Page 1 of 15
IM8.1-7 | Hypertension Foundations — SDL Guide
Learning Objectives
- Define and classify hypertension using the ACC/AHA 2017 staging system and compare it with JNC staging
- Describe the epidemiology and genetic basis of primary (essential) hypertension in the Indian context
- Explain the pathophysiology of primary hypertension including RAAS, SNS, renal, and vascular mechanisms
- Differentiate primary from secondary hypertension and describe clinical clues and aetiologies of secondary causes
- Define hypertensive urgency and emergency, and identify target organ damage
INSTRUCTIONS
Hypertension is the single most important modifiable risk factor for cardiovascular, cerebrovascular, and renal disease worldwide, and India bears a disproportionate part of this burden. This module builds a strong mechanistic and clinical foundation — definition, staging, pathophysiology, primary versus secondary causes, target organ damage, and the critical distinction between hypertensive urgency and emergency. Precision in thresholds and staging is non-negotiable in clinical practice and in examinations.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 271 — Systemic Hypertension (textbook)
- API Textbook of Medicine, 10th ed., Ch. 12 — Hypertension (textbook)
- Davidson's Principles & Practice of Medicine, 24th ed., Ch. 19 — Hypertension (textbook)
- ACC/AHA 2017 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (guideline)
- Indian Guidelines on Hypertension (IGH-IV) 2019, Journal of Human Hypertension (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Ramesh, a 52-year-old schoolteacher from Puducherry, visits the outpatient department for a pre-operative fitness check before elective knee replacement. He has no symptoms. His blood pressure is recorded at 164/98 mmHg on his right arm, and a repeat reading 10 minutes later gives 162/96 mmHg. He says he has never been told he has high blood pressure and feels 'perfectly fine'. His ECG shows left ventricular hypertrophy with strain pattern. His urine dipstick reveals 2+ protein. A fundoscopic examination shows arteriovenous nicking and a focal arteriolar narrowing. Ramesh is hypertensive — almost certainly for years — and his heart, kidneys, and retinal vessels are already paying the price. He is not an outlier: India has approximately 220 million hypertensive adults, fewer than 15% of whom have their blood pressure under control. The silent nature of hypertension, the multiplicity of its mechanisms, the clues that distinguish primary from secondary disease, and the signs that tell you organs are already damaged — these are the foundations this module builds.
WHY THIS MATTERS
Hypertension is the leading attributable risk factor for premature death globally, responsible for approximately 10.4 million deaths per year. For the final-year MBBS student in India, its relevance is inescapable: it underlies roughly 57% of all strokes, 24% of all coronary artery disease, and is the commonest cause of end-stage renal disease referred to tertiary care. The NMC competencies IM8.1–IM8.7 require knowledge and understanding at the KH (applied clinical knowledge) level — meaning you must not only memorise definitions and numbers but use them to identify and stage hypertension in a patient, recognise which features suggest a secondary cause, and identify target organ damage from history, examination, and basic investigations. Every clinical posting — medicine, surgery, obstetrics, paediatrics, ophthalmology — will place a hypertensive patient in front of you.
RECALL
Before proceeding, activate what you already know. Blood pressure (BP) is the product of cardiac output (CO) and systemic vascular resistance (SVR): BP = CO × SVR. Cardiac output is the product of heart rate and stroke volume; systemic vascular resistance depends on arteriolar tone, blood viscosity, and vessel radius (Poiseuille's law: resistance ∝ 1/radius⁴). The renin-angiotensin-aldosterone system (RAAS) — renin from the juxtaglomerular apparatus → angiotensin I → angiotensin II via ACE → aldosterone — raises BP by increasing SVR (angiotensin II vasoconstriction) and increasing blood volume (aldosterone-mediated sodium and water retention). The sympathetic nervous system (SNS) raises heart rate, cardiac contractility, and arteriolar tone via catecholamines. Baroreceptors in the carotid sinus and aortic arch detect wall stretch and modulate SNS output to maintain BP homeostasis. Recall the major vascular beds and which ones contribute to end-organ damage in sustained hypertension: brain, heart, kidneys, retina, and large vessels.
