamol-induced ALF (regardless of time since ingestion if still evolving) and has shown benefit in non-paracetamol ALF from some aetiologies. Manage the complications: cerebral oedema (head elevation 30°, mannitol for herniation), coagulopathy (FFP and vitamin K), hypoglycaemia (10% dextrose infusion), haemodynamic support, and renal failure (renal replacement therapy in HRS context). The King's College Criteria (INR >6.5, or three of five variables including creatinine >3.4 mg/dL, bilirubin >300 μmol/L, age <10 or >40 years, jaundice-to-encephalopathy interval >7 days, drug-induced aetiology) identify patients with non-paracetamol ALF unlikely to survive without transplantation.
Chronic HBV management:
Antiviral therapy for chronic HBV is indicated when there is both significant liver disease (elevated ALT, significant fibrosis on FibroScan/biopsy — typically ≥F2) AND evidence of viral replication (HBV DNA elevated). The two first-line antivirals are:
- Tenofovir disoproxil fumarate (TDF) 300 mg once daily — preferred in most patients; high potency, very high barrier to resistance, inexpensive as generic, safe in pregnancy (category B).
- Entecavir (ETV) 0.5 mg once daily (1 mg/day in lamivudine-resistant patients) — equally potent, high resistance barrier, preferred when TDF-related nephrotoxicity is a concern (renal disease, elderly).
Neither agent is curative — they suppress HBV DNA to undetectable levels, normalise ALT, and arrest fibrosis progression, but HBsAg clearance (functional cure) occurs in only 1–3% per year on therapy. Treatment is therefore lifelong in most patients. Pegylated interferon-alfa (Peg-IFN) offers a finite treatment duration (48 weeks) with higher rates of HBeAg seroconversion and HBsAg clearance, but requires injection, has significant side effects (flu-like illness, cytopenia, neuropsychiatric), and is contraindicated in decompensated cirrhosis. Response monitoring: HBV DNA (every 3–6 months during therapy), ALT, HBeAg/anti-HBe seroconversion, and HBsAg quantification.
Chronic HCV management:
Direct-acting antivirals (DAAs) have revolutionised HCV treatment — pan-genotypic DAA regimens (sofosbuvir + velpatasvir 12 weeks, or glecaprevir + pibrentasvir 8–12 weeks) achieve sustained virological response (SVR) — HCV RNA undetectable 12 weeks after completing treatment — in >95% of patients, effectively curing HCV in most cases. SVR is associated with regression of fibrosis, reduction in HCC risk (though not elimination in cirrhotic patients), and improvement in liver-related mortality. DAAs are well-tolerated (few side effects, once-daily oral dosing). In India, generic DAAs (sofosbuvir-based) are available at low cost under national programmes. Treatment is indicated for all patients with chronic HCV regardless of fibrosis stage. Monitoring: HCV RNA at week 4 (early virological response), at end of treatment (EOT response), and at 12 weeks post-treatment (SVR-12).
SELF-CHECK
A 34-year-old woman with chronic HBV infection has an ALT of 68 IU/L (elevated), HBV DNA 45,000 IU/mL, and a FibroScan score of 9.2 kPa (suggesting significant fibrosis ≥F2). She is currently not on any antiviral therapy. She is planning a pregnancy in 6 months. What is the most appropriate first-line antiviral therapy?
A. Pegylated interferon-alfa — finite treatment duration before pregnancy
B. Entecavir 0.5 mg once daily — preferred over TDF in women of childbearing age
C. Tenofovir disoproxil fumarate (TDF) 300 mg once daily — potent, high resistance barrier, safe in pregnancy
D. Lamivudine — well-tolerated and safe in pregnancy
Reveal Answer
Answer: C. Tenofovir disoproxil fumarate (TDF) 300 mg once daily — potent, high resistance barrier, safe in pregnancy
TDF is the preferred first-line agent for chronic HBV, and critically, it is safe in pregnancy (FDA category B) and is the recommended antiviral for pregnant women with HBV to reduce perinatal transmission risk. Pegylated interferon is contraindicated in pregnancy. Entecavir is teratogenic in animal studies (FDA category C) and is therefore not preferred in a woman planning pregnancy. Lamivudine has a high resistance rate (70% at 5 years) and is no longer a first-line agent. TDF covers both the need for effective antiviral therapy and the safety requirement for impending pregnancy.
