Page 13 of 23
IM7.{14-20,22} | Rheumatologic Disease Management — SDL Guide
Learning Objectives
- Communicate a rheumatologic diagnosis and treatment plan clearly to the patient using a structured communication framework (IM7.14)
- Develop an appropriate, disease-specific treatment plan for RA, AS, SLE, and crystal arthropathies (IM7.15)
- Prescribe and communicate correct medications for joint pain and crystalline arthropathy with appropriate doses and safety precautions (IM7.16)
- Prescribe and communicate treatment for systemic rheumatologic conditions including SLE and RA (IM7.17)
- Describe the pathophysiological basis and mechanism of action of conventional DMARDs, biologic DMARDs, and JAK inhibitors (IM7.18)
- Incorporate patient preferences regarding treatment route, cost, fertility, and monitoring burden into the management plan (IM7.19)
- Establish and communicate a monitoring plan covering disease activity, drug toxicity, and complication screening (IM7.20)
- Determine when specialist rheumatology referral is indicated (IM7.22)
INSTRUCTIONS
Rheumatologic disease management requires integrating pharmacological knowledge, patient communication, monitoring protocols, and referral decision-making. This module focuses on the management arc — diagnosis communication through prescribing through monitoring through referral. Apply the treat-to-target principle and the prescribing safety rules (TB screen before biologics, folic acid with methotrexate, allopurinol timing in gout) at every clinical encounter.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 354 — Rheumatoid Arthritis; Ch. 356 — SLE; Ch. 365 — Gout (textbook)
- API Textbook of Medicine, 10th ed. — Rheumatology: Management of RA, SLE, Crystal Arthropathies (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 26 — Treatment of Rheumatic Diseases (textbook)
- EULAR Recommendations for RA Management 2022 — Smolen et al., Annals of Rheumatic Diseases (guideline)
- ACR 2020 Guideline for Management of Gout — FitzGerald et al., Arthritis & Rheumatology (guideline)
- EULAR Recommendations for SLE Management 2023 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mrs Lakshmi, a 38-year-old primary school teacher, was diagnosed with rheumatoid arthritis six months ago. She has already lost partial grip strength in both hands and has begun making errors writing on the blackboard. Her husband brings her to clinic with a printout of a news article claiming that fish oil and turmeric can cure arthritis. She is worried about side effects of 'strong medicines' and has delayed starting treatment. Her EULAR score from last visit showed high disease activity — DAS28 score of 5.8. Meanwhile, in the adjacent consultation room, a 26-year-old man with ankylosing spondylitis who did not receive NSAIDs four years ago now has a fused lumbar spine visible on X-ray and walks with a rigid forward lean. Both outcomes were preventable. Rheumatologic disease management requires the clinician to communicate the diagnosis clearly, explain the treatment plan including the rationale for disease-modifying drugs, respond to patient concerns and preferences, and ensure the patient understands their monitoring requirements — all while engaging the patient as a partner rather than a passive recipient of prescriptions.
WHY THIS MATTERS
The management competencies for rheumatologic disease (IM7.14–IM7.20, IM7.22) span the full arc of clinical care: communicating diagnosis and treatment plan (IM7.14), developing a treatment plan (IM7.15), prescribing medications for joint pain and crystalline arthropathy (IM7.16), prescribing for systemic conditions (IM7.17), understanding the basis of biologic and DMARD therapy (IM7.18), incorporating patient preferences (IM7.19), establishing follow-up and monitoring (IM7.20), and determining when specialist referral is needed (IM7.22). These competencies are rated SH and KH — reflecting the expectation that final-year students can participate in real management discussions and co-produce a management plan under supervision. In India, rheumatologic diseases carry a high burden of disability and economic loss because many patients present late, DMARDs are initiated late due to patient hesitancy, and monitoring is inconsistent. Acquiring these competencies reduces that gap.
