Page 16 of 23
IM7.21 | Rheumatologic Disease Quality of Life — SDL Guide
Learning Objectives
- Demonstrate understanding of the impact of rheumatologic conditions on quality of life, well-being, work, and family using the biopsychosocial and ICF framework (IM7.21)
- Administer and interpret validated patient-reported outcome measures (HAQ-DI, PHQ-9, FACIT-Fatigue, GAD-7) in a rheumatologic clinic encounter
- Identify and address the discordance between clinical disease activity and patient-experienced disability ('biological remission ≠ patient remission')
- Recognise the psychological comorbidities (depression, anxiety, pain catastrophising) that independently impair QoL in rheumatologic disease and refer appropriately
- Explain the impact of rheumatologic disease on employment, family roles, and sexual health and incorporate QoL findings into a holistic management plan
INSTRUCTIONS
Quality of life in rheumatologic disease is not an optional add-on but a core clinical outcome. This module develops your ability to assess, interpret, and act upon the impact of rheumatologic conditions on function, well-being, work, and family — using validated tools and a biopsychosocial framework that bridges biological disease control and patient-experienced health.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 353 — Patient Perspective and QoL in Rheumatic Disease (textbook)
- API Textbook of Medicine, 10th ed. — Patient-Centred Care in Rheumatology (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 26 — Impact of Musculoskeletal Disease (textbook)
- EULAR recommendations on QoL in rheumatic diseases — Gossec et al., Annals of Rheumatic Diseases 2014 (guideline)
- HAQ-DI: Fries et al., Arthritis & Rheumatism 1980 (validated in Indian populations) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya is a 29-year-old graphic designer who was diagnosed with rheumatoid arthritis 18 months ago. Her DAS28 score shows low disease activity on methotrexate — by clinical and laboratory measures, her RA is 'controlled.' Yet when she came to clinic last week, she was tearful. She has stopped working because she cannot use a mouse for more than an hour without severe hand pain. She is afraid to tell her fiancé about her diagnosis. She has not been to a movie or a restaurant in six months because she cannot open bottles, use cutlery confidently, or sit in one position for more than 20 minutes without stiffness. She describes waking at 3 am and lying in the dark, calculating how many years she has left before she will 'need to be cared for.' Her inflammation markers are normal. Her disease is not controlled — her life is being destroyed by it. In 2015, the EULAR standing committee on quality of life research established that 'clinical remission is not the same as patient remission' — a distinction that every rheumatologist must understand and every general practitioner must begin to practice.
WHY THIS MATTERS
NMC competency IM7.21 — 'Demonstrate an understanding of the impact of rheumatologic conditions on quality of life, well-being, work and family' — is rated SH, meaning students are expected to demonstrate this understanding in a supervised patient encounter, not merely recite it from a textbook. This competency matters because in rheumatology the gap between biological disease control and patient-perceived quality of life is wide, well-documented, and directly addressable. Patients who are not assessed for quality of life impacts will not be treated holistically; their adherence will decline, their psychosocial complications will accumulate, and their long-term outcomes will be worse than their disease activity scores would predict. In India, the quality of life burden is compounded by limited access to specialist care, financial constraints, joint family expectations about disability and work, and the stigma attached to 'arthritis' — a disease that patients and families frequently misattribute to old age, diet, or lack of willpower. Recognising and addressing these dimensions is a clinical skill.