Management of Cirrhosis Complications
The management of cirrhosis complications is the most clinically urgent and practically complex domain in hepatology. Each complication has a specific management protocol that must be applied promptly and correctly — delayed or incorrect management of variceal haemorrhage, SBP, or hepatic encephalopathy carries a substantial mortality cost. The management principles below are organised by complication, each linked back to its pathophysiological mechanism.
Provided image
1. Management of ascites:
First-line management of mild-to-moderate ascites: (a) Restrict dietary sodium to 88 mmol/day (approximately 2 g/day) — the mainstay of initial management; advise avoidance of processed foods, pickles, papads, and added salt. (b) Diuretic therapy: combination of spironolactone (aldosterone antagonist, targets the RAAS-driven sodium retention) starting at 100 mg/day, plus furosemide 40 mg/day in the initial ratio of 100:40 to maintain normokalatemia; dose can be titrated upward to spironolactone 400 mg/day + furosemide 160 mg/day if needed. (c) Monitor serum electrolytes and renal function (diuretics can precipitate hyponatraemia and HRS); weigh daily — target weight loss 0.5 kg/day (1 kg/day if peripheral oedema present).
Refractory ascites (failure of maximal diuresis or diuretic intolerance): (a) Large-volume therapeutic paracentesis (LVP) — drain 4–6 litres per session; must be accompanied by intravenous albumin infusion 6–8 g per litre of ascites removed to prevent post-paracentesis circulatory dysfunction (PPCD — splanchnic vasodilation worsened by sudden reduction of intra-abdominal pressure → haemodynamic collapse → HRS). (b) TIPS (transjugular intrahepatic portosystemic shunt) — an interventional radiology procedure placing a stent between the portal vein and hepatic vein via the jugular vein, reducing portal pressure and controlling refractory ascites; contraindicated in severe hepatic encephalopathy (worsened by shunting), Heart failure, and severe coagulopathy. (c) Liver transplantation for eligible patients.