Definition and Classification of Hypertension
Hypertension is defined as a sustained elevation of arterial blood pressure above a threshold value that is associated with increased cardiovascular, cerebrovascular, and renal end-organ risk. The definition is deceptively simple, but the precise threshold has been the subject of decades of clinical debate, large randomised trials, and evolving guideline recommendations — and two major classification systems remain in active use. Students and clinicians must know both systems and must always state which they are citing when classifying a patient's blood pressure, because the threshold determines whether a patient is labelled hypertensive, whether pharmacological treatment is indicated, and which risk category they occupy. The physiological basis for defining any threshold is the log-linear relationship between blood pressure level and cardiovascular event risk: risk begins rising at pressures as low as 115/75 mmHg and doubles with every 20/10 mmHg increment above that — there is no discrete 'safe floor'. The clinical thresholds represent pragmatic cut-offs where the benefit of treatment outweighs its costs and harms.
ACC/AHA 2017 Classification (Whelton et al., JACC 2018; the most current guideline cited in Harrison's and used internationally):
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | <120 | AND <80 |
| Elevated | 120–129 | AND <80 |
| Stage 1 Hypertension | 130–139 | OR 80–89 |
| Stage 2 Hypertension | ≥140 | OR ≥90 |
| Hypertensive Crisis | >180 | AND/OR >120 |
The ACC/AHA 2017 guideline lowered the hypertension threshold from 140/90 to 130/80 mmHg. This was driven by evidence that cardiovascular risk increases log-linearly above 115/75 mmHg, and that outcomes improve with earlier treatment in high-risk individuals.
JNC 7 Classification (the older system, still referenced in Indian guidelines and many hospital protocols):
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | <120 | AND <80 |
| Pre-hypertension | 120–139 | OR 80–89 |
| Stage 1 HTN | 140–159 | OR 90–99 |
| Stage 2 HTN | ≥160 | OR ≥100 |
Under JNC 7, hypertension begins at 140/90 mmHg. The Indian Guidelines on Hypertension (IGH-IV, 2019) continue to use the JNC 7 threshold of 140/90 as the treatment initiation threshold for most patients, while acknowledging the ACC/AHA 2017 evidence.
For examination purposes: always state which classification system you are citing. If a question says 'classify this patient's BP of 134/86', the answer is Stage 1 under ACC/AHA 2017, but pre-hypertension (not hypertension) under JNC 7 — these are different clinical implications. Isolated systolic hypertension (ISH) is defined as systolic BP ≥140 with diastolic BP <90 and is common in the elderly due to aortic stiffening.