RECALL
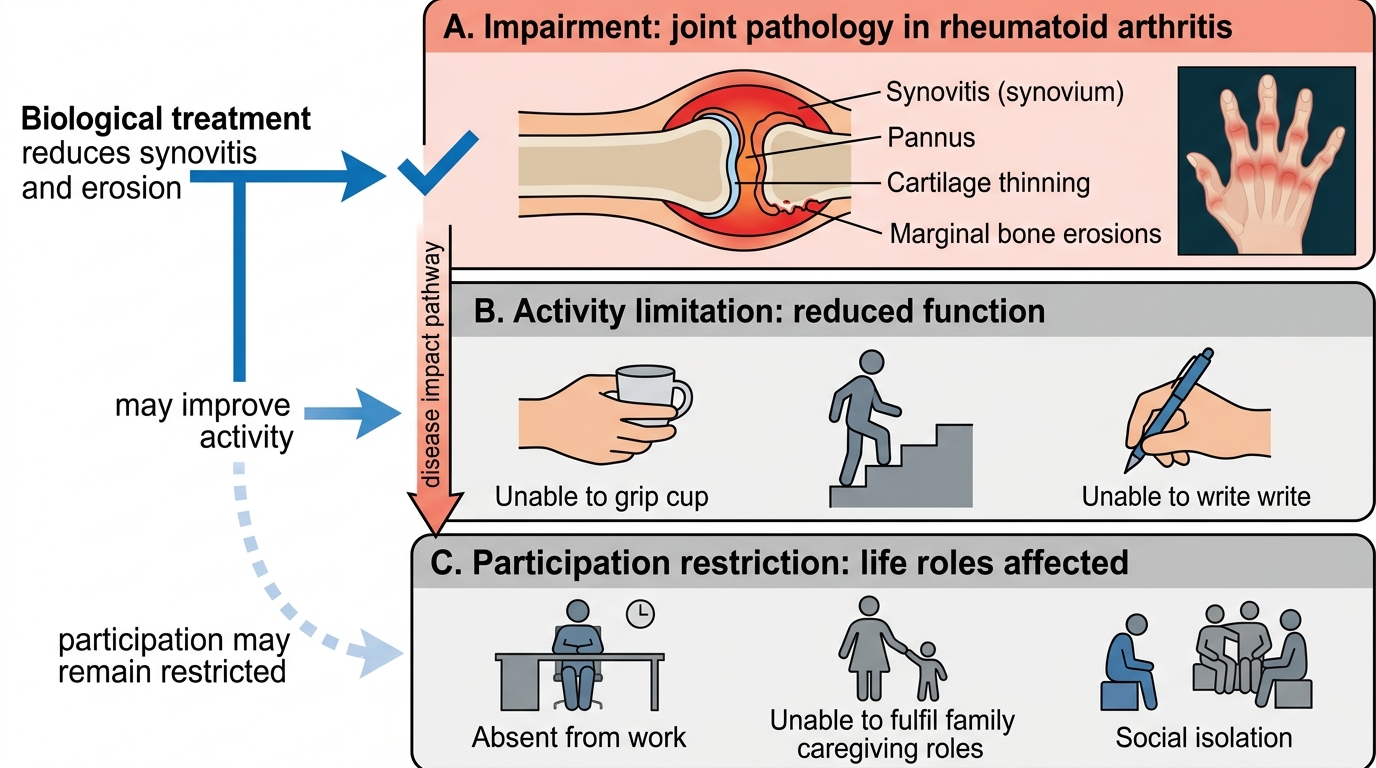
Before proceeding, recall the biopsychosocial model of illness, introduced in your community medicine and psychiatry modules. The World Health Organization's International Classification of Functioning, Disability and Health (ICF) framework distinguishes between three levels of health impact: impairment (the biological disease — joint inflammation, erosion), activity limitation (what the person cannot do — cannot grip, cannot climb stairs, cannot write), and participation restriction (what the person cannot participate in — employment, family roles, social activities, sexual relationships). Rheumatologic diseases produce impairment, activity limitation, and participation restriction simultaneously, and their relative severity may not be correlated — a patient with moderate inflammation may have severe participation restriction if their occupation demands fine motor skills, while a patient with more severe disease may have less restriction if their work is sedentary. Recall also from psychiatry that chronic pain and chronic inflammatory disease are independently associated with major depression (prevalence 2–3× general population) and anxiety disorder — these are not psychological reactions to be dismissed but comorbidities to be screened for and treated.
Clinical Indication and Relevance of Quality of Life Assessment in Rheumatologic Disease
Quality of life (QoL) assessment is clinically indicated in every patient with a chronic rheumatologic condition — not as an optional supplementary exercise but as an integral part of the standard clinical assessment alongside disease activity scores, joint counts, and laboratory markers. The indication arises from a fundamental limitation of traditional clinical outcomes: biological disease control (remission or low disease activity by DAS28, ESR, CRP) does not reliably predict patient-reported well-being, functional capacity, or participation in work and family life. This discordance is well-established across RA, SLE, ankylosing spondylitis, and psoriatic arthritis. In RA, studies consistently show that approximately 20–30% of patients in clinical remission by DAS28 criteria continue to report significant functional impairment on the Health Assessment Questionnaire (HAQ) and significant fatigue and psychological distress on patient-reported outcomes. Treating the DAS28 without addressing the HAQ is incomplete care.
