Page 14 of 23
IM6.13-17 | HIV Treatment and Prophylaxis — SDL Guide (Part 2)
Post-Exposure Prophylaxis (PEP) and Pre-Exposure Prophylaxis (PrEP)
Post-exposure prophylaxis (PEP) is the use of antiretroviral drugs after a potential HIV exposure to prevent seroconversion. It is one of the most time-critical interventions in medicine — efficacy is highest when started within 2 hours, and must be started within 72 hours; beyond 72 hours, PEP is not recommended as there is no evidence of benefit. PEP is not 100% effective — it reduces but does not eliminate the risk of infection; strict adherence for the full 28-day course is essential. The mechanism of PEP is pharmacological interruption of viral replication in the days immediately after exposure, before the virus can establish a stable reservoir in lymphoid tissue. Animal models suggest that HIV disseminates from the mucosal portal of entry to regional lymph nodes within 24–72 hours of exposure; PEP must block replication during this narrow window before the infection becomes irreversible. This temporal biology explains why the 72-hour deadline is absolute, not approximate, and why earlier initiation is meaningfully more effective than later initiation within that window. Understanding this mechanism reinforces the clinical priority of having PEP starter packs immediately accessible in every casualty department, emergency room, and ART centre in India.
Indications for PEP:
- Occupational exposure (healthcare workers): Needlestick injury, sharp instrument injury, or mucous membrane/non-intact skin exposure to blood, tissue, or certain body fluids from a known or suspected HIV-positive source. Risk is highest for: deep percutaneous injury, hollow-bore needle, large-gauge needle, visibly bloody device, or source patient with high viral load. The average risk of HIV transmission from a needlestick injury from an HIV-positive source is approximately 0.3% (3 in 1000); for mucous membrane exposure, ~0.09%.
- Non-occupational exposure (nPEP): Sexual exposure (unprotected anal or vaginal intercourse with an HIV-positive partner or a partner of unknown status in a high-prevalence setting); sexual assault; injecting drug use with shared needles from an HIV-positive source.
PEP assessment: Before starting PEP, assess: the nature of the exposure (risk level — high, medium, low); the HIV status of the source (known positive with viral load, unknown, known negative); and the HIV status of the exposed person (baseline HIV test mandatory). If the source is known HIV-negative, PEP is not indicated. If the source is on ART with undetectable viral load, the risk of transmission is extremely low (U=U principle) — PEP may still be offered while confirmatory testing is obtained, but the risk is negligible.
NACO PEP regimen (standard 28-day course):
- Preferred: TDF 300 mg + 3TC 300 mg + DTG 50 mg once daily for 28 days (same components as first-line TLD)
- Alternative (if DTG not available or contraindicated): TDF + 3TC + LPV/r (lopinavir/ritonavir)
- Special populations: Pregnant women — TDF + 3TC + AZT or TDF + 3TC + LPV/r (DTG safety in early pregnancy — NACO now permits DTG in pregnancy but some guidelines remain cautious)
PEP monitoring: Baseline HIV test (to confirm HIV-negative status before PEP starts), renal function (TDF), full blood count; repeat HIV test at 6 weeks and 3 months after exposure to confirm seroconversion has not occurred. Advise the individual to use barrier contraception and avoid blood donation until 3-month HIV test is confirmed negative.
Pre-exposure prophylaxis (PrEP): The use of antiretroviral drugs by HIV-negative individuals at high ongoing risk of HIV acquisition, to prevent infection. The standard PrEP regimen in India (NACO, introduced 2018 for high-risk groups) is TDF + FTC (emtricitabine) once daily (Truvada or generic equivalent), taken daily. Efficacy is very high (>90% reduction in acquisition risk) when adhered to consistently. Indications in India: MSM, transgender women, female sex workers, serodiscordant couples (HIV-negative partner with HIV-positive partner not virally suppressed), and injecting drug users. Baseline testing includes: HIV test (must be confirmed HIV-negative), creatinine (eGFR; TDF contraindicated if eGFR <60 mL/min), hepatitis B status (TDF covers HBV — stopping PrEP in HBsAg-positive patients can cause HBV reactivation flare). Follow-up every 3 months: HIV test, STI screen, renal function, adherence counselling.