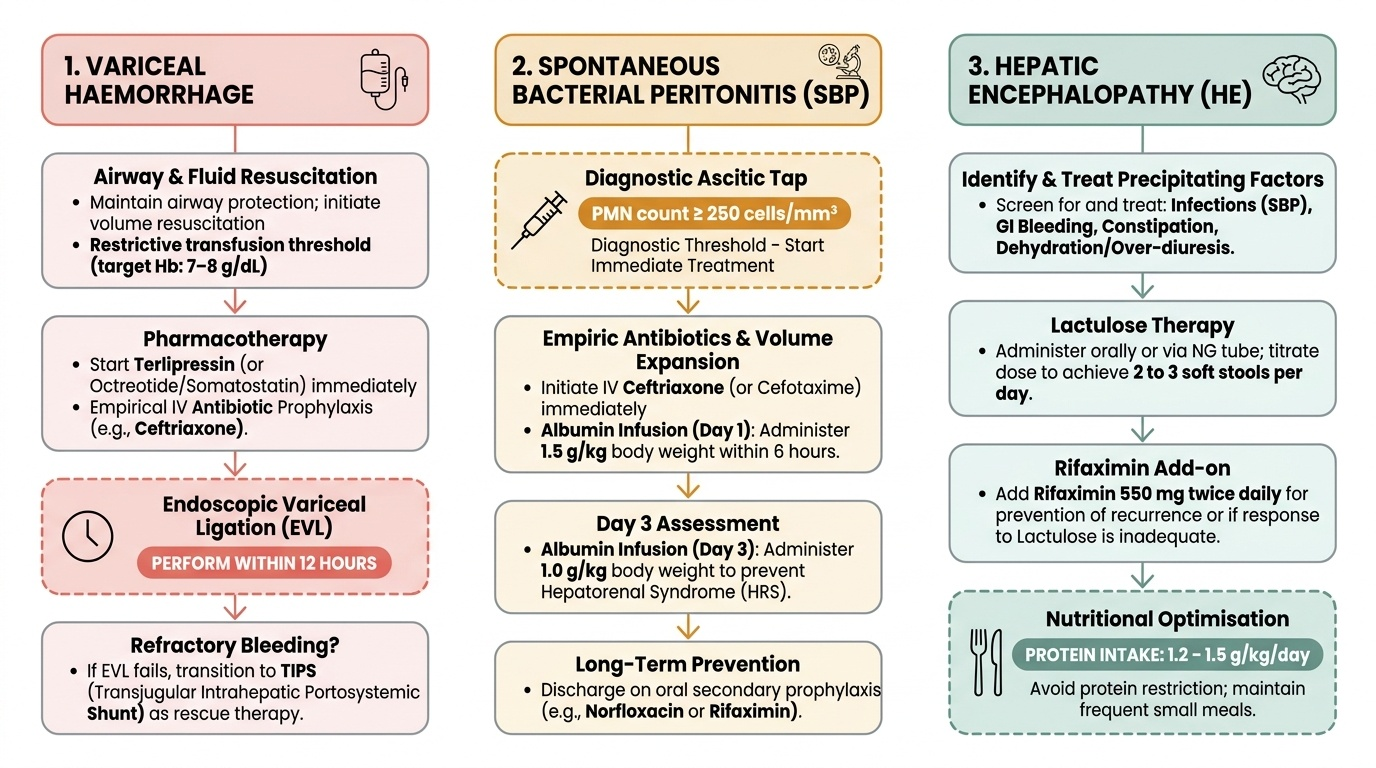
2. Management of spontaneous bacterial peritonitis (SBP):
Once the diagnostic threshold is reached (ascitic PMN ≥250 cells/mm³), treatment must begin immediately — do not wait for culture results:
- Empirical antibiotics: IV cefotaxime 2 g three times daily or ceftriaxone 1–2 g daily for 5 days. Cover: gram-negative enteric organisms (E. coli, Klebsiella) and streptococcal species. Quinolone-resistant organisms are increasing in community-acquired SBP in India — empirical cephalosporins are preferred over fluoroquinolones for empirical therapy.
- IV albumin: 1.5 g/kg at diagnosis and 1 g/kg on day 3 — randomised controlled trial evidence (Sort 1999) shows albumin infusion reduces HRS development and mortality in SBP, even in patients with normal creatinine at baseline. This is mandatory, not optional.
- Secondary prophylaxis: after a first SBP episode, norfloxacin 400 mg/day indefinitely (or if not available, ciprofloxacin 500 mg/day) reduces recurrence risk from ~70%/year to ~20%/year.
- Primary prophylaxis: indicated in high-risk cirrhotic patients — those with ascitic protein <15 g/L + Child-Pugh ≥9 or serum creatinine ≥1.2 mg/dL or Na ≤130 mEq/L.
3. Management of acute variceal haemorrhage:
This is a medical emergency with 15–20% 6-week mortality. The management sequence is:
- Resuscitation: establish IV access (two large-bore cannulas), IV fluids cautiously (over-resuscitation raises portal pressure and worsens rebleeding — target Hb ~7–8 g/dL with blood transfusion, not higher), correct severe coagulopathy with FFP/platelets if active bleeding.
- Vasoactive drugs — start immediately on presentation, before endoscopy: terlipressin 2 mg IV bolus every 4–6 hours (preferred in India, reduces portal pressure via V1 receptor splanchnic vasoconstriction) OR somatostatin/octreotide (IV infusion). Continue for 3–5 days.