The clinical relevance of QoL assessment operates at three distinct levels. First, at the individual patient level, identifying unmet QoL needs — fatigue, pain, functional loss, psychological comorbidity, work disability, sexual health — allows targeted referral and intervention beyond pharmacological management: physiotherapy, occupational therapy, psychological support, social work, disability benefits assessment. Second, at the therapeutic decision level, QoL measures inform whether a treatment that is biologically effective is also experientially effective — a patient may have well-controlled inflammatory markers but severe fatigue or depression, indicating the need for additional management strategies. Third, at the population and health systems level, patient-reported outcome measures (PROMs) from QoL assessments are increasingly used to benchmark healthcare quality, inform commissioning decisions, and evaluate the effectiveness of rheumatology services.
The World Health Organization defines health-related quality of life (HRQoL) as the subjective perception of health across physical functioning, role functioning (work, family, social), mental health, and vitality. This definition makes explicit that HRQoL is subjective — only the patient can report it — and multi-dimensional — no single symptom or test captures it. A complete HRQoL assessment therefore requires structured, validated patient-reported outcome measures (PROMs), not just the clinician's impression of the patient's functional state.
ICF Framework in Rheumatoid Arthritis
Biopsychosocial Principles Governing QoL Impact in Rheumatologic Disease
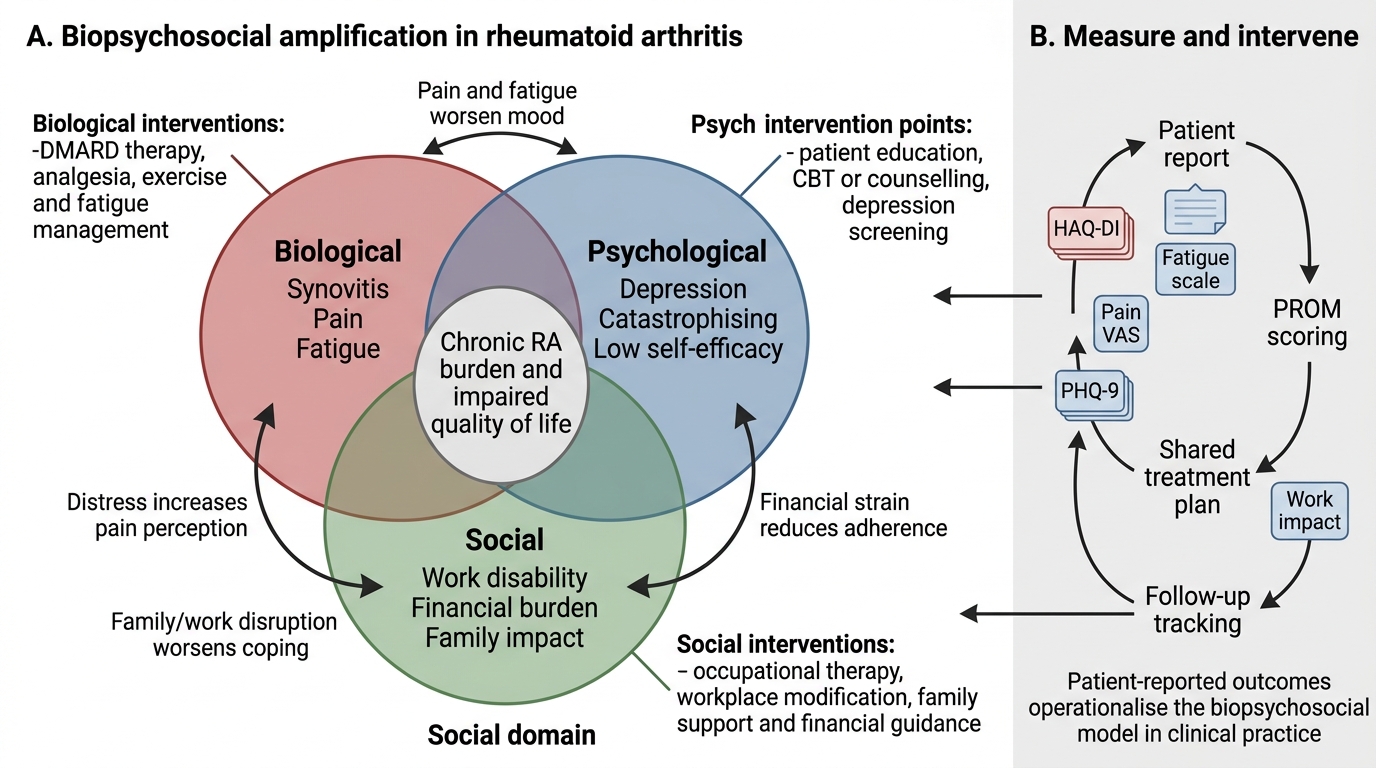
The biopsychosocial model provides the governing framework for understanding how rheumatologic disease affects quality of life. George Engel's original model (1977) proposed that illness is produced by the interplay of biological (disease, inflammation, joint damage), psychological (pain cognitions, coping style, mood, self-efficacy), and social (occupation, family support, financial resources, cultural context) factors. In rheumatology, these three domains interact bidirectionally: biological disease activity causes pain and functional loss; pain and functional loss generate psychological distress (depression, anxiety, reduced self-efficacy); psychological distress amplifies pain perception and reduces engagement with treatment; reduced family and workplace support increases social isolation, which worsens depression. This cycle is not inevitable — it can be interrupted at any level — but it cannot be interrupted by pharmacological management alone.
Biological determinants of QoL in rheumatologic disease: Joint inflammation, structural damage (erosions, joint space narrowing), and extra-articular involvement produce the primary physiological impairments: pain, stiffness, fatigue, and functional loss. Pain in inflammatory arthritis has two components: nociceptive pain from active synovitis (responsive to DMARDs and anti-inflammatory drugs) and central sensitisation — a state in which the central nervous system becomes hypersensitised to pain signals, producing pain that persists even after inflammation is controlled. This component of pain requires different management (graded exercise, cognitive-behavioural approaches, amitriptyline at low dose for central sensitisation) and is a key reason why patients in 'remission' by DAS28 may still report significant pain. Fatigue in RA and SLE is one of the most distressing and disabling symptoms — driven by cytokine-mediated effects on the brain, anaemia, sleep disturbance, depression, and deconditioning — and correlates poorly with joint counts. An HAQ or PROMIS Fatigue score should be obtained at every visit.