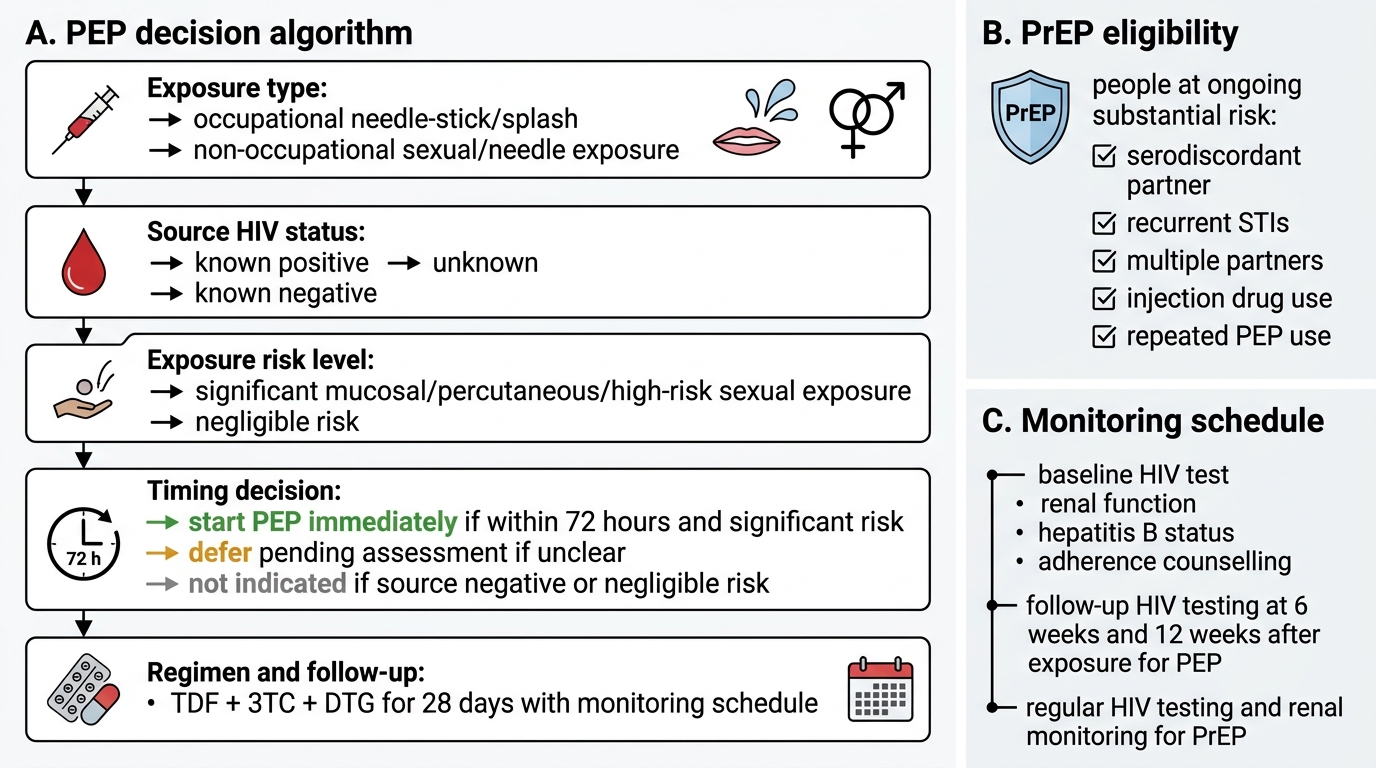
HIV PEP Decision Algorithm and PrEP Monitoring
OI Prophylaxis: Drugs, Thresholds, and Diarrhoea Management
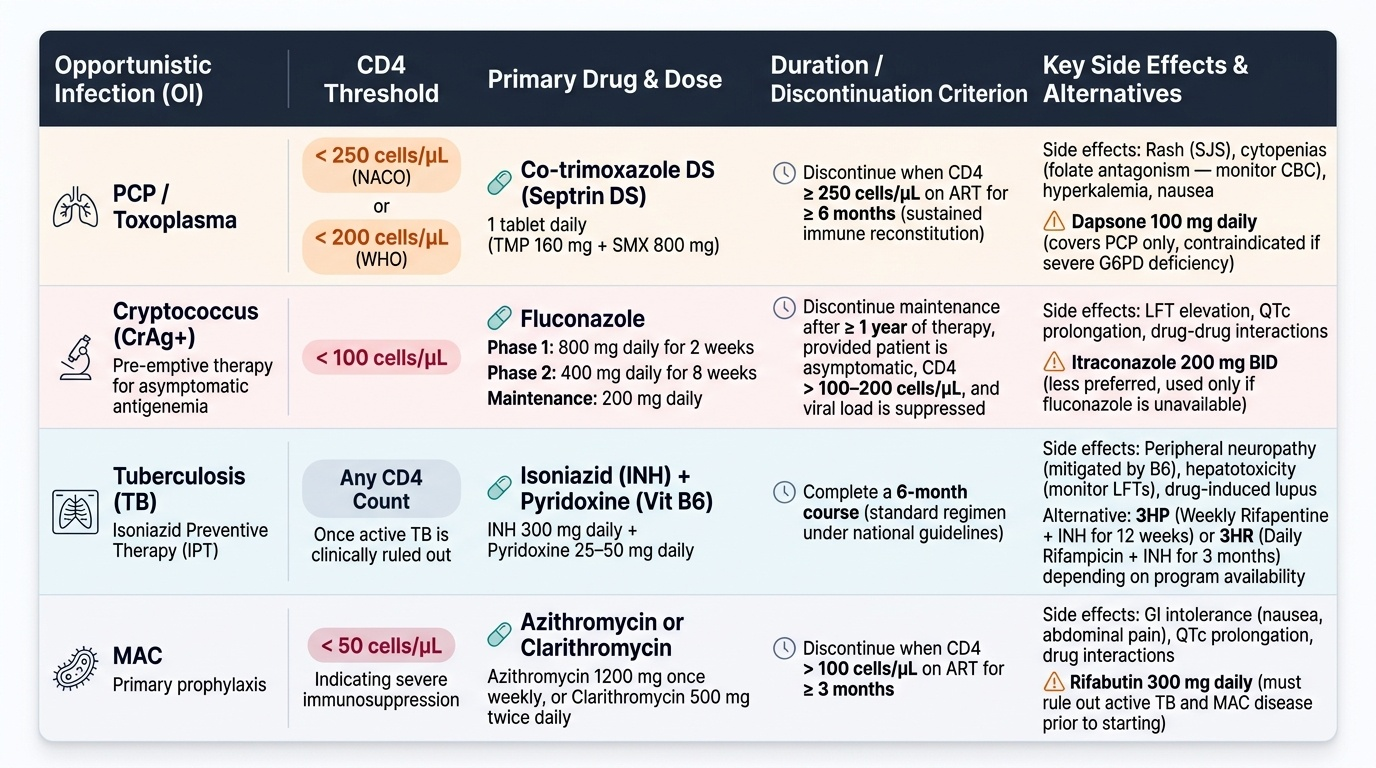
Prophylaxis against opportunistic infections is one of the most evidence-based and cost-effective interventions in HIV medicine. It is indicated at specific CD4 thresholds — the thresholds at which the probability of an OI developing without prophylaxis exceeds the risk of the prophylactic drug itself. Prophylaxis can be primary (preventing first episode) or secondary (preventing recurrence after a treated episode). Secondary prophylaxis (maintenance therapy) is continued until immune reconstitution on ART restores CD4 above the protective threshold for ≥6 months. The foundation of prophylaxis in India is different from high-income country settings because of the extremely high burden of TB and the limited availability of certain specialist drugs. Co-trimoxazole is the most impactful single prophylactic agent in the Indian HIV context: a single cheap tablet daily protects against PCP, Toxoplasma, Isospora, and certain bacterial infections simultaneously. IPT addresses the massive TB-HIV overlap that makes TB the leading cause of death in PLHIV in India. The CrAg pre-emptive strategy has reduced cryptococcal meningitis incidence where implemented. Understanding the rationale behind each threshold and each drug — not merely memorising the table — enables the clinician to adapt when the standard drug is unavailable, contraindicated, or not tolerated. The following covers NACO-recommended prophylaxis regimens and the management of the major HIV-related diarrhoeal pathogens.