Blood pressure measurement must follow standardised technique to be valid: patient seated and rested for ≥5 minutes, back supported, feet flat, arm supported at heart level, no caffeine/exercise/smoking for 30 minutes, appropriate cuff size (bladder encircles >80% of arm circumference). At least 2 readings on 2 or more separate occasions are needed to diagnose hypertension, except in hypertensive emergencies.
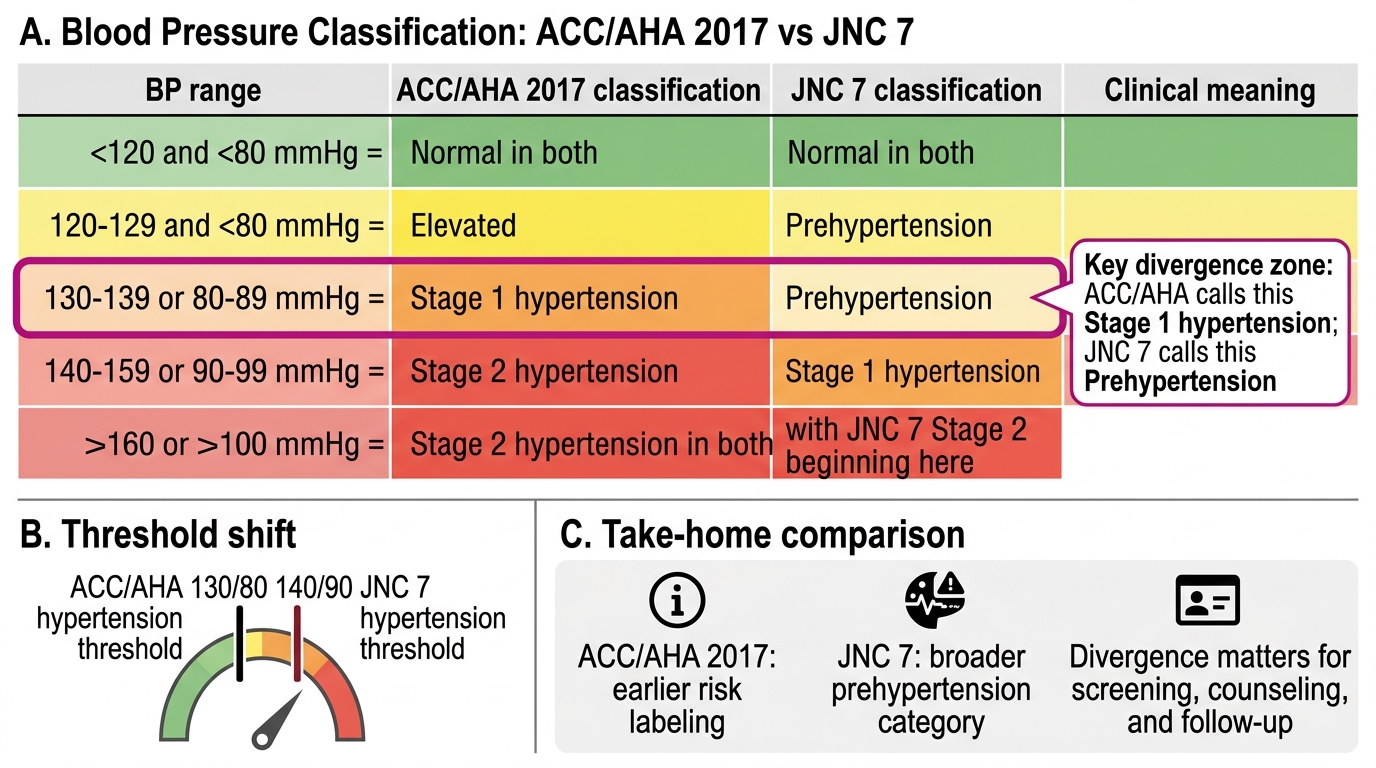
ACC/AHA 2017 vs JNC 7 Blood Pressure Classification
Epidemiology, Genetics, and Prevalence of Hypertension
Epidemiology describes who gets hypertension, how commonly, and why. Understanding the magnitude and distribution of the burden is the first step in competency IM8.1 — describing and discussing epidemiology and prevalence.
Globally, an estimated 1.28 billion adults aged 30–79 years have hypertension (WHO 2021), making it the most prevalent non-communicable disease. Only approximately 42% of those with hypertension are diagnosed, and a mere 21% have their BP under control. The age-standardised prevalence has risen sharply in low- and middle-income countries while declining modestly in high-income countries, reflecting the epidemiological transition — urbanisation, dietary sodium excess, sedentary lifestyles, and obesity are driving the rise in the developing world.
In India, the most recent National Family Health Survey (NFHS-5, 2019–21) data show that hypertension (BP ≥140/90 mmHg) affects approximately 28.4% of men and 27.9% of women aged 15 and above — translating to roughly 220 million hypertensive Indians. A striking feature of the Indian pattern is the low treatment and control rate: only about 45% of hypertensive individuals are aware of their diagnosis, 36% are on treatment, and barely 15% achieve BP control. Urban Indians have higher prevalence than rural populations, though the rural-urban gap is narrowing rapidly with economic development. South Indian states (Tamil Nadu, Kerala, Andhra Pradesh) show higher prevalence than northern states, reflecting dietary patterns (high salt intake in coastal diets) and genetic determinants. NHANES data (USA) show prevalence of approximately 45% in adults, with higher rates in Black Americans — a well-studied disparity linked to RAAS responsiveness, salt sensitivity, and socioeconomic determinants.
Risk factors for hypertension can be divided into non-modifiable (age — prevalence rises from <10% at age 30 to >65% at age 70; male sex until menopause when women catch up; ethnicity; family history) and modifiable (obesity — especially central adiposity; dietary sodium excess; physical inactivity; alcohol excess; psychological stress; sleep-disordered breathing). The classic J-curve relating diastolic pressure to cardiovascular events (suggestion that very low diastolic BP in treated patients increases coronary risk) is most relevant in patients with known coronary artery disease and is not a threshold-lowering argument.