- Antibiotics: IV ceftriaxone 1 g/day or norfloxacin for 7 days prevents bacterial infection (up to 20% of cirrhotic patients with GI bleed develop SBP/bacteraemia) and reduces rebleeding and mortality — this is guideline-mandated in all patients.
- Endoscopic therapy: oesophageal variceal ligation (EVL) — rubber band ligation of varices — is the standard endoscopic treatment; sclerotherapy (injection of sclerosant into variceal channel) is an alternative when EVL is unavailable. Endoscopy should be performed within 12 hours of presentation.
- Balloon tamponade (Sengstaken-Blakemore tube): temporary measure for massive uncontrolled haemorrhage when endoscopy is not immediately available or has failed — compresses varices mechanically; maximum 24 hours; high complication rate (aspiration, oesophageal necrosis); use as bridge to definitive therapy.
- TIPS: for refractory or recurrent variceal bleeding not controlled by endoscopy + vasoactive drugs.
- Secondary prophylaxis: non-selective beta-blockers (propranolol starting 10–20 mg twice daily, titrated to reduce resting heart rate by 25% or to 55–60 bpm; or carvedilol — vasodilatory beta-blocker with additional portal pressure-reducing effect) combined with repeated EVL sessions every 4–6 weeks until varices obliterated.
4. Management of hepatic encephalopathy (HE):
The first and most important step in managing HE is identifying and treating the precipitating cause — this alone may reverse the encephalopathy without the need for specific anti-HE therapy. Common precipitants and their treatments: GI bleed (haemostasis, bowel clearance with lactulose enema); infection/SBP (antibiotics); hyponatraemia (fluid restriction, hypertonic saline cautiously); diuretic over-dosage (withhold diuretics, replace fluid and electrolytes); constipation (lactulose titration); sedatives/opioids (withhold, consider flumazenil for benzodiazepines); urinary tract infection (antibiotics); dehydration (IV fluids).
Specific pharmacological treatment:
- Lactulose (syrup, 20–30 mL two to four times daily, titrated to produce 2–3 soft stools per day): non-absorbable disaccharide — gut bacteria ferment lactulose to short-chain fatty acids, acidifying the colon; acidic pH converts ammonia (NH₃) to ammonium (NH₄⁺) which is ionised and cannot be absorbed; additionally acts as a laxative reducing substrate for bacterial urease. Lactulose is first-line for both acute treatment and secondary prevention of HE.
- Rifaximin 550 mg twice daily: non-absorbable oral antibiotic that reduces gut ammonia-producing bacteria; added for recurrent or refractory HE (in combination with lactulose); superior to lactulose for prevention of HE recurrence in the RFHE trial. Not absorbed systemically — very few side effects.
- Protein intake: the old advice to restrict dietary protein in HE is outdated and harmful — protein restriction causes sarcopenia (itself a major risk factor for HE and poor outcomes in cirrhosis). Current guidelines recommend 1.2–1.5 g/kg/day of protein, preferring vegetable protein and branched-chain amino acids (BCAA) over animal protein.
- Grade III–IV HE: protect the airway (risk of aspiration), consider nasogastric feeding, manage cerebral oedema (for acute liver failure with fulminant HE — mannitol), ICU monitoring.
5. Management of hepatorenal syndrome (HRS):
HRS is defined as acute kidney injury in cirrhosis with ascites after exclusion of other causes (hypovolaemia, nephrotoxins, obstructive uropathy, parenchymal renal disease) and failure of response to volume expansion with IV albumin 1 g/kg/day × 2 days (plus withdrawal of diuretics).
- First-line: Terlipressin 1–2 mg IV every 4–6 hours (or as a continuous infusion) + albumin 20–40 g/day until serum creatinine falls below 1.5 mg/dL (treatment response), or for maximum 14 days. Terlipressin causes splanchnic vasoconstriction via V1 receptors, redirecting blood to the systemic and renal circulation. Response rate in HRS-AKI: ~50% with terlipressin + albumin (vs ~9% with albumin alone). Adverse effects: ischaemia (myocardial, peripheral, mesenteric) — contraindicated in ischaemic cardiovascular disease.