RECALL
Recall the diagnostic patterns from the preceding modules. Rheumatoid arthritis (RA) is a symmetric inflammatory polyarthritis of the small joints characterised by synovial pannus formation, erosive joint destruction, elevated RF and/or anti-CCP, and elevated ESR/CRP. Seronegative spondyloarthropathies (including ankylosing spondylitis) are axial inflammatory arthritides with sacroiliitis, enthesitis, and HLA-B27 association. Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease with ANA positivity and specific organ involvement. Crystal arthropathies — gout (monosodium urate, negatively birefringent crystals) and pseudogout (CPPD, positively birefringent crystals) — are episodic acute arthritides with specific treatments. Osteoarthritis (OA) is a degenerative joint disease treated primarily with non-pharmacological measures and analgesia. The management principles below are disease-specific — treatment is never generic but always tied to the diagnosis and the disease mechanism.
Clinical Presentation and Communication of Diagnosis in Rheumatologic Disease
The clinical presentation of rheumatologic disease has been covered in detail in the preceding modules. This module begins at the point at which a diagnosis has been established and the clinician must communicate it clearly to the patient and begin the management process. Effective communication at this stage is not merely courtesy — it is a competency (IM7.14) that directly determines whether the patient engages with treatment, adheres to their medication regimen, attends for monitoring, and reports side effects promptly. Patients who receive unclear or frightening diagnoses without explanation are more likely to seek unproven complementary therapies, delay filling prescriptions, and default from follow-up — all of which worsen long-term outcomes.
The structured approach to communicating a rheumatologic diagnosis follows the SPIKES protocol (adapted from oncology communication for chronic inflammatory disease): Setting (private, comfortable, unhurried); Perception (what does the patient already know or believe?); Invitation (does the patient want detailed information now?); Knowledge (give information in plain language, without jargon); Empathy (acknowledge the emotional response before proceeding with the plan); Summary and Strategy (what happens next, and when).
Key communication points specific to rheumatologic diseases:
- RA: the condition is lifelong but controllable with appropriate treatment; the goal is disease remission (low disease activity score); joint damage occurs early and is irreversible — this is why starting treatment promptly is important, not optional. Explain that DMARDs are not 'strong medicines' to be feared, but rather medications that specifically target the inflammation driving the damage. The 'window of opportunity' concept — that early treatment in the first 3–6 months of RA reduces long-term disability more effectively than treatment started later — should be explained in accessible terms.
- Ankylosing spondylitis: the spine can stiffen and fuse if inflammation is not suppressed; daily exercise (not bed rest) is a core part of treatment. Unlike RA, exercise improves the pain and reduces fusion risk.
- SLE: the disease is variable and can affect multiple organs; the patient must understand the importance of regular monitoring (blood tests, urine tests, blood pressure) because organ complications (particularly lupus nephritis) may be asymptomatic until advanced.
- Gout: explicitly dispel the misconception that gout is a 'rich man's disease' caused by indulgence; explain the biochemical basis (urate crystal deposition, impaired renal excretion) and the lifestyle and pharmacological strategies for long-term control.
