Page 3 of 23
IM6.1-6 | HIV Foundations and Opportunistic Disease — SDL Guide (Part 3)
Self-Assessment: Integrating HIV Clinical Staging and OI Recognition
At this stage of the module you have covered the full natural history of HIV from acute seroconversion through progressive immunosuppression to AIDS-defining illness, and the constellation of opportunistic infections, malignancies, and mucocutaneous lesions that mark each stage of immune decline. The following clinical vignettes are designed to consolidate your ability to apply the CD4 threshold model in real clinical scenarios, recognise specific OIs by their clinical, radiological, and laboratory clues, and classify HIV disease accurately according to WHO staging. Each scenario requires you to integrate multiple data points — CD4 count, clinical presentation, investigation results — and arrive at a diagnosis and management plan before reading the analysis. This is the skill tested in final-year examinations and, more importantly, the skill that will enable you to accurately diagnose and manage PLHIV presenting to district hospitals across India. Work through each vignette independently before reading the analysis. The reference table below provides a structured recap of the key CD4 thresholds, associated OIs, and prophylaxis recommendations as a self-assessment anchor.
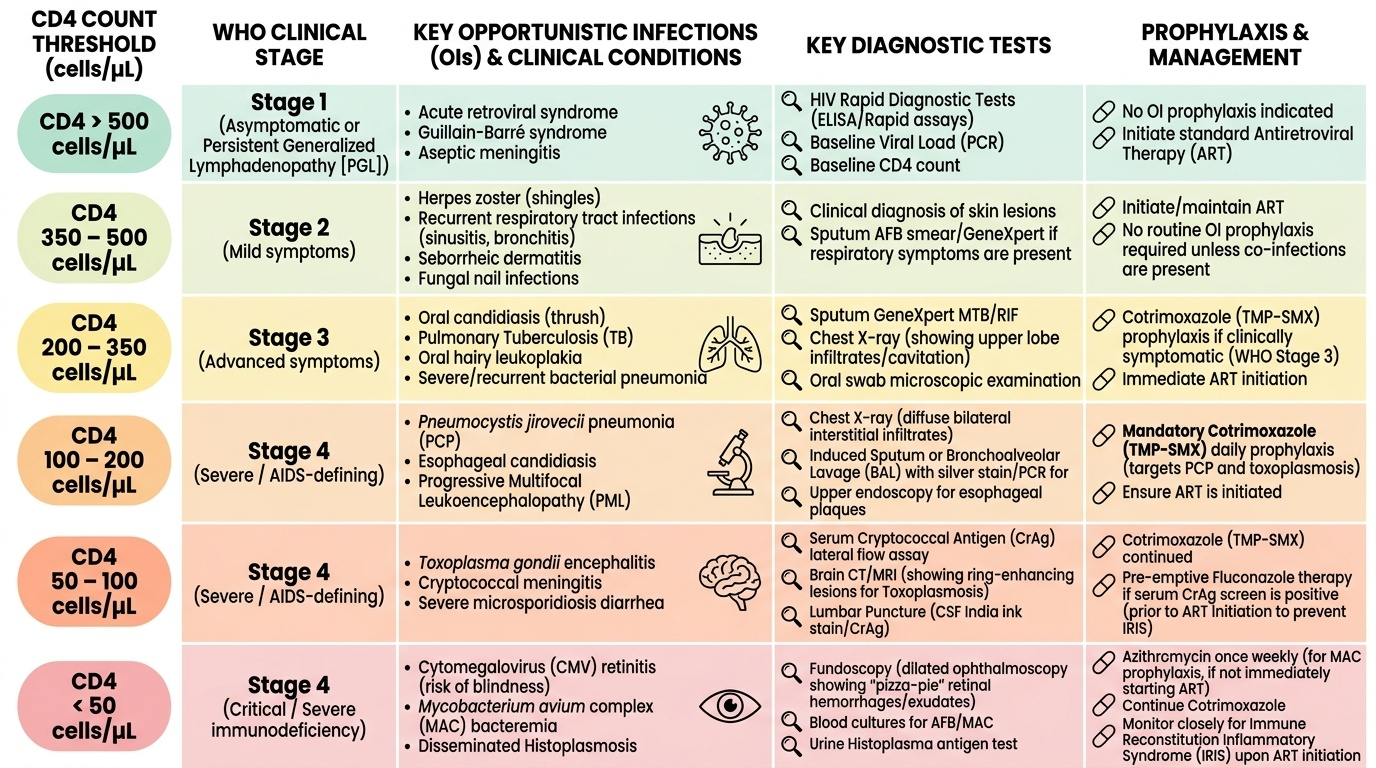
Provided image
HIV CD4 Thresholds, WHO Staging, OIs, and Prophylaxis
Scenario A: A 30-year-old man, newly diagnosed HIV, presents with three weeks of progressive dry cough, exertional dyspnoea, and fever. SpO₂ is 82% on room air. CXR shows bilateral perihilar ground-glass infiltrates. LDH is 780 IU/L. His CD4 count is 62 cells/µL. What is the diagnosis, and what treatment and adjunctive therapy does he need?