- Alternative: Noradrenaline (norepinephrine) infusion + albumin — equivalent efficacy to terlipressin in ICU setting, less available in general wards.
- TIPS: bridge to transplantation in HRS-CKD or when HRS-AKI is unresponsive to vasoconstrictor therapy.
- Renal replacement therapy: for refractory AKI as a bridge to transplantation — not a definitive treatment (the kidney is functionally normal; only liver transplant corrects the underlying haemodynamic derangement).
- Liver transplantation is the definitive and only curative treatment for HRS.
6. HCC management (overview):
Treatment per BCLC stage: BCLC 0/A (very early/early — single nodule ≤2 cm or up to 3 nodules ≤3 cm, Child-Pugh A/B, performance status 0–1): surgical resection (if adequate remnant liver function), percutaneous ablation (radiofrequency or microwave, for tumours ≤3 cm), or liver transplantation within Milan criteria (single ≤5 cm or ≤3 nodules each ≤3 cm, no vascular invasion, no extrahepatic spread). BCLC B (intermediate — multinodular, Child-Pugh A/B): transarterial chemoembolisation (TACE) — delivers chemotherapy (doxorubicin) and embolic material directly to the tumour via the hepatic artery. BCLC C (advanced — vascular invasion or extrahepatic spread, Child-Pugh A/B, PS 1–2): sorafenib (tyrosine kinase inhibitor, first approved systemic agent) or lenvatinib (equivalent or superior efficacy, first-line alternative); atezolizumab + bevacizumab (immunotherapy + anti-VEGF) is now the preferred first-line regimen in international guidelines for advanced HCC in patients without oesophageal varices at risk of bleeding. BCLC D (end-stage): best supportive care.
SELF-CHECK
A 50-year-old man with decompensated cirrhosis (Child-Pugh B) is admitted with acute large-volume haematemesis. He is haemodynamically unstable (BP 85/55, HR 118). After initial resuscitation, what is the CORRECT sequence of next interventions?
A. Endoscopy immediately, then vasoactive drug (terlipressin), then antibiotics after endoscopy confirms varices
B. Terlipressin IV immediately + IV ceftriaxone simultaneously, then endoscopy within 12 hours
C. Emergency TIPS procedure, then vasoactive drug, then endoscopy in 24 hours
D. Blood transfusion to Hb >10 g/dL, then endoscopy within 6 hours, antibiotics after discharge
Reveal Answer
Answer: B. Terlipressin IV immediately + IV ceftriaxone simultaneously, then endoscopy within 12 hours
Current guidelines mandate three concurrent interventions in acute variceal haemorrhage: (1) vasoactive drug (terlipressin or octreotide) started IMMEDIATELY — before endoscopy, at the time of presentation; (2) prophylactic IV antibiotics (ceftriaxone or norfloxacin) SIMULTANEOUSLY — not after endoscopy — because bacterial infection complicates up to 20% of variceal bleeds and antibiotics reduce rebleeding and mortality; (3) endoscopy (EVL) within 12 hours. Blood transfusion targets Hb 7–8 g/dL (not >10 — overtransfusion raises portal pressure). TIPS is reserved for refractory bleeding. The key error in option A is deferring both terlipressin and antibiotics until after endoscopy — both must start immediately.
Hepatitis Vaccination: Indications and Schedules
Hepatitis vaccination is a core preventive medicine competency for the general physician. The IM5.16 competency requires the ability to enumerate the indications, know the precautions, and counsel patients on vaccination for hepatitis — meaning the clinician must know not just the schedules but also who specifically needs the vaccine and what to tell the patient about it. There are two vaccines for hepatitis relevant to clinical practice in India: hepatitis B vaccine (well-established, universal immunisation) and hepatitis A vaccine (targeted high-risk immunisation). There is no licensed vaccine for hepatitis C or hepatitis E in India (an HEV vaccine, HEV-239/Hecolin, is licensed in China only; not globally available).