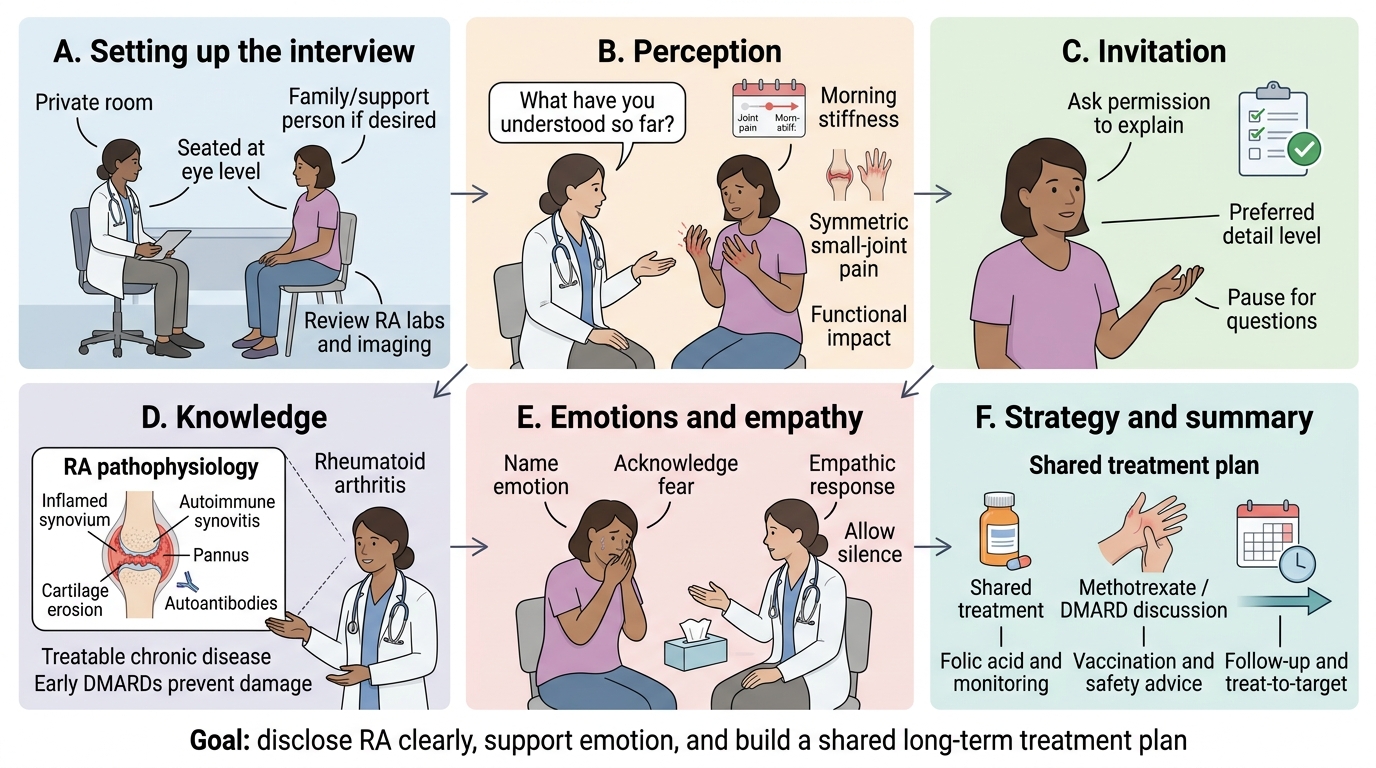
SPIKES Framework for Rheumatoid Arthritis Diagnosis Disclosure
Pathophysiological Basis of Biologic and Disease-Modifying Therapy
Understanding the basis of biologic and disease-modifying therapy (IM7.18) requires understanding the pathophysiology of chronic inflammatory joint disease. In rheumatoid arthritis, the central event is activation of the adaptive immune system — specifically CD4+ T helper cells (Th1 and Th17 subsets) and B cells — within the synovium, leading to the production of inflammatory cytokines, autoantibodies (RF, anti-CCP), and the formation of a destructive synovial pannus. The key cytokines mediating synovial inflammation and joint destruction in RA are tumour necrosis factor-α (TNF-α), interleukin-6 (IL-6), and interleukin-1 (IL-1), along with T cell-mediated direct activation of fibroblast-like synoviocytes that erode cartilage and bone. This molecular understanding has directly produced the modern pharmacological arsenal:
Conventional synthetic DMARDs (csDMARDs) work through broad immunomodulatory mechanisms. Methotrexate (MTX) is the anchor DMARD for RA — it inhibits dihydrofolate reductase, reducing purine and pyrimidine synthesis (anti-proliferative for activated T and B cells) and also has adenosine-mediated anti-inflammatory effects independent of folate metabolism. Because methotrexate reduces folate-dependent pathways, folic acid 5 mg once weekly (on a different day from MTX) is prescribed concurrently to reduce mucositis, hepatotoxicity, and haematological side effects without reducing efficacy. MTX is given at 7.5–25 mg once weekly. Sulfasalazine (5-ASA + sulfapyridine) has combined anti-inflammatory and antibacterial mechanisms; used in RA (especially seronegative), spondyloarthropathies, and inflammatory bowel disease-associated arthritis. Hydroxychloroquine (HCQ) inhibits lysosomal function in macrophages, reducing antigen presentation and cytokine production; used in mild RA and SLE, and is one of the safest long-term immunomodulators.
