Page 11 of 23
IM7.11-13 | Rheumatologic Diagnostic Testing — SDL Guide (Part 3)
Self-Assessment: Integrating Rheumatologic Diagnostics
This self-assessment section tests your ability to select, order, and interpret rheumatologic investigations correctly — integrating the hypothesis-driven test selection framework, autoantibody interpretation rules, synovial fluid analysis, and radiograph interpretation covered in this module. Work through each case systematically before reading the analysis. The key skill being tested is the application of the three governing principles: pre-test probability first, integration not isolation, and specificity for confirmation versus sensitivity for screening.
Self-Assessment A: A 45-year-old man presents with recurrent attacks of severe left first MTP joint pain (3 episodes in the past year, each lasting 5–7 days and resolving completely). He drinks 3–4 units of alcohol daily. Between attacks, examination is normal. Serum uric acid is 8.4 mg/dL. X-ray of the left foot shows no erosions. Which investigation would you perform to definitively confirm the diagnosis during an acute attack, and what would you expect to find?
Analysis: The clinical pattern (recurrent acute monoarthritis of the first MTP joint in a man with alcohol use, hyperuricaemia, intercritical normality) is essentially diagnostic of gout. However, the definitive diagnostic test is synovial fluid aspiration during an acute attack with polarised light microscopy. Expected finding: needle-shaped, negatively birefringent monosodium urate crystals — yellow when aligned parallel to the compensator's slow axis. The absence of erosions on plain X-ray is expected in early/recurrent gout; erosions appear in chronic tophaceous gout. Note: do not delay treatment waiting for a crystal result in a classic presentation — begin NSAIDs or colchicine clinically while aspiration is arranged if possible.
Self-Assessment B: A 32-year-old woman presents with 6 months of fatigue, bilateral wrist pain, and three episodes of painless oral ulcers. CBC: haemoglobin 10.2 g/dL (normocytic), total WBC 3,400/μL (lymphocytes 700/μL), platelets 112,000/μL. ESR 64 mm/h. Urine dipstick: 2+ protein, 1+ blood. ANA positive 1:1280 (homogeneous pattern). What specific antibodies should you test next, and why is the CBC highly significant?
Analysis: The clinical picture strongly suggests SLE — oral ulcers, arthritis, fatigue. The CBC is highly significant: lymphopenia (<1,500/μL) is a classification criterion for SLE (SLICC 2012), as is thrombocytopenia and haemolytic anaemia. The combination of lymphopenia + thrombocytopenia + normocytic anaemia + proteinuria + haematuria in a young woman with constitutional symptoms and oral ulcers is a compelling clinical picture for SLE with possible renal involvement. Next investigations: anti-dsDNA (for confirmation and disease-activity monitoring), anti-Sm (highly specific), complement C3/C4 (if both low, highly supportive of active SLE with immune complex deposition), urine microscopy for red cell casts (to classify lupus nephritis severity — determines treatment intensity), and 24-hour urine protein or spot PCR ratio.
Self-Assessment C: A 55-year-old man presents with X-ray of both hands performed as part of a rheumatology referral. Key findings: periarticular osteopenia at the MCPs and PIPs bilaterally, symmetric joint space narrowing at MCP 2 and 3 bilaterally, and a small marginal erosion at the radial aspect of the right 2nd MCP 'bare area'. His RF is weakly positive (slightly above ULN), anti-CCP is positive at 6× ULN, ESR 45 mm/h. What do the X-ray findings indicate, and what is the significance of the high-titre anti-CCP?
Analysis: The X-ray findings — periarticular osteopenia, symmetric small-joint space narrowing, and marginal erosion at the bare area — are diagnostic features of erosive RA. The presence of even a single erosion confirms structural joint damage and indicates that DMARD therapy is urgently needed to prevent further damage. The high-titre anti-CCP (>3× ULN) is an adverse prognostic marker associated with a greater risk of progressive joint destruction — this patient needs early aggressive treatment. The ACR/EULAR 2010 score: large joint involvement (0) + small joints (MCP/PIP = score 2) + anti-CCP high positive (score 3) + elevated ESR (score 1) + duration unknown (likely >6 weeks from the erosion = score 1) = total ≥7, which comfortably classifies as definite RA.
