Page 1 of 23
IM7.1-7 | Rheumatologic Disease Foundations — SDL Guide
Learning Objectives
- Describe the pathophysiology and genetic basis of autoimmune rheumatic diseases including HLA associations
- Classify causes of joint pain by pathophysiology — inflammatory vs mechanical, articular vs periarticular
- Discriminate acute, subacute, and chronic causes of joint pain
- Distinguish arthralgia from arthritis and describe the cardinal signs of synovitis
- Describe the common signs of articular and periarticular diseases including specific hand deformities
- Describe the systemic manifestations of rheumatologic disease across skin, eyes, kidneys, lungs, and cardiovascular system
- Develop a systematic clinical approach to joint pain
- Outline treatment principles for RA, SLE, gout, and seronegative spondyloarthropathies
INSTRUCTIONS
This module builds the conceptual foundation for all rheumatologic clinical work. Master the inflammatory vs mechanical distinction, the compartment-based classification of joint pain, the systemic manifestations that make rheumatic diseases multi-organ conditions, and the management principles. This framework underpins both bedside diagnosis and rational use of investigations.
References
- Harrison's Principles of Internal Medicine, 21st ed., Chapters 351–366 — Rheumatology (textbook)
- API Textbook of Medicine, 10th ed., Chapters on Rheumatic Diseases (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Chapter 26 — Musculoskeletal disease (textbook)
- ACR/EULAR Classification Criteria for RA, 2010 (guideline)
- EULAR Recommendations for the management of RA, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Ramesh is a 35-year-old schoolteacher who wakes up one morning unable to make a fist. His fingers are swollen, warm, and stiff — and the stiffness lasts nearly two hours before it eases. His wife has noticed he seems fatigued and has lost weight over the past six weeks. At the local clinic, the doctor suspects 'arthritis' and prescribes a painkiller. Two months later, Ramesh returns — now unable to hold a pen, with X-rays showing erosions at the MCP joints. Contrast this with Sunita, a 60-year-old retired cook whose knees have ached for years, worse on climbing stairs, with bony swellings at the finger joints and no morning stiffness beyond 20 minutes. Both patients say 'my joints hurt' — but the underlying biology, the urgency of diagnosis, and the treatment are entirely different. The difference between recognising inflammatory arthritis (Ramesh) and mechanical/degenerative disease (Sunita) early enough to intervene is a skill built on foundations: understanding the pathophysiology of joint disease, the patterns that distinguish aetiology, and the systemic connections that make rheumatology not merely a joint specialty but a window into the whole body.
WHY THIS MATTERS
Rheumatologic diseases — spanning autoimmune, crystal, degenerative, and infectious aetiologies — account for a substantial portion of outpatient medicine in India. Rheumatoid arthritis affects approximately 0.5–1% of the adult Indian population, while osteoarthritis is nearly universal after the sixth decade. Systemic lupus erythematosus disproportionately affects young women of reproductive age. Septic arthritis, gout, and reactive arthritis are frequent presentations in emergency and general medicine settings. The NMC competency set for IM7.1–IM7.7 requires you not only to know these conditions but to build a systematic mental model: classify joint pain by pathophysiology, distinguish inflammatory from mechanical disease at the bedside, recognise articular from periarticular disease, and identify systemic manifestations that indicate multi-organ autoimmune disease. This foundational SDL lays the conceptual framework that every subsequent clinical encounter in rheumatology will depend upon.
RECALL
Before exploring rheumatologic disease, revisit two foundations from earlier learning. First, the structure of a synovial joint: articular cartilage covering bone ends, a synovial membrane (a thin vascular lining producing synovial fluid), an outer fibrous capsule, supporting ligaments, and the surrounding periarticular structures — tendons, bursae, and entheses (the insertions of tendons and ligaments into bone). The synovial fluid normally is acellular and viscous, providing lubrication and nutrition to avascular cartilage. Second, recall the basic immunology of autoimmunity: the immune system normally distinguishes self from non-self through central tolerance (deletion of autoreactive T-cells in the thymus) and peripheral tolerance (Treg cells, anergy). Failure of these mechanisms — due to genetic susceptibility, environmental triggers (infection, UV, hormones), and molecular mimicry — allows autoreactive T-cells and B-cells to attack self-tissues. In the joint, this translates to synovial inflammation, pannus formation, and eventual joint destruction. These two structural and immunological building blocks underpin every concept in this module.