Psychological determinants of QoL: Depression is present in approximately 15–38% of RA patients and 25–47% of SLE patients — far higher than in age-matched controls and in many other chronic diseases. The relationship is bidirectional: disease causes depression, and depression amplifies pain, reduces adherence, and worsens disease outcomes. Pain catastrophising (the tendency to perceive pain as overwhelming and to focus on it helplessly) is the strongest psychological predictor of disability in rheumatoid arthritis — stronger than joint count or radiographic damage. Self-efficacy — the patient's belief in their capacity to manage their condition — is a modifiable psychological factor that predicts medication adherence, exercise engagement, and long-term function. Patients with high self-efficacy can maintain better function at equivalent disease severity compared with low-self-efficacy patients.
Social determinants of QoL: Employment status is one of the most powerful determinants of QoL in rheumatologic disease. Work disability — inability to maintain paid employment — occurs in 30–50% of RA patients within 10 years of diagnosis and 40–60% in those with untreated or undertreated disease. Work disability causes income loss, social role loss, loss of daily structure, and reduced self-worth — all of which compound psychological comorbidity. Family impact is particularly salient in India, where women with RA or SLE may face pressure to perform domestic roles (cooking, childcare) that they can no longer manage, with attendant family tension. Financial burden — cost of DMARDs, biologics, physiotherapy, and monitoring blood tests — is a major determinant of adherence and QoL in resource-constrained settings. Sexual health — disrupted by pain, joint limitation, fatigue, and psychological distress — is rarely discussed in standard clinic encounters but is highly relevant to younger patients with RA, SLE, and spondyloarthropathies.
Biopsychosocial Model of Rheumatoid Arthritis
Patient-Reported Outcome Measures: Technique and Administration
Patient-reported outcome measures (PROMs) are standardised, validated questionnaires completed by the patient (not the clinician) to quantify health-related quality of life, functional status, pain, fatigue, and psychological well-being. Their use in clinical practice is the operationalisation of the biopsychosocial model — transforming subjective patient experience into reproducible, trackable numbers that can guide clinical decision-making. The IM7.21 competency, when assessed at the SH level, requires students to demonstrate familiarity with the most important PROMs used in rheumatologic practice, understand their structure and scoring, and be able to administer them appropriately in a supervised clinical encounter.