Provided image
Co-trimoxazole (TMP-SMX) prophylaxis:
- Indication: CD4 <250 cells/µL (NACO threshold; WHO uses <200 cells/µL)
- Dose: Co-trimoxazole DS (Septrin DS: TMP 160 mg + SMX 800 mg) — one tablet once daily
- Protects against: PCP, Toxoplasma gondii encephalitis (seropositive patients), Isospora belli, Nocardia, Salmonella, and certain bacterial infections
- Discontinue when: CD4 ≥250 cells/µL on ART for ≥6 months (sustained immune reconstitution)
- Side effects: Rash (including Stevens-Johnson syndrome — rare), bone marrow suppression (folate antagonism — monitor CBC), hyperkalaemia (especially with TDF), nausea
- Contraindications: Sulfa allergy; G6PD deficiency (risk of haemolysis — dapsone substitute in mild-moderate deficiency)
- Alternative if sulfa-allergic: Dapsone 100 mg once daily (for PCP only, does not cover Toxoplasma as monotherapy; dapsone + pyrimethamine + leucovorin for dual coverage)
Fluconazole pre-emptive therapy for cryptococcal disease:
- Indication: Serum CrAg positive at CD4 <100 cells/µL (without meningitis)
- NACO pre-emptive protocol: Fluconazole 800 mg loading dose (day 1), then 400 mg/day × 2 weeks, then 200 mg/day for 1 year (or until CD4 >200 on ART)
- Rationale: Pre-emptive fluconazole in CrAg-positive patients significantly reduces progression to cryptococcal meningitis
Isoniazid Preventive Therapy (IPT):
- Indication: All PLHIV after excluding active TB (WHO 4-symptom screen negative) regardless of CD4 count
- Regimen: Isoniazid 300 mg/day × 6 months + pyridoxine (vitamin B6) 25 mg/day (to prevent INH-related peripheral neuropathy)
- Extended IPT: INH for 36 months (or continuous) in high-TB-burden settings — NACO recommends extended IPT
- Contraindication: Active TB (must exclude first); active hepatitis (elevated transaminases >3× ULN)
MAC prophylaxis: Azithromycin 1250 mg once weekly at CD4 <50 cells/µL — indicated in settings with high MAC prevalence; less commonly used in India (lower MAC incidence than in Western cohorts) but indicated in patients with very low CD4 who are not expected to reconstitute rapidly on ART.
Management of HIV-related diarrhoea (IM6.13): Diarrhoea in HIV is one of the most common and debilitating complications. The management depends on the causative organism:
- Cryptosporidium: No reliably effective antiprotozoal therapy; nitazoxanide (500 mg BD × 3 days for immunocompetent — less effective in HIV) has modest benefit. ART is the definitive treatment — CD4 recovery controls cryptosporidiosis. Supportive: oral rehydration, loperamide for symptom control, nutritional support.
- Isospora belli: TMP-SMX DS (two tablets QID × 10 days, then one tablet BD × 3 weeks) — highly effective; secondary prophylaxis with one tablet daily until CD4 >200 on ART.
- Microsporidiosis: Albendazole 400 mg BD × 4 weeks (for Encephalitozoon intestinalis); fumidil for Enterocytozoon bieneusi — limited availability; ART is the mainstay.
- Salmonella bacteraemia: Ciprofloxacin or third-generation cephalosporin; duration 4–6 weeks (to prevent relapse); secondary prophylaxis with ciprofloxacin until CD4 >200.
- Campylobacter: Azithromycin or ciprofloxacin (note rising quinolone resistance).
- CMV colitis: Ganciclovir IV 5 mg/kg BD × 21 days (or oral valganciclovir) — for CMV colitis at CD4 <50; maintenance valganciclovir until CD4 >100 on ART.
- Clostridium difficile (C. diff) colitis: Oral vancomycin or oral fidaxomicin (preferred over metronidazole for severe or recurrent disease).
- ART-related diarrhoea: Lopinavir/ritonavir causes secretory diarrhoea in up to 30% — manage with loperamide; consider regimen switch if severe.