Provided image
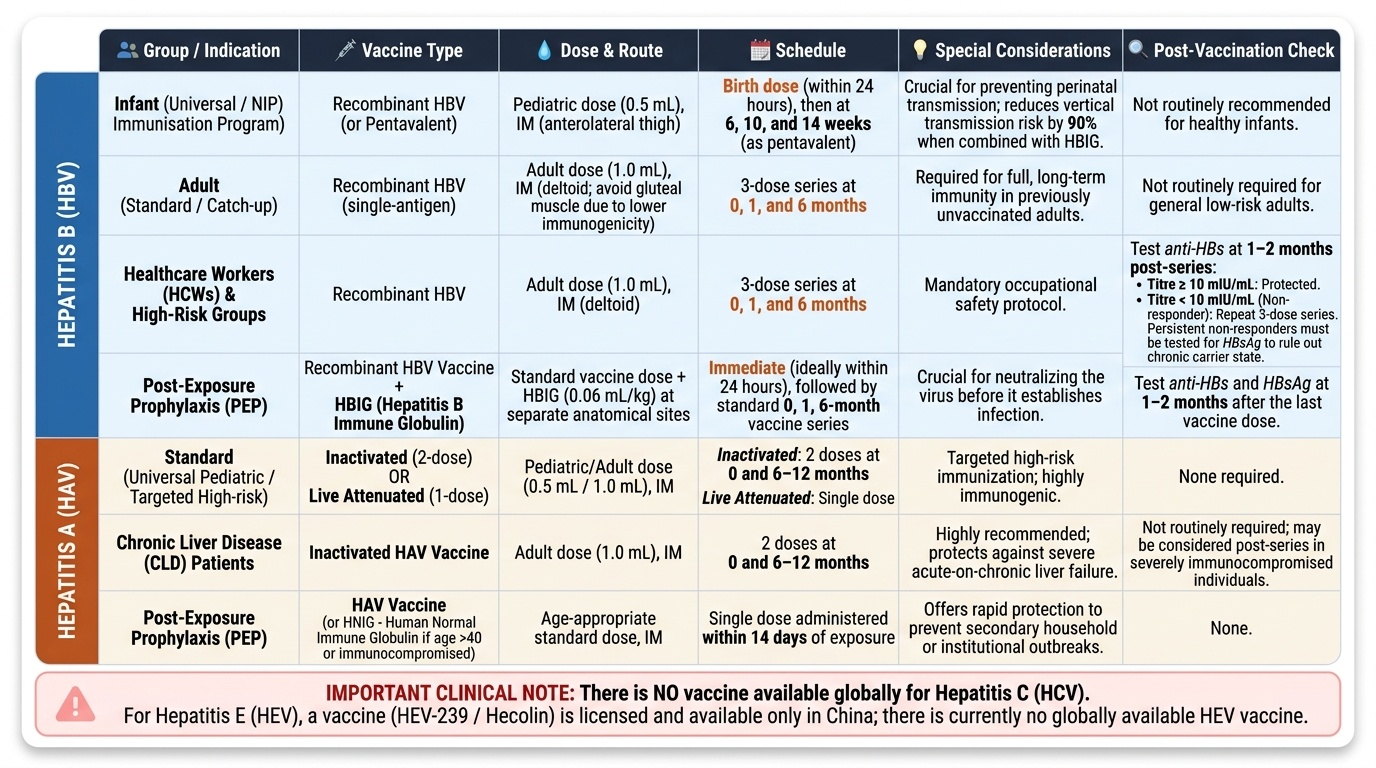
Hepatitis B vaccination:
Schedule: 3-dose series at 0, 1, and 6 months (primary series). In adults, all three doses are required for full immunity — check anti-HBs at 1–2 months post-series; a titre ≥10 mIU/mL indicates protection. Non-responders (anti-HBs <10 mIU/mL) should receive a repeat 3-dose series; persistent non-responders should be tested for HBsAg (may be chronic HBV carriers).