Clinical Presentation of Joint Disease: Classification Framework
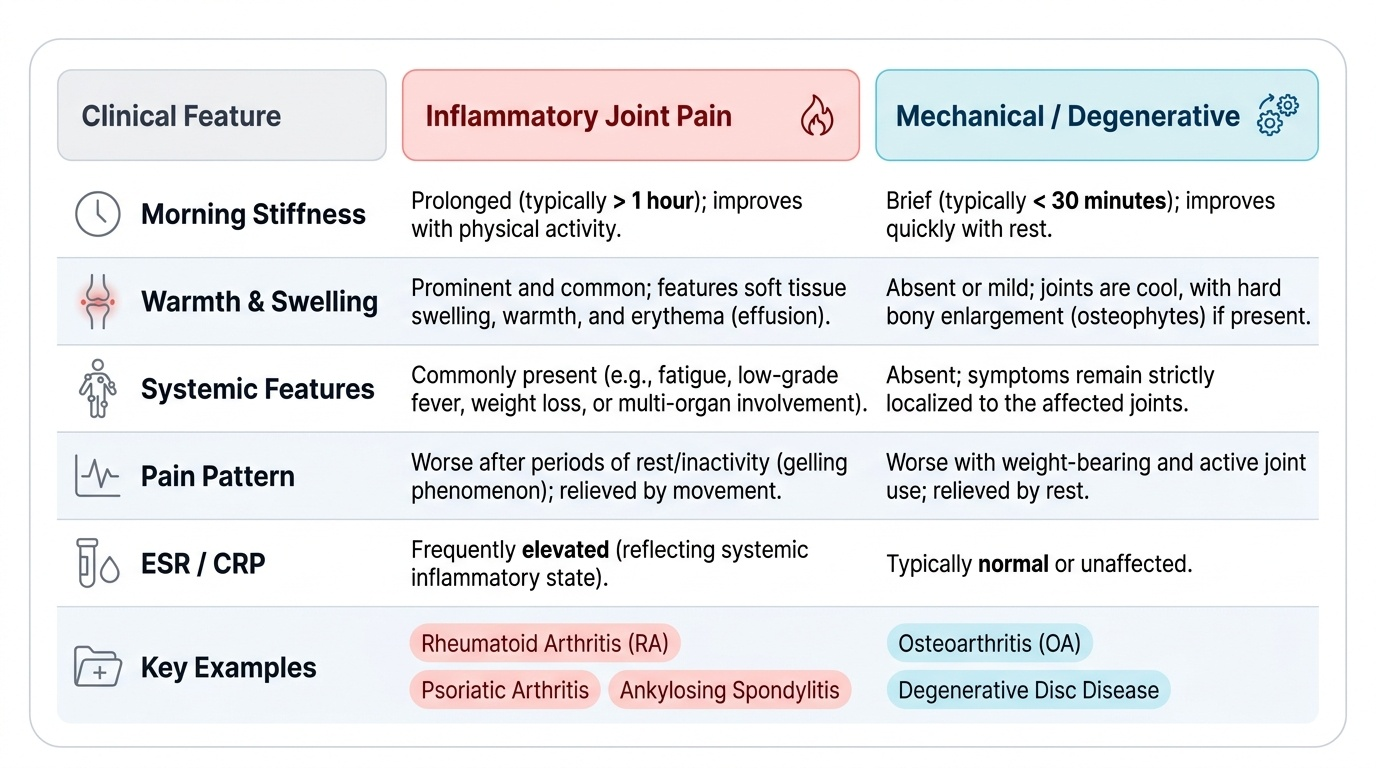
The clinical presentation of joint pain in any patient requires a systematic, pathophysiology-based classification before a differential diagnosis can be constructed. The most important first distinction — and the one that most decisively directs investigation and treatment — is whether the joint pain is inflammatory or mechanical/degenerative in origin. This distinction is made clinically, from the history and examination, before any blood test or imaging result is available, and it is the skill that separates a systematic clinician from one who reflexively orders 'a rheumatology panel'.