Analysis: CD4 62 + bilateral interstitial infiltrates + SpO₂ 82% + elevated LDH = PCP (Pneumocystis jirovecii pneumonia). The SpO₂ <90% (PaO₂ <70 mmHg equivalent) and the degree of respiratory compromise indicate moderate-to-severe PCP → adjunctive corticosteroids are mandatory (prednisolone 40 mg BD for 5 days, then taper over 21 days). Treatment: high-dose TMP-SMX (TMP 15–20 mg/kg/day) × 21 days. Confirm diagnosis via bronchoalveolar lavage (BAL) with silver stain for Pneumocystis.
Scenario B: A 44-year-old man with known HIV (on ART, but poor adherence for 6 months) presents with 3 weeks of headache, low-grade fever, and one episode of vomiting. CD4 = 38 cells/µL. Examination shows neck stiffness minimal, no focal neurology. CT head is normal. LP opening pressure is 38 cm H₂O; CSF India ink stain is positive for encapsulated yeast. What is the diagnosis and the most important immediate management step beyond antifungals?
Analysis: Cryptococcal meningitis confirmed by India ink stain + severely elevated ICP (38 cm H₂O, normal <25). Beyond starting Amphotericin B + flucytosine, the most important immediate intervention is therapeutic LP to reduce intracranial pressure — remove CSF to bring pressure below 20 cm H₂O (20–30 mL if needed). Repeat therapeutic LP daily until pressure normalises. Untreated raised ICP is the leading cause of death in cryptococcal meningitis.
Scenario C: A 25-year-old woman presents with multiple violaceous nodular lesions on her face and lower extremities for two months, and dark plaques on her hard palate. She is newly diagnosed HIV with a CD4 count of 55 cells/µL. She has no respiratory symptoms. What is the diagnosis, what is the causative pathogen, and what is the first-line treatment?
Analysis: Clinical picture = AIDS-related Kaposi sarcoma caused by HHV-8. At CD4 55 with skin + mucosal (palate) involvement without visceral symptoms, this is limited mucocutaneous KS. First-line treatment is ART (start immediately) — immune reconstitution alone can cause regression of limited KS. She does not need chemotherapy at this stage, but requires close monitoring for disease progression.
CLINICAL PEARL
The mnemonic 'FACT' captures the four cardinal sites where HIV-related OIs cluster: F — Fungus in the lung (PCP) and brain (Cryptococcus); A — Atypical organisms (MAC, Cryptosporidium, CMV); C — CNS (toxoplasmosis, PCNSL, CMV encephalitis, HIV encephalopathy); T — TB at all CD4 levels with increasing severity at lower counts. A second pearl: in any HIV-positive patient presenting with a focal neurological deficit and ring-enhancing lesion on CT/MRI, always start empirical toxoplasmosis treatment first (pyrimethamine + sulfadiazine + leucovorin) — if there is clinical and radiological improvement at 2 weeks, toxoplasmosis is confirmed and a brain biopsy is avoided. Reserve biopsy for non-responders (primary CNS lymphoma being the main differential). Third pearl: oral hairy leucoplakia cannot be scraped off — this single clinical feature distinguishes it from oral candidiasis and makes it virtually pathognomonic of HIV.