Genetics of primary hypertension is complex — it is a polygenic quantitative trait with heritability estimated at 30–50%. Large genome-wide association studies (GWAS) have identified hundreds of common variants with small individual effects, involving pathways regulating sodium transport (epithelial sodium channel, sodium-hydrogen exchanger), RAAS components (AGT, ACE, AT1R genes), aldosterone synthesis (CYP11B2), endothelin, nitric oxide synthesis, and the sympathetic nervous system. No single gene accounts for more than 1–2 mmHg of BP variance. Rare monogenic forms of hypertension (Mendelian hypertension syndromes) exist and are important diagnostic considerations in young patients with severe or resistant hypertension: Liddle syndrome (gain-of-function ENaC mutation → salt retention → low renin, low aldosterone), Gordon syndrome (pseudohypoaldosteronism type II), glucocorticoid-remediable aldosteronism (GRA), and congenital adrenal hyperplasia are canonical examples.
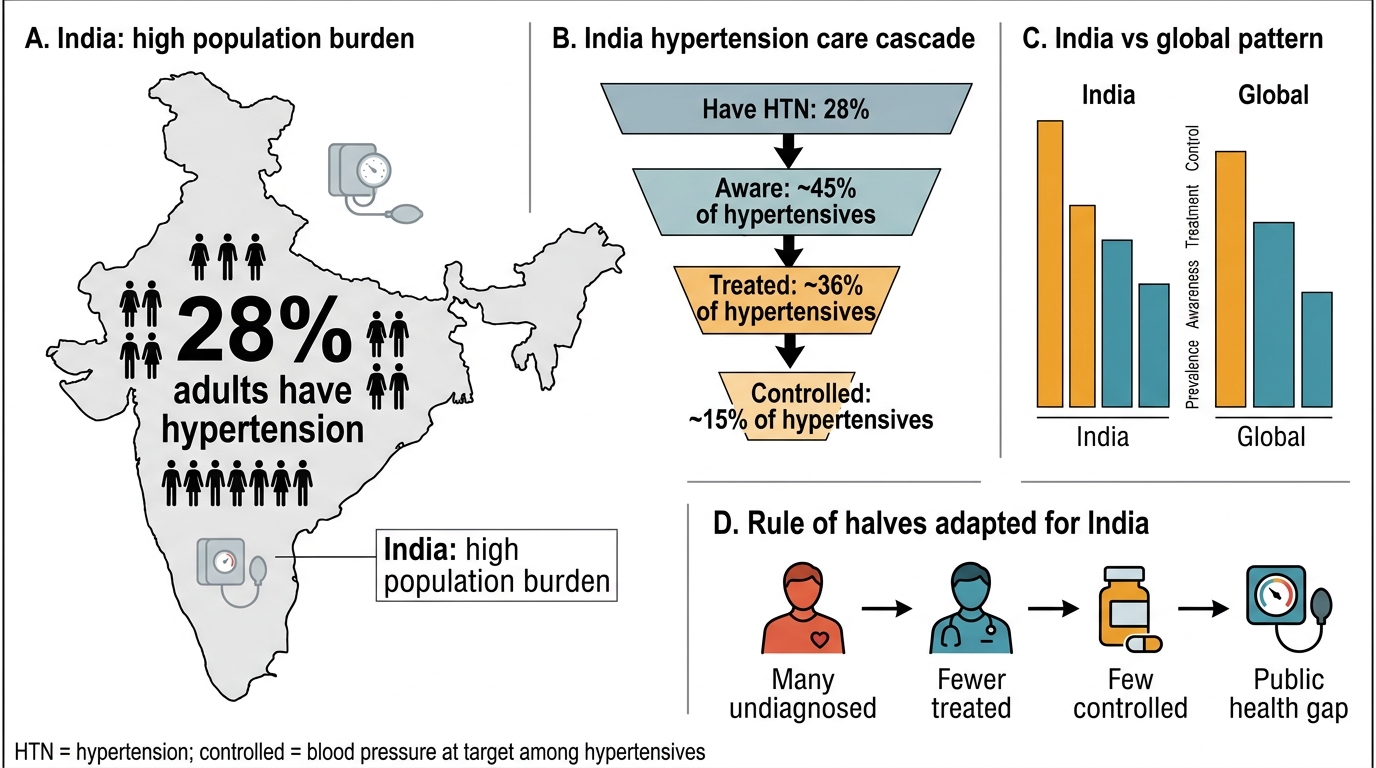
India's Hypertension Burden and Care Cascade
Pathophysiology of Hypertension
Primary (essential) hypertension — which accounts for 90–95% of all hypertension — does not have a single identifiable cause; its pathophysiology is the convergence of multiple interacting mechanisms that together shift the BP set-point upward. Understanding these mechanisms is the foundation for rationalising antihypertensive drug classes. The key mechanisms are RAAS activation, sympathetic nervous system overactivity, renal salt handling abnormalities, vascular endothelial dysfunction, and chronic low-grade inflammation. In any given patient, one or more of these pathways may predominate.