Biologic DMARDs (bDMARDs) are targeted therapies derived from biologic sources (antibodies, receptor constructs, fusion proteins) that block specific cytokines or immune cell subsets identified from the pathophysiology above. TNF inhibitors — infliximab (chimeric anti-TNF monoclonal antibody, IV), etanercept (soluble TNF receptor fusion protein, SC), adalimumab (fully human anti-TNF, SC), certolizumab, golimumab — block TNF-α directly, preventing its binding to TNF receptors on synoviocytes and macrophages. They produce rapid suppression of synovial inflammation and radiographic progression. IL-6 receptor blockers — tocilizumab, sarilumab — block the IL-6 receptor, reducing acute-phase response (ESR, CRP normalise), joint destruction, and systemic features. T cell co-stimulation blocker — abatacept (CTLA4-Ig fusion protein) — inhibits the CD28-CD80/86 co-stimulatory signal required for T cell activation. B cell depletion — rituximab (anti-CD20 monoclonal antibody) — depletes B cells, reducing autoantibody production; effective in seropositive RA.
Targeted synthetic DMARDs (tsDMARDs) — Janus kinase (JAK) inhibitors (tofacitinib, baricitinib, upadacitinib) — are small molecules that inhibit intracellular JAK-STAT signalling pathways through which multiple cytokines (including IL-6, IL-2, GM-CSF) exert their effects. JAK inhibitors are oral and provide rapid onset of action; they are used in RA where csDMARDs have failed.
Critical pre-treatment screen before all biologics: TB screening. TNF-α is essential for forming and maintaining granulomas that wall off latent tuberculosis (Mycobacterium tuberculosis). TNF inhibitors (and to a lesser extent other biologics and JAK inhibitors) reactivate latent TB — in India, a country with the world's highest TB burden, this screening is non-negotiable. Every patient must have a QUANTIFERON-TB Gold (IGRA) test or Mantoux tuberculin skin test plus a chest X-ray before starting any biologic. Latent TB must be treated with isoniazid preventive therapy (IPT) for 6–9 months (under NTEP guidance) before or concurrent with biologic initiation, depending on the urgency of starting therapy.