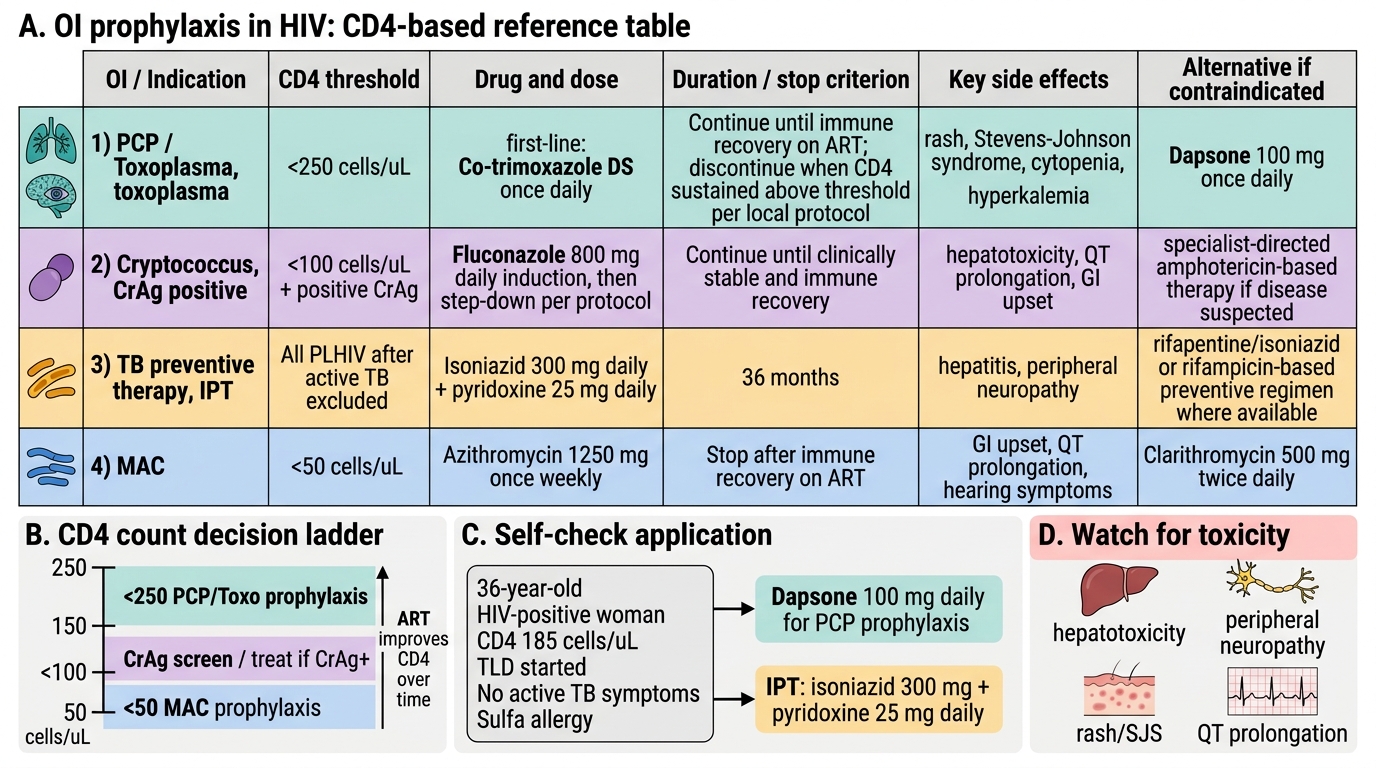
HIV Opportunistic Infection Prophylaxis Reference
SELF-CHECK
A 36-year-old HIV-positive woman with CD4 count 185 cells/µL is started on ART (TLD). She has no active TB symptoms and a negative WHO 4-symptom screen. She is allergic to sulfa drugs (rash with co-trimoxazole). Which prophylaxis regimen is MOST appropriate for her?
A. No prophylaxis required as CD4 >150 cells/µL
B. Fluconazole 200 mg daily for cryptococcal prophylaxis
C. Dapsone 100 mg once daily + isoniazid 300 mg daily + pyridoxine 25 mg daily
D. Azithromycin 1250 mg once weekly for MAC prophylaxis
Reveal Answer
Answer: C. Dapsone 100 mg once daily + isoniazid 300 mg daily + pyridoxine 25 mg daily
At CD4 185 cells/µL, this patient requires: (1) PCP/Toxoplasma prophylaxis (NACO threshold <250) — co-trimoxazole is first-line but she has a sulfa allergy; dapsone 100 mg daily is the appropriate alternative for PCP prophylaxis. (2) IPT — isoniazid 300 mg daily × 36 months + pyridoxine 25 mg to prevent peripheral neuropathy — indicated for all PLHIV with negative active TB screen. Fluconazole pre-emptive therapy is for CrAg-positive patients at CD4 <100 — not applicable here. MAC prophylaxis (azithromycin) is indicated at CD4 <50, not at 185. No prophylaxis is incorrect — at CD4 <250, PCP prophylaxis is mandated by NACO guidelines.