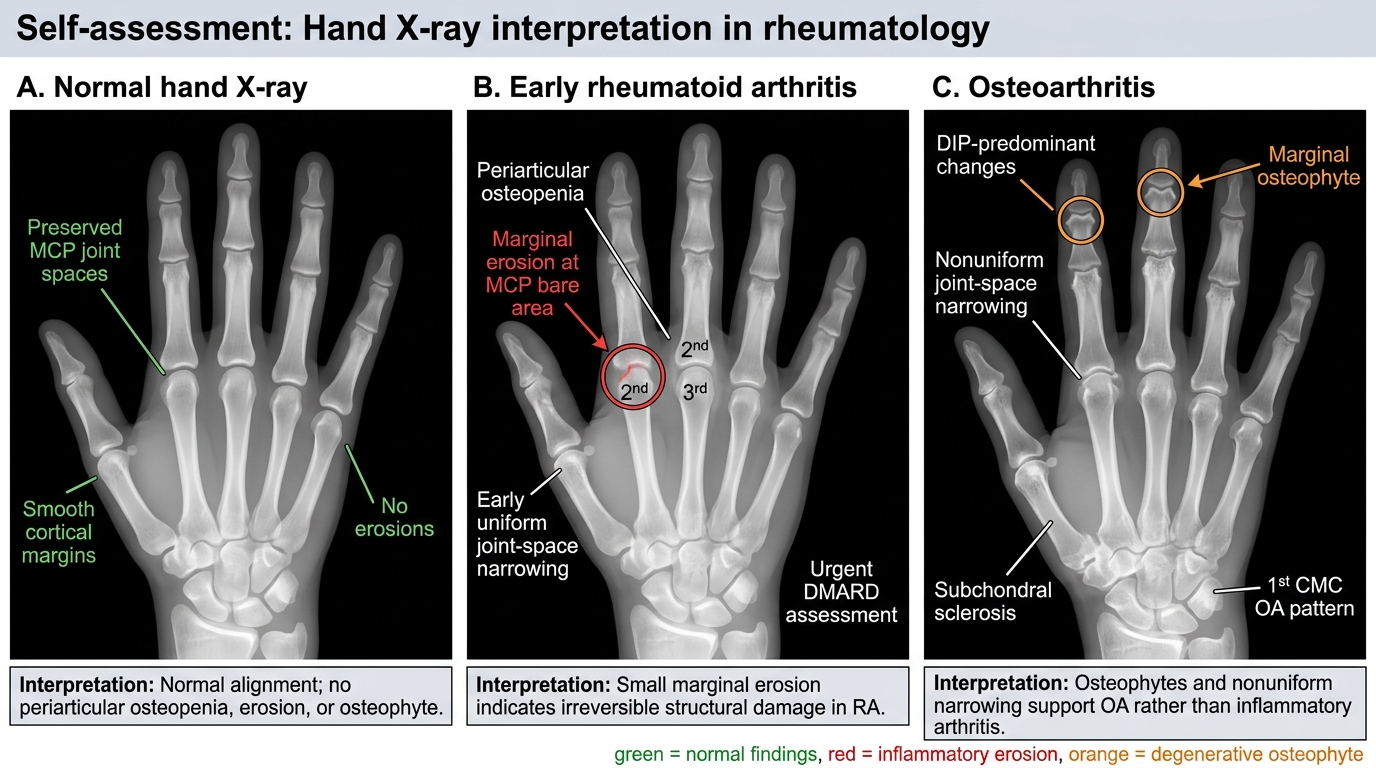
Hand X-ray Interpretation: Normal, Early RA, and OA
CLINICAL PEARL
The three most important clinical pearls in rheumatologic diagnostic testing are:
- Serum uric acid can be NORMAL during an acute gout attack. The inflammatory stress response of the acute attack increases renal uric acid excretion, temporarily lowering serum levels. A normal uric acid during an acute severe monoarthritis at the first MTP joint does NOT exclude gout — synovial fluid crystal analysis is the definitive test.
- ANA is a screening test, not a diagnostic test for SLE. It is positive in 95% of SLE patients (high sensitivity) but also in 5–15% of healthy people and many other diseases (low specificity). Always interpret ANA against the clinical context and follow with specific antibodies (anti-dsDNA, anti-Sm) before making the diagnosis of SLE.
- Erosions on joint X-ray indicate irreversible structural damage in RA and mandate urgent DMARD therapy. The presence of even a single small marginal erosion at the MCP 'bare area' changes the management urgency. This is why baseline X-rays at the time of RA diagnosis and periodic repeat imaging (every 1–2 years) are part of standard rheumatology monitoring. MRI is more sensitive for early erosions when X-rays are still normal.