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
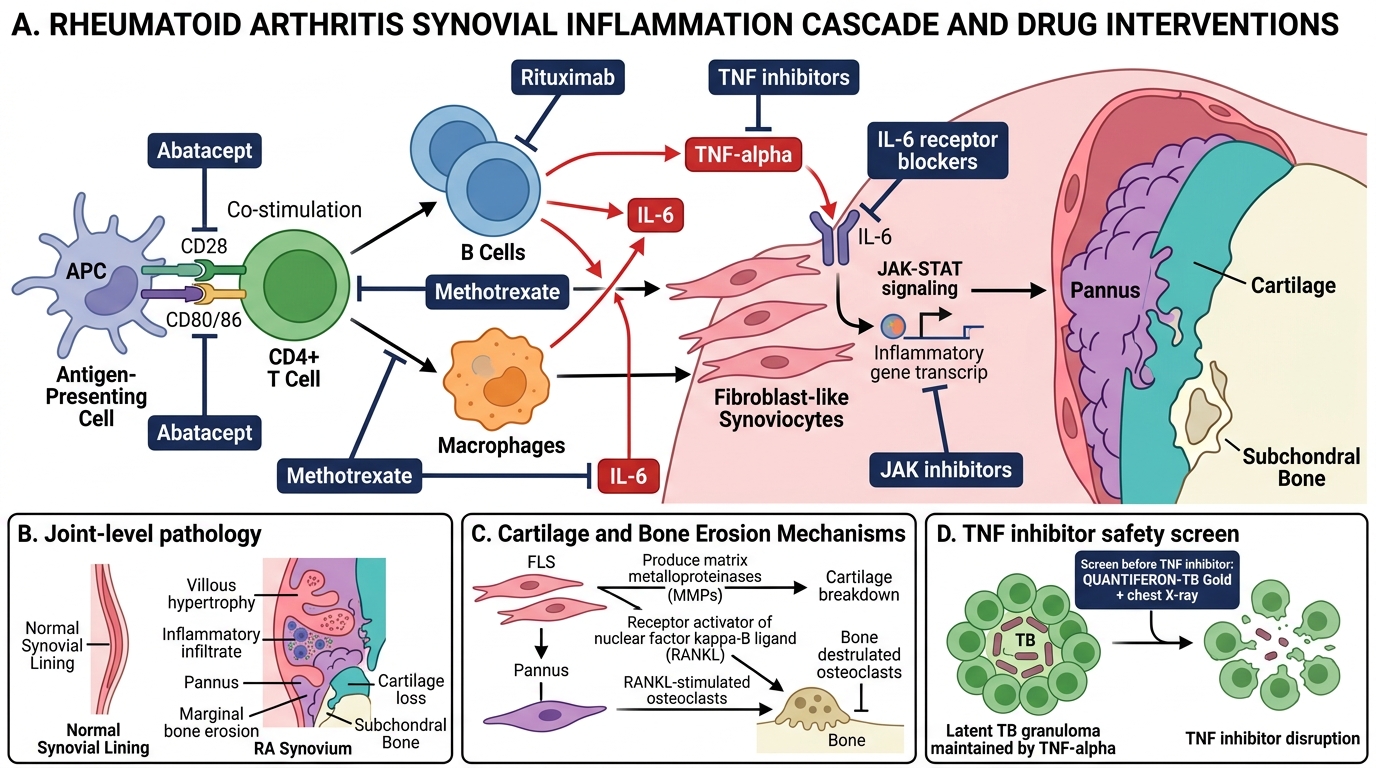
Rheumatoid Arthritis Pathophysiology and Drug Targets
SELF-CHECK
Which pre-treatment screen is MANDATORY before initiating a TNF inhibitor (e.g., adalimumab) for RA, and what is the rationale?
A. Hepatitis B and C serology, because biologics cause hepatotoxicity
B. QUANTIFERON-TB Gold and chest X-ray, because TNF-α is required to maintain latent TB granulomas and TNF inhibitors reactivate latent TB
C. Echocardiogram, because TNF inhibitors worsen heart failure
D. Renal function test, because biologics are renally cleared
Reveal Answer
Answer: B. QUANTIFERON-TB Gold and chest X-ray, because TNF-α is required to maintain latent TB granulomas and TNF inhibitors reactivate latent TB
TNF-α is critical for granuloma formation and maintenance — the immune structure that contains latent Mycobacterium tuberculosis. TNF inhibitors break down granuloma integrity, reactivating latent TB and dramatically increasing the risk of active TB (including disseminated and extrapulmonary TB). In India, with the world's highest TB burden, this is a non-negotiable screen. QUANTIFERON-TB Gold (preferred over Mantoux which has poor specificity post-BCG vaccination) combined with a chest X-ray must be performed before all biologics. Latent TB must be treated with isoniazid preventive therapy (IPT) as per NTEP guidelines before or concurrently with biologic initiation. Hepatitis B serology is also checked (biologics can reactivate hepatitis B), but the TB screen is the single most critical mandatory pre-biologic check in India.