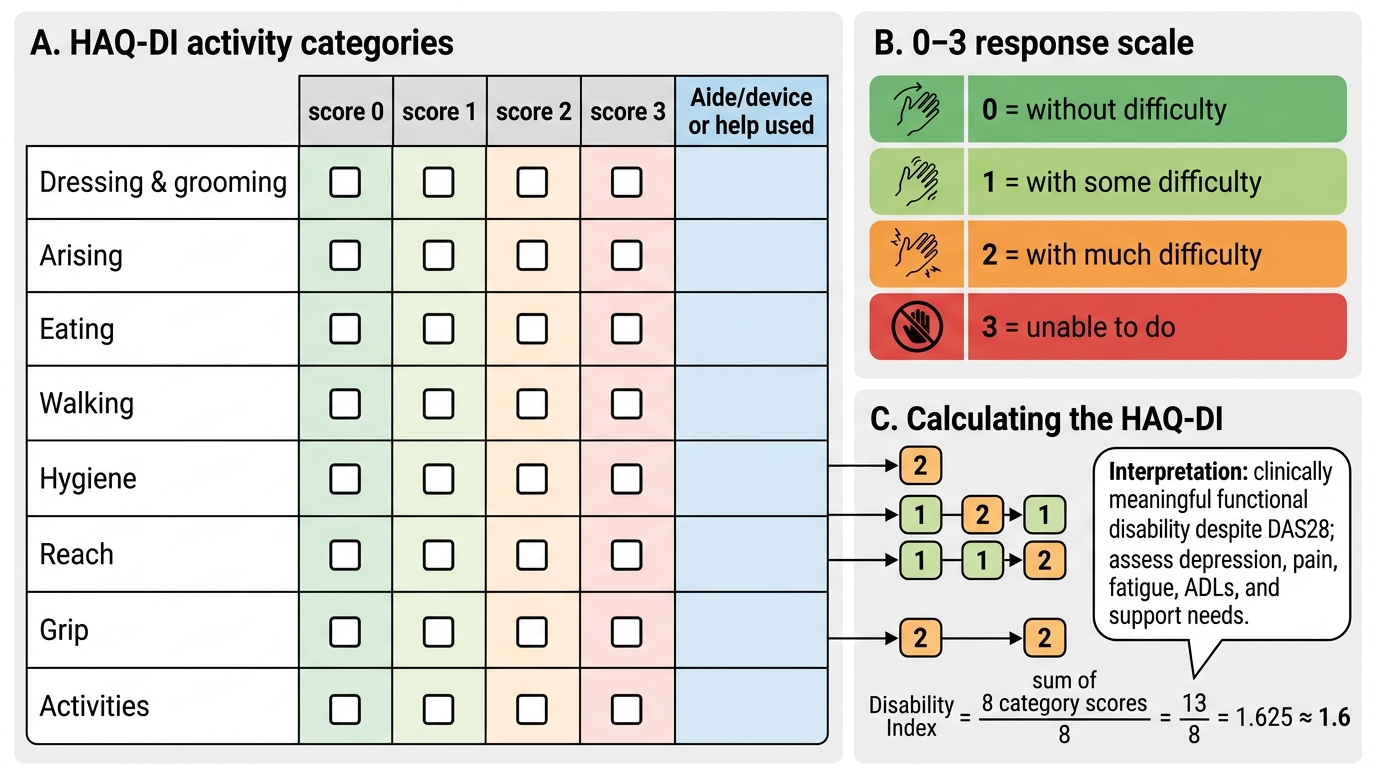
Health Assessment Questionnaire — Disability Index (HAQ-DI): The HAQ-DI is the most widely used and validated PROM for rheumatoid arthritis globally, including in Indian clinical practice. It assesses functional disability across eight categories of daily activities: dressing and grooming, arising, eating, walking, hygiene, reach, grip, and usual activities. Each category is scored 0–3 (0 = no difficulty, 1 = some difficulty, 2 = much difficulty, 3 = unable to do). The overall HAQ-DI score is the mean of the eight category scores, ranging from 0 (no disability) to 3 (complete disability). An HAQ score of ≥1.0 indicates significant functional disability correlating with work incapacity; changes of ≥0.22 are considered clinically meaningful. The HAQ-DI is sensitive to treatment effects — successful DMARD therapy produces measurable HAQ improvement within 3–6 months. Administration: hand the HAQ form to the patient in the waiting area before the clinic visit; it takes 5–8 minutes to complete; score and review with the patient during the consultation.