1. Renin-Angiotensin-Aldosterone System (RAAS) activation: In many hypertensive patients — particularly those with high-renin hypertension — increased renin secretion from the juxtaglomerular cells drives excess angiotensin II generation. Angiotensin II acts on AT1 receptors to cause: (a) direct vasoconstriction raising SVR; (b) stimulation of the adrenal cortex to release aldosterone, which promotes distal nephron sodium and water reabsorption, expanding extracellular volume; (c) central and peripheral sympathetic activation; (d) cardiac and vascular hypertrophy; and (e) renal afferent arteriolar constriction, reducing GFR and triggering further sodium retention. Angiotensin II also stimulates reactive oxygen species (ROS) generation and promotes endothelial inflammation. This mechanism is the target of ACE inhibitors (block angiotensin I → II conversion), angiotensin receptor blockers (ARBs) (block AT1 receptors), and renin inhibitors (aliskiren).
2. Sympathetic nervous system (SNS) overactivity: Elevated sympathetic tone — demonstrated by microneurography and plasma catecholamine studies — is a consistent finding in early hypertension, especially in young, lean, high-renin patients. SNS overactivity raises heart rate, cardiac contractility (increasing CO), and peripheral vascular tone (increasing SVR). It also stimulates renin release from the kidney. Chronic SNS activation contributes to the development of insulin resistance and metabolic syndrome. Beta-blockers reduce heart rate and renin release; alpha-1 blockers reduce SVR; central sympatholytics (clonidine, methyldopa) reduce central SNS outflow.
3. Renal sodium handling: Guyton's seminal hypertension model emphasised that sustained hypertension requires a renal pressure-natriuresis defect — the kidney's ability to excrete sodium is impaired at normal BP, so a higher BP 'pressure natriuresis' is needed to achieve sodium balance. This may result from intrinsic nephron loss (reduced GFR), increased tubular sodium reabsorption (aldosterone, angiotensin II, sympathetic stimulation of tubules), or primary genetic variants in sodium transporters. Salt sensitivity — an exaggerated BP response to sodium loading — is more common in older patients, Black individuals, and those with CKD or diabetes. Thiazide diuretics and loop diuretics lower BP by increasing renal sodium excretion.
4. Endothelial dysfunction: Vascular endothelium produces nitric oxide (NO) (from eNOS acting on L-arginine), a potent vasodilator that maintains vascular tone and inhibits platelet aggregation and smooth muscle proliferation. In hypertension, reduced NO bioavailability — due to ROS-mediated quenching, reduced eNOS activity (often secondary to angiotensin II and aldosterone), or L-arginine deficiency — shifts vascular tone toward vasoconstriction. Endothelin-1 (a vasoconstrictor) is upregulated. The net effect is a higher resting SVR and reduced vasodilatory reserve. Calcium channel blockers (CCBs) lower SVR by blocking voltage-gated L-type calcium channels in vascular smooth muscle.
5. Structural vascular changes (vascular remodelling): Sustained elevated BP causes concentric hypertrophy and inward remodelling of resistance arteriole walls (increased media:lumen ratio). This vascular remodelling is initially adaptive but ultimately pathological — the thickened, stiffer arteriolar wall reduces the maximal vasodilatory capacity, perpetuating and amplifying the BP elevation. Aortic stiffness (measured by pulse wave velocity) increases with age and with hypertensive vascular damage, explaining the preferential rise in systolic (and widening of pulse pressure) in older hypertensive patients.