Self-Assessment: Integrating HIV Treatment Decisions
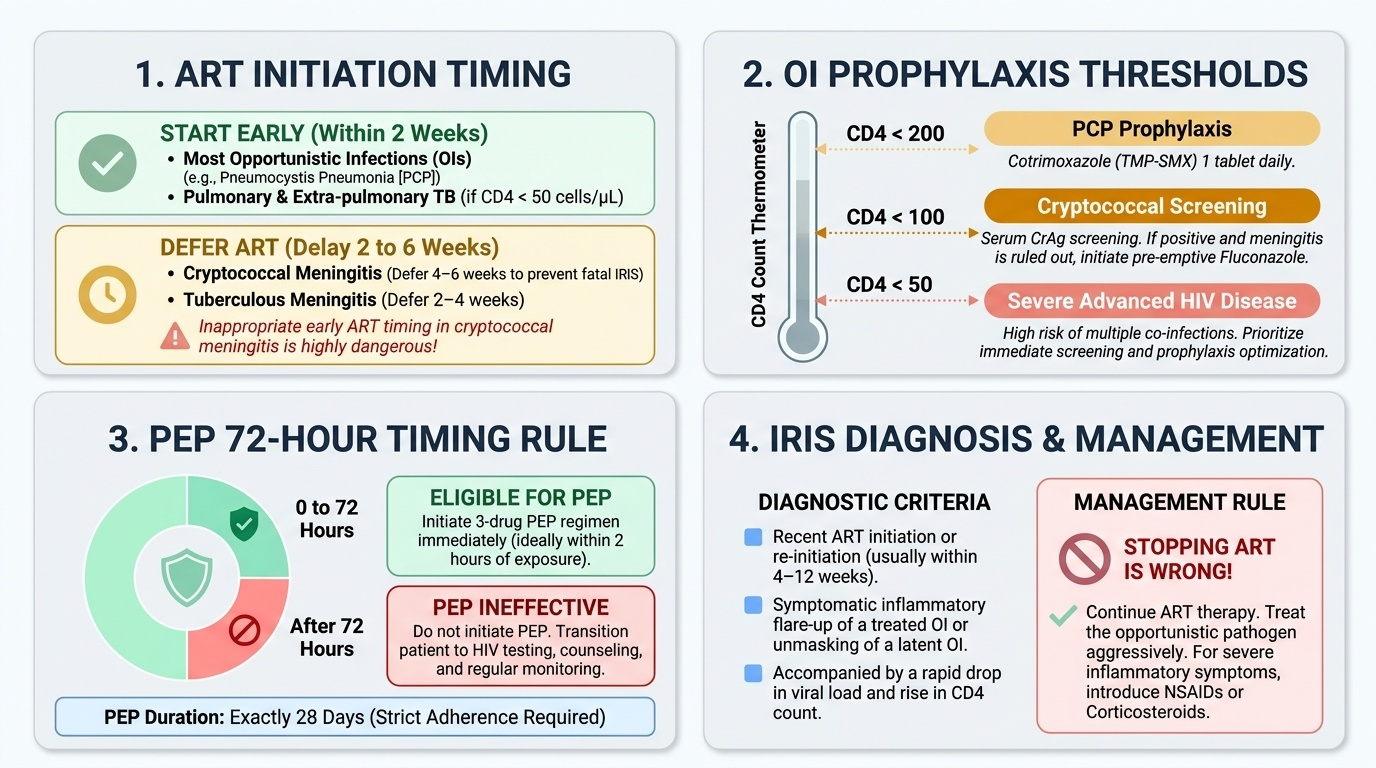
The following scenarios integrate the treatment principles across ART initiation, IRIS management, PEP, and OI prophylaxis. Each scenario requires you to apply the management framework constructed across this module before reading the analysis. The clinical decisions in HIV treatment are often time-critical — delayed PEP is ineffective; inappropriate ART timing in cryptococcal meningitis is dangerous; stopping ART for IRIS is almost always wrong. Consolidating these decision rules through clinical scenario practice prepares you for both examination success and safe clinical practice in any setting in India. Work through each scenario independently, identify the single most important management decision, and then verify against the analysis. The scenarios below are drawn from real clinical encounter types in Indian ART centres and district hospitals. They test not just factual recall but clinical reasoning under uncertainty — the ability to make the right decision when the full information set is not yet available. Notice that in each scenario the decision is not 'what treatment exists for this condition' but 'which decision must I make right now, and what is the evidence behind that decision?' This distinction marks the KH level of competence these competencies require.