Treatment Plans for Specific Rheumatologic Conditions: Prescribing and Monitoring
Developing a treatment plan for a rheumatologic condition requires integrating diagnosis, disease activity, prognostic factors, patient comorbidities, and patient preferences into a coherent and safe prescription strategy. The following disease-specific treatment frameworks are based on EULAR guidelines, API recommendations, and Indian National League Against Rheumatism (ILAR) practice principles. Each plan must begin with a measurable treatment target — in RA, this is the DAS28 score (remission <2.6 or low disease activity ≤3.2); in gout, a serum uric acid target of <6 mg/dL; in SLE, suppression of anti-dsDNA titres, complement normalisation, and organ-specific outcome markers. Treatment is not static — it is reviewed at defined intervals (3–6 months in RA, monthly initially in lupus nephritis, every 3–6 months in stable gout), escalated if the target is not met, and tapered if the target is sustained. The prescribing of rheumatologic medications is complicated by their significant side-effect profiles and the need for mandatory safety screens before initiating biologic and immunosuppressive agents. These requirements are detailed below for each disease category.
Rheumatoid Arthritis (RA) — treat-to-target strategy:
The ACR and EULAR 'treat-to-target' (T2T) recommendation defines the therapeutic goal as remission (DAS28 <2.6) or low disease activity (DAS28 2.6–3.2) in patients for whom remission is not achievable. The treatment is stepped up if the target is not achieved within 3–6 months.
- Step 1: Methotrexate (7.5–25 mg/week orally or SC) + folic acid (5 mg once weekly, NOT on the same day as MTX) ± short-term bridging prednisolone (≤10 mg/day, tapered over 3 months). Hydroxychloroquine and sulfasalazine may be added in a triple DMARD regimen.
- Step 2 (inadequate response at 3–6 months): Add or switch to a biologic DMARD (TNF inhibitor as first-line biologic) or a JAK inhibitor (tofacitinib, baricitinib). Check TB screen before starting biologic.
- Step 3 (second biologic failure): Switch mechanism class (e.g., IL-6 inhibitor tocilizumab, or rituximab, or abatacept).
- Monitoring for methotrexate toxicity: CBC and liver function tests at baseline, then every 4–8 weeks initially, then every 3 months once on a stable dose. Methotrexate is contraindicated in pregnancy (teratogenic — causes fetal death and neural tube defects), severe renal impairment, active liver disease, and active alcohol use. Counsel women of childbearing age about contraception.
- Monitoring for biologic toxicity: Full blood count, liver function, infection screening (including TB reactivation — fever, cough, weight loss) at each clinic visit. Hold biologics during any active infection or surgical procedure.
Ankylosing Spondylitis (AS) — ASAS-EULAR 2022 recommendations:
- First-line: NSAIDs (naproxen, diclofenac, celecoxib) at full anti-inflammatory dose, taken continuously (not just as needed), are the cornerstone of axial spondyloarthropathy treatment. Unlike other rheumatologic conditions, NSAIDs may slow radiographic progression in AS by reducing the anular ossification process — they are disease-modifying in this context. Physiotherapy (targeted spinal exercises, postural training, hydrotherapy) is equally important and should be prescribed as a co-primary therapy.
- Second-line (NSAID failure or contraindication): Biologic DMARDs — TNF inhibitors (adalimumab, etanercept, certolizumab) are first-line biologics for axial disease; IL-17 inhibitors (secukinumab, ixekizumab) are equally effective and are preferred in patients with co-existing psoriasis or IBD (TNF inhibitors can worsen IBD). Conventional DMARDs (methotrexate, sulfasalazine) are NOT effective for axial disease — they have a role only in peripheral joint and skin/nail involvement.
- Physiotherapy: daily home exercise programme, swimming, and postural advice are core non-pharmacological treatment. Explain that unlike RA, where rest may relieve stiffness temporarily, bed rest worsens AS.
Systemic Lupus Erythematosus (SLE) — organ-based treatment:
SLE treatment is guided by which organs are involved and their severity.
- All SLE patients: Hydroxychloroquine (HCQ) 200–400 mg/day (weight-based dosing, maximum 5 mg/kg/day to avoid retinopathy). HCQ reduces flare frequency, reduces damage accrual, and improves survival — it is maintained indefinitely unless contraindicated. Annual ophthalmology review for retinopathy after the first 5 years.