Provided image
The second major classification axis concerns the anatomical source of pain: is it articular (arising from within the joint — synovium, cartilage, ligamentous capsule) or periarticular (arising from structures adjacent to the joint — tendons, bursae, entheses, muscle)? This distinction matters because periarticular disease (e.g., rotator cuff tendinitis, trochanteric bursitis, De Quervain tenosynovitis) is not arthritis and should not be treated as such. The clinical sign is that in periarticular disease, passive joint movement is typically preserved while specific active movements that stress the affected periarticular structure are painful; in true arthritis, both active and passive movement are painful because the joint itself is inflamed.
The third axis is temporal pattern: acute (days to weeks), subacute (weeks to 3 months), or chronic (>3 months). Acute monoarthritis demands immediate differentiation of septic arthritis and crystal disease from other causes. Chronic symmetrical polyarthritis with morning stiffness >1 hour has a profoundly different differential from acute asymmetric oligoarthritis following a genitourinary infection.
Arthralgia versus arthritis is a fundamental distinction. Arthralgia means joint pain without objective evidence of inflammation — no warmth, no swelling, no limited ROM, normal synovial fluid. It is a subjective symptom only. Arthritis implies joint pain with objective signs of synovial inflammation: warmth, swelling (effusion or synovial thickening), tenderness on palpation, and often limited range of motion. The distinction matters clinically: arthralgia alone (as in early SLE or viral illness) does not require disease-modifying therapy; arthritis with synovitis does. Never label a patient as having 'arthritis' solely on the basis of joint pain — confirm the objective signs.
Acute versus subacute versus chronic: the temporal classification guides urgency:
- Acute (<6 weeks): septic arthritis (emergency, requires same-day arthrocentesis and antibiotics), gout, pseudogout, reactive arthritis, viral arthritis (parvovirus B19, hepatitis B, dengue in India), trauma
- Subacute (6 weeks–3 months): early RA, reactive arthritis resolution, rheumatic fever (acute phase is <6 weeks but constitutional symptoms may persist), early connective tissue disease
- Chronic (>3 months): established RA, OA, psoriatic arthritis, ankylosing spondylitis, SLE, Sjögren syndrome, gout with tophaceous disease, TB arthritis (endemic in India — monoarthritis of weight-bearing joints is the classic presentation)
Inflammatory vs Mechanical Joint Disease: Clinical Discrimination
The distinction between inflammatory and mechanical/degenerative joint disease is one of the most clinically important skills in general medicine, and it can be made with high accuracy from the history alone. The pathophysiological basis of this distinction explains the clinical features: in inflammatory disease, the primary pathology is synovial inflammation (synovitis) driven by immune mechanisms — neutrophils and macrophages infiltrate the synovium, producing cytokines (TNF-α, IL-1β, IL-6, IL-17), prostaglandins, and kinins. These mediators accumulate overnight when the patient is recumbent and cause the characteristic prolonged morning stiffness. As the patient moves, synovial fluid is circulated, warmth reduces, and stiffness eases — but the process resumes with rest. In mechanical disease, the primary pathology is cartilage degradation — the collagen matrix is disrupted, subchondral bone becomes exposed and thickened, osteophytes (bony outgrowths) form, and pain results from mechanical loading on poorly cushioned joint surfaces. There is minimal active synovitis, so morning stiffness (from joint gelling) lasts typically less than 30 minutes and worsens with use rather than improving.
Key discriminating features in the history and examination:
Morning stiffness: inflammatory arthritis produces stiffness lasting ≥1 hour (often 2 hours or more in active RA); mechanical disease produces stiffness <30 minutes ('gelling' after rest that quickly eases with movement).
Pain pattern: inflammatory pain is worse at rest and after inactivity, improving with gentle movement (the paradox of inflammatory arthritis — movement helps). Mechanical pain is worse with use, improves with rest.
Warmth and swelling: true synovitis in inflammatory arthritis produces warmth (detectable by the back of the examiner's hand) and swelling (either effusion — fluctuant, crosses the joint line — or synovial thickening — rubbery, boggy). Mechanical OA may produce a cool effusion (non-inflammatory fluid) but typically without significant warmth.
Joint distribution: inflammatory polyarthritis classically involves the small joints of the hands and feet (MCPs, PIPs, MTPs) symmetrically — the pattern of RA. Mechanical OA preferentially involves weight-bearing joints (knee, hip, first MTP) and the DIP joints (Heberden's nodes). The MCP joint is the cardinal joint of RA and is rarely primarily involved in OA — a swollen, tender MCP joint should always prompt consideration of inflammatory disease.
