Page 7 of 23
IM7.8-10 | Rheumatologic Clinical Evaluation — SDL Guide (Part 3)
Self-Assessment: Clinical Evaluation in Practice
Having worked through the structured history framework, the GALS examination, regional joint examination techniques, skin and muscle assessment, and the approach to differential diagnosis generation, this self-assessment section tests your ability to integrate these skills in clinical vignettes. For each vignette, identify the key history features, the examination findings that confirm or refute the working diagnosis, and the differential diagnosis ranked by probability and urgency. This mirrors the IM7.10 competency standard — generating and prioritising a differential diagnosis based on clinical features that suggest a specific aetiology. Do not reach for investigations before completing the clinical reasoning step; the goal is to demonstrate that the history and examination alone can generate a high-confidence working diagnosis in the majority of rheumatologic presentations, with investigations used to confirm rather than replace clinical assessment.
Provided image
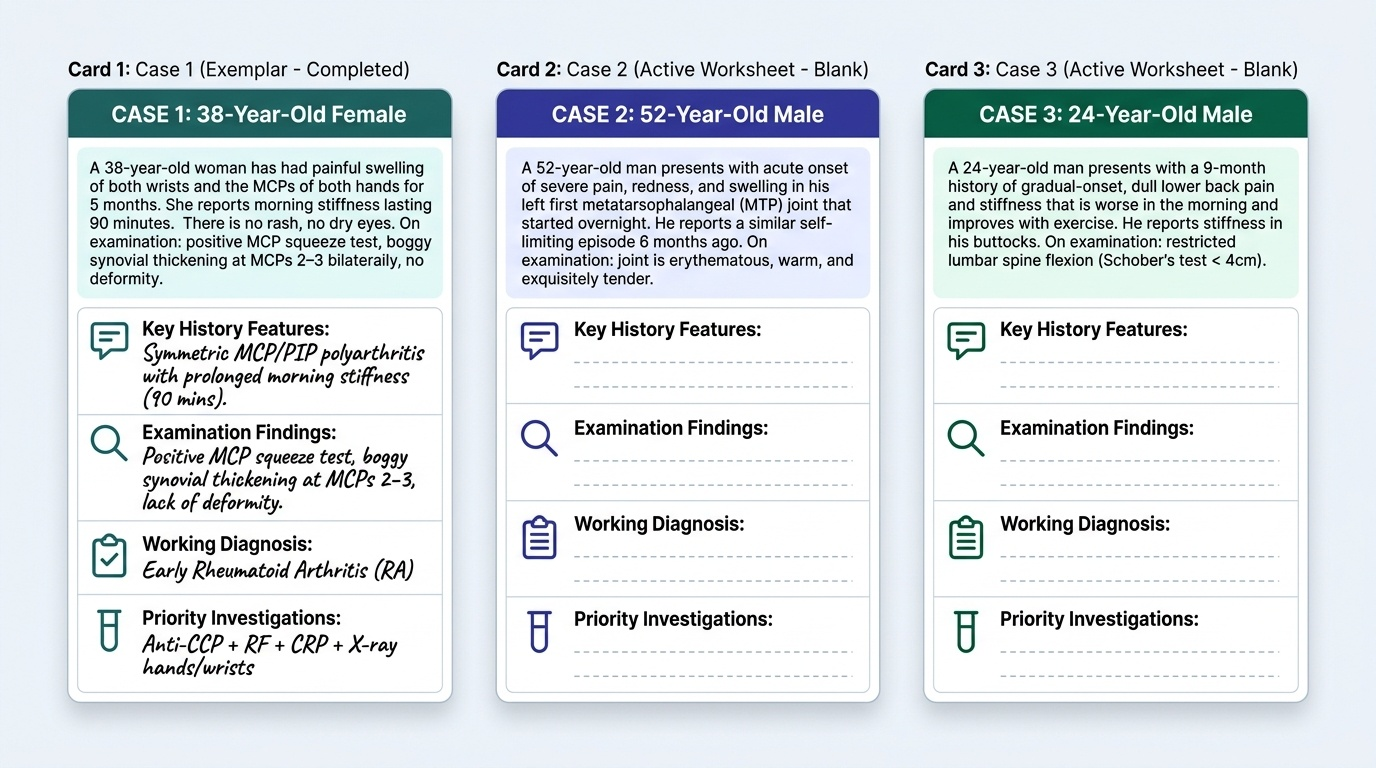
Case 1: A 38-year-old woman has had painful swelling of both wrists and the MCPs of both hands for 5 months. She reports morning stiffness lasting 90 minutes. There is no rash, no dry eyes. On examination: positive MCP squeeze test, boggy synovial thickening at MCPs 2–3 bilaterally, no deformity. Key history feature: symmetric MCP/PIP polyarthritis with prolonged morning stiffness. Working diagnosis: early RA. Next investigation: anti-CCP + RF + CRP + X-ray hands/wrists.
Case 2: A 22-year-old man has right knee swelling for 2 days with inability to fully extend the knee. He has fever (38.4°C). The knee is hot, red, and extremely tender. ESR 86 mm/h, CRP 96 mg/L. No other joints involved. Key history feature: acute monoarthritis + fever + inability to weight-bear. Priority action: arthrocentesis THAT DAY — synovial fluid for cell count, Gram stain, culture, crystal analysis; start empirical antibiotics (IV cloxacillin) after aspiration. Do NOT inject steroid. Working diagnosis: septic arthritis until proven otherwise.
Case 3: A 50-year-old man presents with a 2-day history of excruciating pain, redness, and swelling of the right first MTP joint — it started overnight after a dinner party. He cannot bear the bed sheet touching the foot. He is on hydrochlorothiazide for hypertension. ESR 55 mm/h, serum uric acid 9.2 mg/dL. Key history feature: acute podagra + hyperuricaemia + diuretic use. Working diagnosis: acute gout. Immediate management: NSAIDs (e.g., indomethacin) or colchicine (within 24 hours); do NOT start allopurinol during the acute attack.
CLINICAL PEARL
The MCP squeeze test is the single most useful bedside sign for early rheumatoid arthritis. Squeeze firmly across the metacarpal heads of both hands simultaneously — tenderness on transverse compression is a very sensitive sign of MCP synovitis, detectable even before visible swelling has developed. It takes 5 seconds and costs nothing. Similarly, the metatarsal squeeze test (same manoeuvre across the metatarsal heads of the foot) detects early MTP synovitis — a sign that is pathognomonic of RA when present in a patient with hand synovitis, because the MTP joints are the second most commonly affected site in early RA after the hand.
A second pearl: in any patient presenting with acute severe monoarthritis, the primary duty of care is to exclude septic arthritis before any other diagnosis is entertained. Septic arthritis destroys a joint within days. The investigation is arthrocentesis — synovial fluid for Gram stain, culture, cell count, and crystal analysis. Empirical antibiotics (IV cloxacillin for Staph coverage, adjusted as per local antibiogram) must be started after aspiration while awaiting culture. Never give intra-articular steroids before excluding infection.