Neonatal schedule (National Immunisation Program, India): birth dose within 24 hours of birth (critical for prevention of perinatal transmission — reduces vertical transmission risk by >90% when combined with HBIG in high-risk births), followed by doses at 6 weeks, 10 weeks, and 14 weeks as part of the pentavalent vaccine.
Indications for hepatitis B vaccination (prioritised groups):
- Universal — all infants from birth (NIP schedule)
- Healthcare workers and students — highest occupational risk; 3-dose series mandatory before clinical attachment
- Household contacts and sexual partners of HBsAg-positive individuals
- Patients on haemodialysis or receiving frequent blood products (thalassaemia, haemophilia)
- HIV-positive individuals and other immunocompromised patients — note: higher dose (40 µg) may be needed for immunocompromised; re-check anti-HBs after series
- Persons with chronic liver disease (including HCV, NAFLD, ALD) — HBV superinfection can cause acute decompensation
- Travellers to highly endemic areas
- Men who have sex with men (MSM), persons with multiple sexual partners
- People who inject drugs (PWID)
Contraindications to hepatitis B vaccine: anaphylaxis to a previous dose or to yeast (HBV vaccine is produced in yeast — Saccharomyces cerevisiae). Pregnancy is NOT a contraindication — vaccination is safe in pregnancy and recommended for pregnant women at risk.
Hepatitis B Immune Globulin (HBIG): Used for post-exposure prophylaxis (needle-stick from HBsAg-positive source, sexual exposure within 14 days) and for neonates of HBsAg-positive mothers (0.5 mL IM at birth, given simultaneously with the birth dose of vaccine at separate anatomical sites). HBIG provides immediate passive immunity while vaccine induces active immunity.
Hepatitis A vaccination:
Schedule: 2-dose series at 0 and 6–12 months (or 6–18 months depending on brand). A single dose provides protection for 1–2 years; the full series provides long-term (likely lifelong) immunity. In India, high seroprevalence from childhood exposure limits routine adult vaccination in low-income populations, but targeted vaccination of at-risk adults is clinically important.
Indications for hepatitis A vaccination:
- Travellers to HAV-endemic areas (most of Asia, Africa, Central/South America)
- Food handlers — prevention of food-borne outbreaks
- Patients with chronic liver disease (including cirrhosis, chronic HBV or HCV, NAFLD) — HAV superinfection in a patient with chronic liver disease carries much higher mortality than in a healthy host; vaccination is especially important in this group
- Household contacts of HAV cases
- Immunocompromised patients (e.g., HIV) — use inactivated HAV vaccine (live vaccines contraindicated)
- People who inject drugs
- MSM — HAV transmission documented in MSM communities
- Post-exposure prophylaxis (PEP): single dose of HAV vaccine within 14 days of exposure is as effective as HAIG in immunocompetent individuals aged 1–40 years; HAIG preferred for immunocompromised and those >40 years.
Patient counselling points for hepatitis vaccination:
1. The vaccine does not cause the disease (it is not a live virus — hepatitis B vaccine uses recombinant HBsAg; hepatitis A vaccine is inactivated virus).
2. Side effects are mild — soreness at injection site, occasional mild fever for 24–48 hours; anaphylaxis is rare.
3. The series must be completed for full protection — a single dose of HBV vaccine is NOT sufficient for long-term protection.
4. After the HBV series, check anti-HBs to confirm response, especially in healthcare workers and immunocompromised patients.
5. There is no vaccine for hepatitis C — stress this to patients with HCV risk factors; prevention relies entirely on behavioural measures (safe injection practices, protected sex, no needle sharing).