Systemic features: inflammatory rheumatic diseases produce constitutional symptoms — fever (low-grade), weight loss, fatigue, anaemia of chronic disease, elevated ESR and CRP — reflecting systemic cytokine activity. Mechanical disease is typically confined to the musculoskeletal system with no systemic inflammation.
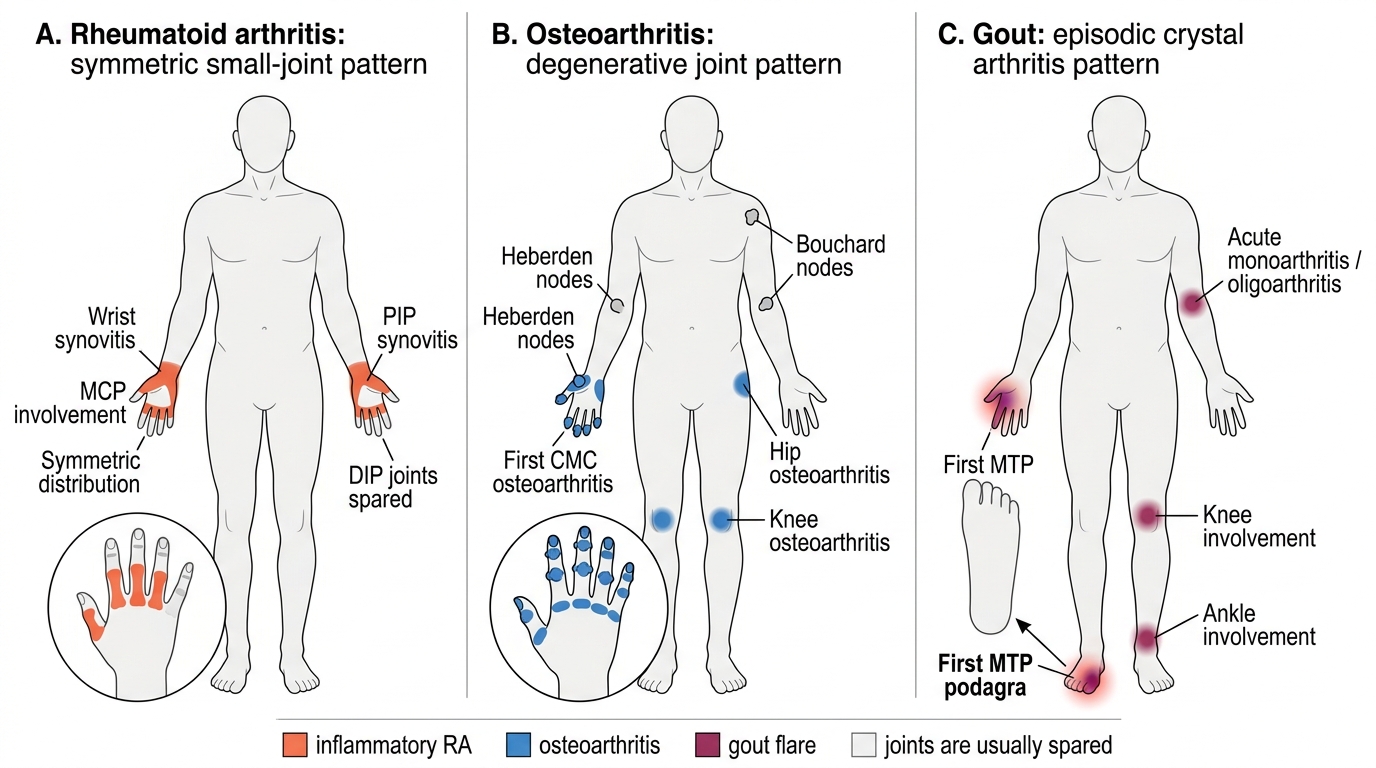
Joint Distribution Patterns in RA, Osteoarthritis, and Gout
Articular versus periarticular disease: in practice, the most efficient discrimination is by examining ROM. True joint inflammation causes pain and restriction on both active AND passive movement in multiple planes. Periarticular disease (tendinitis, bursitis) causes pain on specific active movements (the ones that stress the involved structure) while passive movement is preserved. For example: in rotator cuff tendinitis, passive abduction by the examiner is relatively painless while active abduction against resistance is painful — the joint ROM is preserved. In trochanteric bursitis, the hip joint ROM is fully preserved; there is focal tenderness over the greater trochanter. In De Quervain tenosynovitis (first extensor compartment), the Finkelstein test (ulnar deviation with the thumb enclosed in the fist) is positive — not a joint sign. Making this distinction prevents the mis-diagnosis of bursitis as arthritis and the inappropriate use of DMARDs.