Disease-specific and generic HRQoL PROMs used in rheumatology:
- Short Form-36 (SF-36): A generic HRQoL measure assessing 8 domains (physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, mental health); produces two summary scores (Physical Component Summary [PCS] and Mental Component Summary [MCS]); useful for comparing QoL across disease types and with healthy population norms
- PROMIS (Patient-Reported Outcomes Measurement Information System): A US NIH-developed adaptive item bank covering pain interference, fatigue, physical function, anxiety, depression, social participation; computer-adaptive testing reduces respondent burden; increasingly used in rheumatology clinical trials and major rheumatology centres
- Fatigue assessment: FACIT-Fatigue scale (13 items, 0–52, lower scores = more fatigue; scores ≤30 indicate clinically significant fatigue); Bristol Rheumatoid Arthritis Fatigue scales (BRAF); fatigue is consistently reported as one of the most impactful symptoms in RA and SLE
- Depression and anxiety screening: PHQ-9 (Patient Health Questionnaire, 9 items, score 0–27; ≥10 = moderate depression warranting intervention; ≥20 = severe depression) and GAD-7 (Generalised Anxiety Disorder, 7 items; ≥10 = moderate anxiety) are brief, validated, and widely used in primary and specialist care. In any patient with chronic rheumatologic disease and unexplained pain disproportionate to disease activity, the PHQ-9 should be administered. A PHQ-9 ≥10 warrants referral to or management by a psychiatry or psychology service.
- Work productivity: WPAI-RA (Work Productivity and Activity Impairment questionnaire); assesses absenteeism, presenteeism (working but impaired), and overall work impairment; relevant for younger working-age patients
Communication technique for PROM administration: Introduce the questionnaire to the patient with an explanation of its purpose: 'These questions will help me understand how your arthritis is affecting your daily life and how you are feeling — not just your blood results. Your answers will help me adjust your treatment plan.' Emphasise that there are no right or wrong answers and that it should reflect their experience over the past week (or as specified by the PROM). After scoring, discuss the results with the patient: 'Your HAQ score has improved from 1.8 to 1.2 since starting methotrexate — that's meaningful progress. Your PHQ-9 score suggests you may be feeling quite low — let's talk about that today.'
HAQ-DI Questionnaire Format and Scoring
SELF-CHECK
A 38-year-old woman with RA has a DAS28 of 2.4 (remission) on methotrexate but completes an HAQ-DI during her clinic visit scoring 1.6 and a PHQ-9 scoring 16 (moderate depression). How should the clinician interpret these findings?
A. The DAS28 remission means the disease is well controlled — the HAQ and PHQ-9 do not require action
B. The HAQ and PHQ-9 findings indicate that biological remission does not equate to patient remission — functional disability and depression require targeted management
C. The PHQ-9 score is likely a spurious result caused by the joint pain and will improve automatically as the RA improves
D. An HAQ of 1.6 in remission is expected and does not require further assessment
Reveal Answer
Answer: B. The HAQ and PHQ-9 findings indicate that biological remission does not equate to patient remission — functional disability and depression require targeted management
This scenario illustrates the well-documented gap between clinical disease activity (DAS28 remission) and patient-experienced quality of life. An HAQ-DI of 1.6 indicates significant functional disability (the threshold for clinically meaningful disability is ≥1.0) that is not captured by the DAS28. PHQ-9 ≥10 indicates moderate depression, which in rheumatoid arthritis is not merely a psychological reaction to pain — it is a comorbidity that independently reduces medication adherence, amplifies pain perception, and worsens long-term functional outcomes. Both findings require active management: functional disability warrants referral to occupational therapy and physiotherapy; depression should be assessed further and managed (cognitive-behavioural therapy is first-line in the context of chronic pain; antidepressants if moderate-severe). Clinical remission is not patient remission.