- Mild-to-moderate SLE (arthritis, rash, serositis, without major organ involvement): HCQ + low-dose prednisolone (≤7.5 mg/day) ± NSAIDs for joint pain; azathioprine or mycophenolate mofetil as steroid-sparing agents.
- Lupus nephritis (active, class III/IV): Induction: high-dose methylprednisolone IV pulse (1 g × 3 days) followed by oral prednisolone (1 mg/kg/day tapering) + mycophenolate mofetil (MMF) 2–3 g/day (preferred in Indian patients) or cyclophosphamide (NIH protocol or Euro-Lupus low-dose protocol). Maintenance: MMF 1–2 g/day or azathioprine + low-dose prednisolone for at least 3 years.
- CNS lupus, severe haematological SLE, severe vasculitis: IV cyclophosphamide (pulse protocol) + high-dose glucocorticoids.
- Monitoring SLE: CBC, renal function, urine protein:creatinine ratio, anti-dsDNA titre, complement C3/C4 at every clinic visit. Monitor blood pressure. Ophthalmology review for HCQ retinopathy annually after the first 5 years of therapy.
Crystal Arthropathies — prescribing for gout and pseudogout (IM7.16):
- Acute gout: First-line options — colchicine 0.5 mg twice or three times daily (continue until attack resolves; contraindicated in severe renal or hepatic failure — interacts with CYP3A4 inhibitors) OR NSAIDs (naproxen 500 mg twice daily or indomethacin 50 mg three times daily; avoid in CKD, peptic ulcer, elderly with high cardiovascular risk) OR prednisolone 30–35 mg/day tapering over 5 days (preferred if NSAIDs and colchicine are both contraindicated — renal failure, elderly, on anticoagulants). Do NOT start allopurinol or urate-lowering therapy (ULT) during an acute attack — this can prolong or worsen the attack by mobilising urate crystals.
- Urate-lowering therapy (ULT) for chronic gout prevention: Indications for ULT include: ≥2 attacks per year, tophi, urate nephropathy, or renal calculi. Allopurinol (xanthine oxidase inhibitor, first-line) — start at 100 mg/day 2–4 weeks AFTER the acute attack has resolved, titrate up to achieve target serum uric acid <6 mg/dL (or <5 mg/dL in severe tophaceous gout). Use with prophylactic colchicine 0.5 mg twice daily for the first 3–6 months of ULT initiation to prevent mobilisation flares. Second-line: febuxostat (more potent XO inhibitor), probenecid (uricosuric, avoid in renal impairment).
- Pseudogout (CPPD): Acute attacks treated with the same agents as gout — colchicine, NSAIDs, or corticosteroids. No disease-specific ULT exists for CPPD; management is symptomatic.