Provided image
Scenario A — ART timing: A 42-year-old HIV-positive man is diagnosed with cryptococcal meningitis (CSF India ink positive, CrAg positive). His CD4 count is 38 cells/µL. He is started on Amphotericin B + flucytosine. His wife asks whether ART should be started immediately. When should ART be initiated, and why?
Analysis: ART should be deferred for 4–6 weeks (approximately 5 weeks) after starting antifungal therapy in cryptococcal meningitis. This is the single most important exception to the 'start ART as soon as possible' rule. Early ART in cryptococcal meningitis (within 1–2 weeks of antifungal induction) significantly increases the risk of cryptococcal IRIS, which is associated with high mortality due to raised intracranial pressure and CNS inflammation. The antifungal induction phase must be completed and the antigen burden reduced before immune reconstitution begins. Continue Amphotericin B + flucytosine × 2 weeks → fluconazole consolidation → start ART at ~5 weeks.
Scenario B — IRIS diagnosis: A 30-year-old woman with HIV and pulmonary TB started ART (TLD) 3 weeks ago after 4 weeks of TB treatment. Her CD4 has risen from 55 to 120 cells/µL. She now presents with high fever, worsening cough, and a new CXR showing increased bilateral infiltrates and hilar lymphadenopathy. Her sputum CBNAAT is negative for MTB. What is the diagnosis, and what is the management?
Analysis: Paradoxical TB-IRIS — clinical worsening of TB features (worsening CXR, fever, hilar lymphadenopathy) occurring 3 weeks after ART initiation, with evidence of immune reconstitution (CD4 rising, viral load suppressing), and negative sputum CBNAAT (no new drug resistance or new TB). Management: continue both ART and anti-TB therapy (never stop ART for IRIS). For moderate-to-severe IRIS (worsening CXR + systemic features): add prednisolone 1 mg/kg/day × 4 weeks then taper.
Scenario C — PEP: A 26-year-old nurse sustains a deep needlestick injury from an HIV-positive patient (viral load 14,000 copies/mL) at 10 pm. She comes to the casualty department 3 hours later. What is the immediate management? What is the duration of therapy, and when should she be retested for HIV?
Analysis: Immediately start PEP (exposure was 3 hours ago — well within 72-hour window). Wash the wound thoroughly with soap and water. Baseline HIV test (to confirm she is currently HIV-negative). Start TDF + 3TC + DTG once daily × 28 days (NACO preferred PEP regimen). Report to occupational health. Retest HIV at 6 weeks and 3 months post-exposure. During the 3-month window: use barrier contraception, avoid blood/organ donation. Counsel on adherence — incomplete PEP course significantly reduces efficacy.
CLINICAL PEARL
Three treatment pearls that are frequently tested and clinically critical. First: never stop ART for IRIS — the instinct to 'wait for the inflammation to settle' by pausing ART is wrong; ART must be continued; the inflammation is managed with NSAIDs or corticosteroids, and the immune reconstitution that causes IRIS is the goal of treatment, not a complication. Second: PEP is a 72-hour clock — every hour of delay reduces efficacy; the most common clinical error is to 'wait until morning' when a needlestick occurs at night; PEP starter packs should be available in every casualty department. Third: the NACO first-line regimen is now TLD (not TLE) — if you attribute efavirenz-related CNS side effects to the current regimen, you are working from an outdated mental model; know the composition of TLD (TDF + 3TC + DTG) and its key safety considerations (TDF renal monitoring, DTG caution in first trimester).