6. Adipose-tissue and metabolic contributions: Central obesity contributes to hypertension through multiple channels: adipokines (leptin stimulates SNS; adiponectin is reduced), free fatty acid-mediated insulin resistance (which impairs vasodilatory insulin signalling), RAAS activation by adipose RAAS components, sleep apnoea (hypoxia triggers SNS), and physical inactivity. The metabolic syndrome (central obesity + hypertension + dyslipidaemia + hyperglycaemia) amplifies cardiovascular risk beyond the additive contributions of its components.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
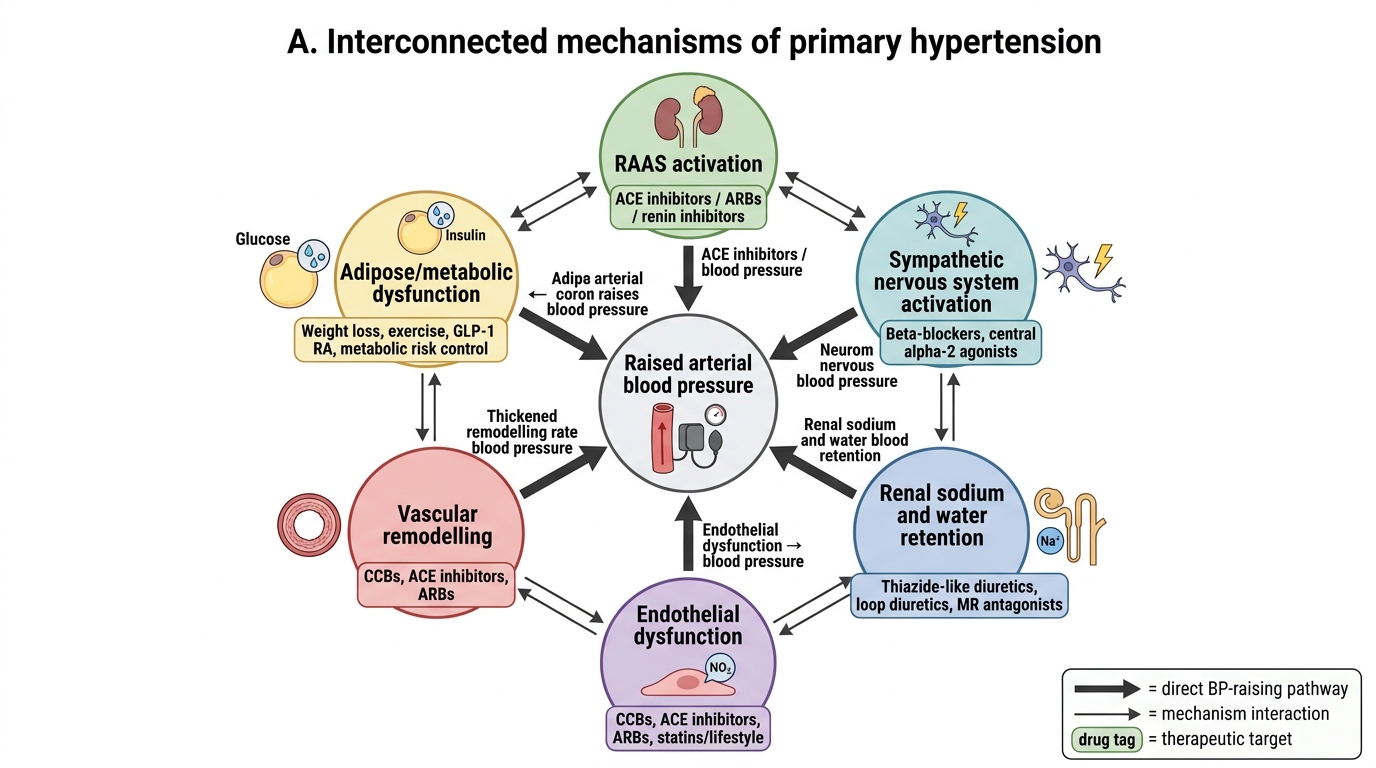
Primary Hypertension: Interconnected Mechanisms and Drug Targets
SELF-CHECK
A 45-year-old man has blood pressure consistently 134/86 mmHg on three separate visits. According to the ACC/AHA 2017 classification, which stage does this represent?
A. Normal blood pressure
B. Elevated blood pressure
C. Stage 1 hypertension
D. Stage 2 hypertension
Reveal Answer
Answer: C. Stage 1 hypertension
Under ACC/AHA 2017, Stage 1 hypertension is defined as systolic 130-139 mmHg OR diastolic 80-89 mmHg. This patient has systolic 134 (in the 130-139 range) and diastolic 86 (in the 80-89 range), meeting Stage 1. Under JNC 7, this same reading (134/86) would classify as pre-hypertension (120-139/80-89), NOT hypertension. This distinction is critical — always state which system you are using. The ACC/AHA 2017 lowering of the threshold from 140/90 to 130/80 mmHg was based on evidence of increased cardiovascular risk and improved outcomes with earlier treatment initiation.