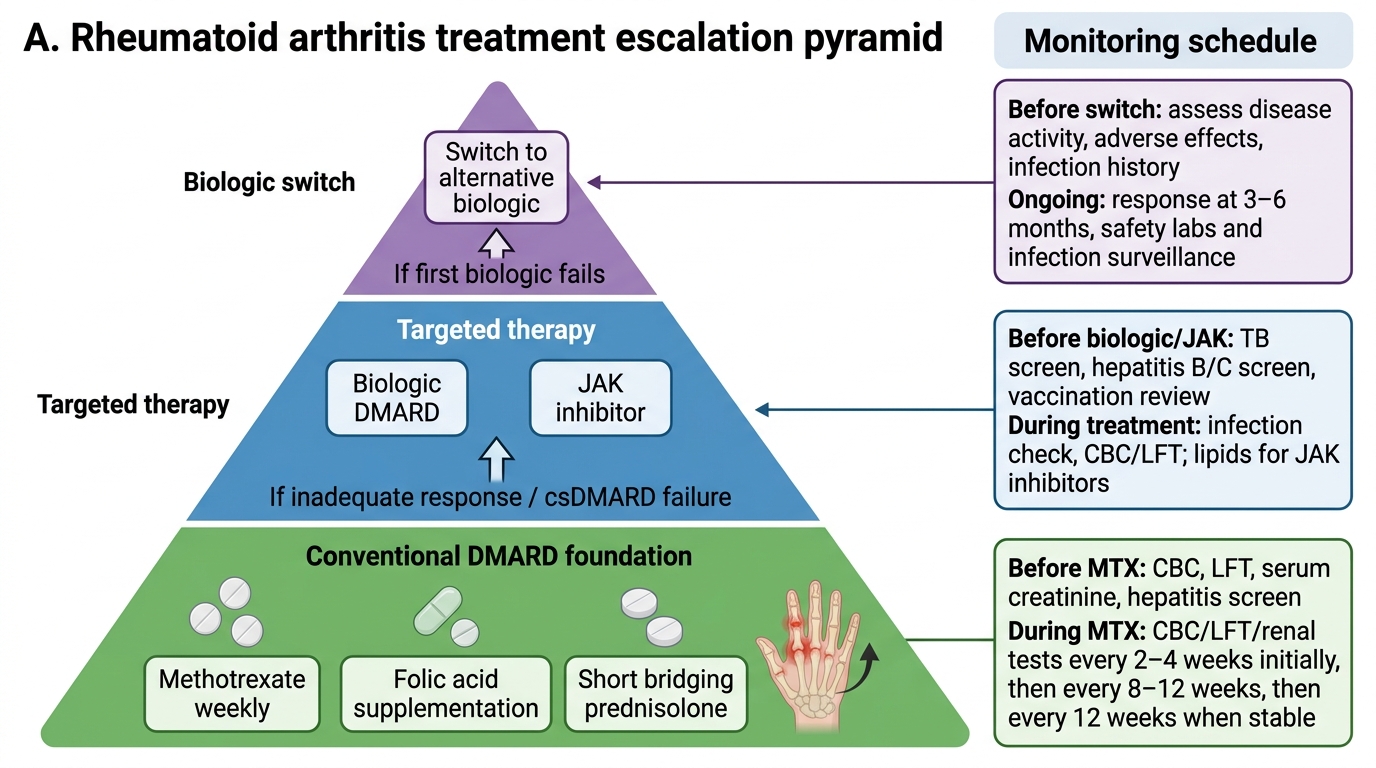
RA Treatment Escalation Pyramid
SELF-CHECK
A 52-year-old man has just experienced his third attack of gout in 12 months. He is currently in the intercritical (asymptomatic) period, 3 weeks after his last attack resolved. Serum uric acid is 9.1 mg/dL. He has no evidence of tophi. What is the MOST appropriate pharmacological intervention at this point?
A. Start allopurinol 300 mg/day immediately and continue without prophylactic cover
B. Start colchicine 0.5 mg twice daily for prophylaxis and defer allopurinol until the next acute attack
C. Start allopurinol at low dose (100 mg/day) with concurrent prophylactic colchicine 0.5 mg twice daily
D. Start NSAIDs as the primary long-term treatment for urate reduction
Reveal Answer
Answer: C. Start allopurinol at low dose (100 mg/day) with concurrent prophylactic colchicine 0.5 mg twice daily
This patient has met the indication for urate-lowering therapy (≥2 attacks per year). Allopurinol should be initiated 2–4 weeks after the acute attack has completely resolved (not during or immediately after the attack, as mobilisation of urate can trigger another attack). The starting dose of allopurinol is 100 mg/day, titrated upward by 100 mg every 2–4 weeks to achieve a target serum uric acid <6 mg/dL. Concurrent prophylactic colchicine (0.5 mg twice daily) is prescribed for the first 3–6 months of ULT initiation to suppress mobilisation flares as urate levels fall. Starting allopurinol without prophylactic colchicine at a full dose immediately risks triggering an acute attack. NSAIDs are for acute attack treatment — they do not reduce urate levels.