Signs and Symptoms of Articular and Periarticular Disease
A precise vocabulary of articular and periarticular signs is necessary to document findings accurately and communicate them to colleagues and consultants. The clinical examination of joints must be systematic and comprehensive — every final-year student should be able to examine the hands, wrists, elbows, shoulders, hips, knees, ankles, and feet in a structured way, distinguishing the physical findings that indicate different pathological processes. The examination has two goals: first, to confirm that the patient's complaint arises from the joint itself and not from adjacent periarticular structures; and second, to characterise the nature of any joint pathology — whether it reflects active synovitis, structural deformity from past inflammation, or mechanical wear-and-tear changes. Accurate recording of these findings is the basis for monitoring disease activity over time and judging treatment response. The signs below form the vocabulary of this examination — master them not as a list to memorise but as physical correlates of the pathological processes described in the preceding sections. Each sign has a mechanistic explanation that links it to the underlying disease process.
Cardinal signs of synovitis (joint inflammation):
- Warmth: detected by the dorsum of the examiner's hand, comparing the inflamed joint to the contralateral side and to adjacent non-inflamed skin. The warmth of acute septic arthritis or gout is often striking; in RA it is moderate.
- Swelling: may be from (a) synovial effusion — fluctuant, crossing the joint line, detectable by the bulge sign (small effusion, knee) or patellar tap (large effusion); or (b) synovial thickening — boggy, rubbery, not fluctuant, found on the medial and lateral aspects of the joint and the MCP/PIP joint dorsum in RA.
- Tenderness: MCP joints are squeezed across the row (metacarpal squeeze test); individual PIPs and DIPs are palpated. Tenderness at the joint line is articular; tenderness at tendon insertions or 1–2 cm away from the joint margin is periarticular.
- Restricted range of motion: measured with a goniometer for documentation and monitoring disease progression.
Hand signs specific to rheumatic diseases:
- Heberden's nodes (OA): bony swellings at DIP joints, hard, non-tender in established disease
- Bouchard's nodes (OA): bony swellings at PIP joints
- Swan-neck deformity (RA): PIP hyperextension + DIP flexion — from volar plate laxity at PIP and extensor tendon tightening
- Boutonnière deformity (RA): PIP flexion + DIP hyperextension — from central slip rupture of the extensor tendon
- Z-thumb (RA/SLE): flexion at IP joint + hyperextension at MCP joint of thumb
- Ulnar deviation of fingers at MCPs (RA): characteristic finger drift toward the ulnar side
- Jaccoud's arthropathy (SLE): reducible, non-erosive ulnar deviation — UNLIKE RA which produces fixed erosive deformity
- Telescoping digits (psoriatic arthritis — arthritis mutilans): severe bone resorption with 'opera glass' digit appearance
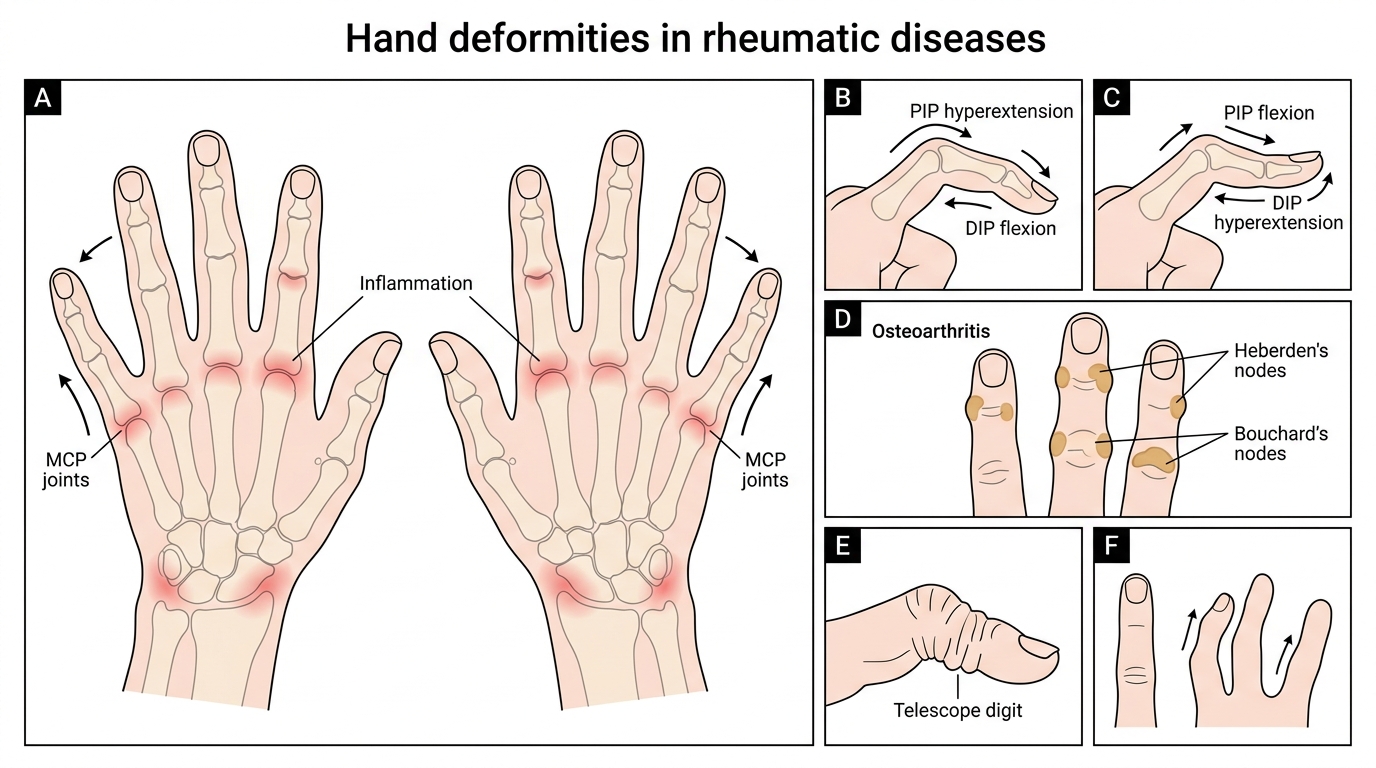
Hand Deformities in Rheumatic Diseases
Periarticular signs:
- Bursitis: localised, fluctuant, tender swelling over a bursa — prepatellar (housemaid's knee), olecranon (gout, RA, septic), subacromial/subdeltoid, trochanteric
- Tendinitis/tenosynovitis: pain on resisted active movement of the involved tendon; crepitus may be felt; the overlying tendon sheath may be swollen in tenosynovitis (De Quervain, flexor tenosynovitis in RA)
- Enthesitis: tenderness at the bone insertion of a tendon or ligament — Achilles tendon insertion, plantar fascia origin, greater trochanter, patella; a hallmark of spondyloarthropathies (psoriatic arthritis, ankylosing spondylitis, reactive arthritis)
- Dactylitis ('sausage digit'): diffuse swelling of an entire digit (finger or toe) — ALL synovial structures involved (flexor tendon sheath + all IP joints); characteristic of spondyloarthropathies, particularly psoriatic arthritis and reactive arthritis
SELF-CHECK
A 32-year-old woman presents with bilateral wrist and MCP joint pain. She reports stiffness lasting 2 hours each morning, joint swelling, fatigue, and weight loss over 3 months. Which single feature most strongly distinguishes inflammatory from mechanical arthritis?
A. Bilateral distribution of joint involvement
B. Morning stiffness lasting ≥1 hour
C. Presence of joint swelling
D. Elevated serum uric acid
Reveal Answer
Answer: B. Morning stiffness lasting ≥1 hour
Morning stiffness lasting ≥1 hour (often >2 hours in active RA) is the most specific feature distinguishing inflammatory arthritis from mechanical/degenerative disease. Mechanical OA causes stiffness typically lasting <30 minutes ('gelling' after inactivity, not morning stiffness). Bilateral distribution can occur in both. Joint swelling indicates arthritis but does not distinguish inflammatory from mechanical. Uric acid elevation is not diagnostic of gout and can be asymptomatic; gout is characteristically monoarticular and acute rather than bilateral and chronic.