Page 6 of 19
IM9.3-5 | Anaemia Clinical Evaluation — SDL Guide (Part 2)
Generating and Prioritising the Differential Diagnosis
After completing the history and examination, the clinician constructs a differential diagnosis — a ranked list of possible diagnoses, ordered by probability given the specific clinical data, with the most dangerous and most treatable diagnoses explicitly considered even if less probable. This is the competency tested by IM9.5. The process has three steps: pattern recognition (matching the clinical data to the known clinical profiles of each anaemia type), probability estimation (using epidemiological and context-specific priors to rank diagnoses by likelihood), and safety-netting (explicitly including diagnoses that, if missed, would cause serious harm).
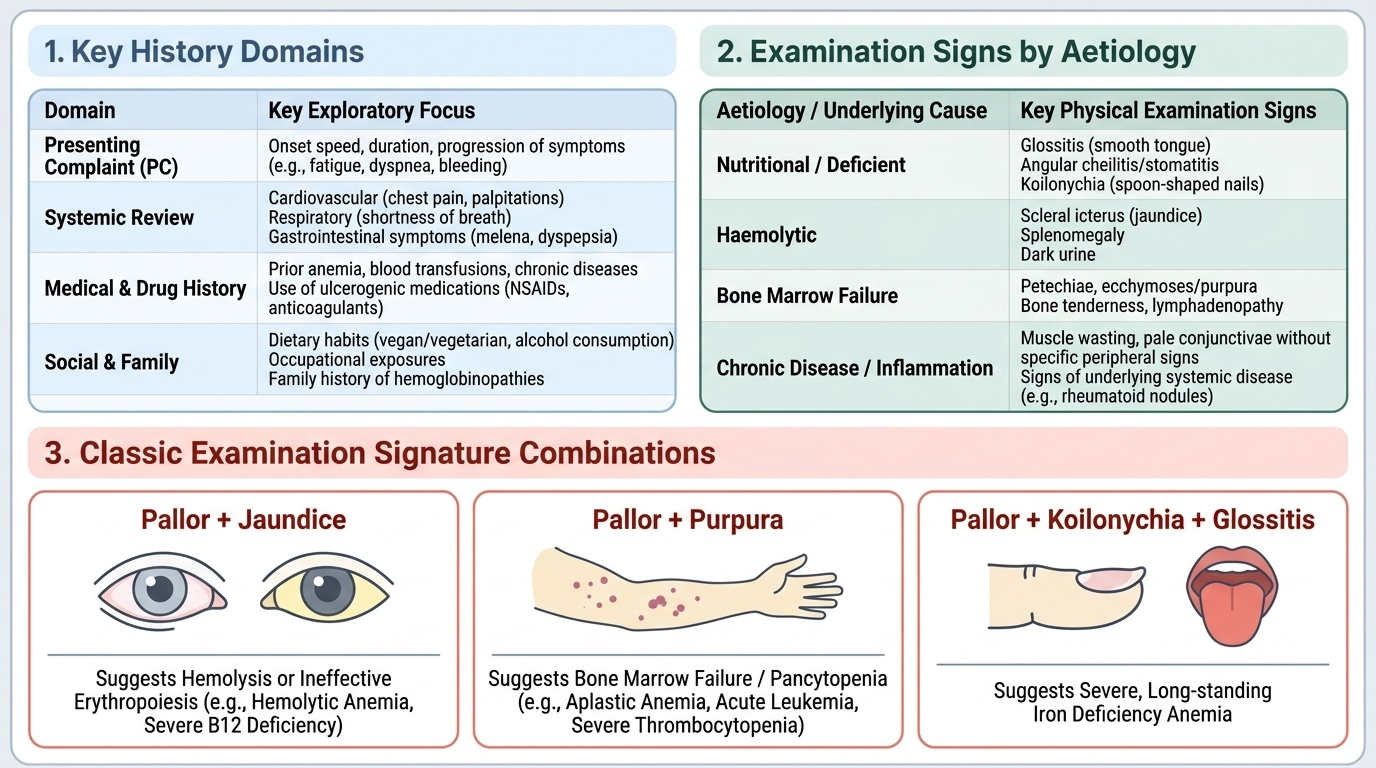
Step 1 — Morphological hypothesis from examination. Even before any investigation, the examination generates a morphological hypothesis. The combination of pica + koilonychia + smooth tongue + pallor without jaundice in a young woman suggests IDA with high probability. The combination of pallor + jaundice + splenomegaly in a young person from a high-prevalence ethnicity suggests haemolytic anaemia. Smooth beef-red tongue + neurological signs (ataxia, impaired proprioception) in an elderly vegetarian suggests B12 deficiency. Pancytopenia signs (pallor + purpura + recurrent infections) without organomegaly suggest aplastic anaemia. These examination patterns set the prior probability for each diagnostic category before a single test is ordered.
Step 2 — Incorporating epidemiological context. In India, the pre-test probability of IDA in a reproductive-age woman presenting with fatigue and pallor is very high (>70%) — the statistical weight of the background prevalence means IDA must be at the top of the list unless a competing pattern clearly argues otherwise. Similarly, in a tribal community patient from Chhattisgarh with haemolytic anaemia, sickle cell disease and β-thalassaemia have high prior probability. In a 65-year-old male with IDA, colorectal carcinoma has a high enough probability to mandate endoscopic investigation even when another cause (e.g., NSAID use) is apparently present. Never anchor to a benign cause and close the differential prematurely in high-risk demographics.
Step 3 — Building and documenting the prioritised differential. Structure the differential by the morphological category supported by the examination, and within each category, rank by probability:
For a young woman with microcytic anaemia:
1. Iron deficiency anaemia (IDA) — commonest cause in India; menorrhagia, dietary deficiency, hookworm
2. Beta-thalassaemia trait — if from a high-prevalence ethnic background; family history of anaemia
3. Anaemia of chronic disease with microcytosis — if chronic infection or inflammatory disease present
4. Sideroblastic anaemia — rare; consider if drug exposure (isoniazid, chloramphenicol)
For a male adult with normocytic anaemia:
1. Anaemia of chronic disease — if chronic illness (TB, HIV, malignancy, rheumatoid) is present
2. Renal failure anaemia — if CKD known or suspected (check creatinine)
3. Haemolytic anaemia — if pallor + jaundice + splenomegaly or elevated reticulocyte count
4. Acute blood loss — if GI bleeding symptoms or history of haematemesis/melaena
5. Aplastic anaemia / marrow infiltration — if pancytopenia present
For a macrocytic anaemia in any adult:
1. B12 deficiency (dietary) — if vegetarian/vegan, elderly, or from South Asia
2. Folate deficiency — if pregnancy, alcohol use, malnutrition, or on folate-antagonist drugs
3. Hypothyroidism — if symptoms (cold intolerance, constipation, weight gain, bradycardia) present
4. Liver disease / alcohol — if alcohol history, elevated liver enzymes, spider naevi, parotid enlargement
5. Myelodysplastic syndrome — if elderly with unexplained macrocytic anaemia not responding to B12/folate
Safety-netting rule: In every adult with unexplained IDA, include 'GI malignancy' in the differential and state explicitly in the clinical notes what investigation is being ordered to exclude it. A male or postmenopausal woman with IDA has GI malignancy in their differential until excluded by endoscopy — this is a medico-legal and patient safety standard, not just a clinical consideration.
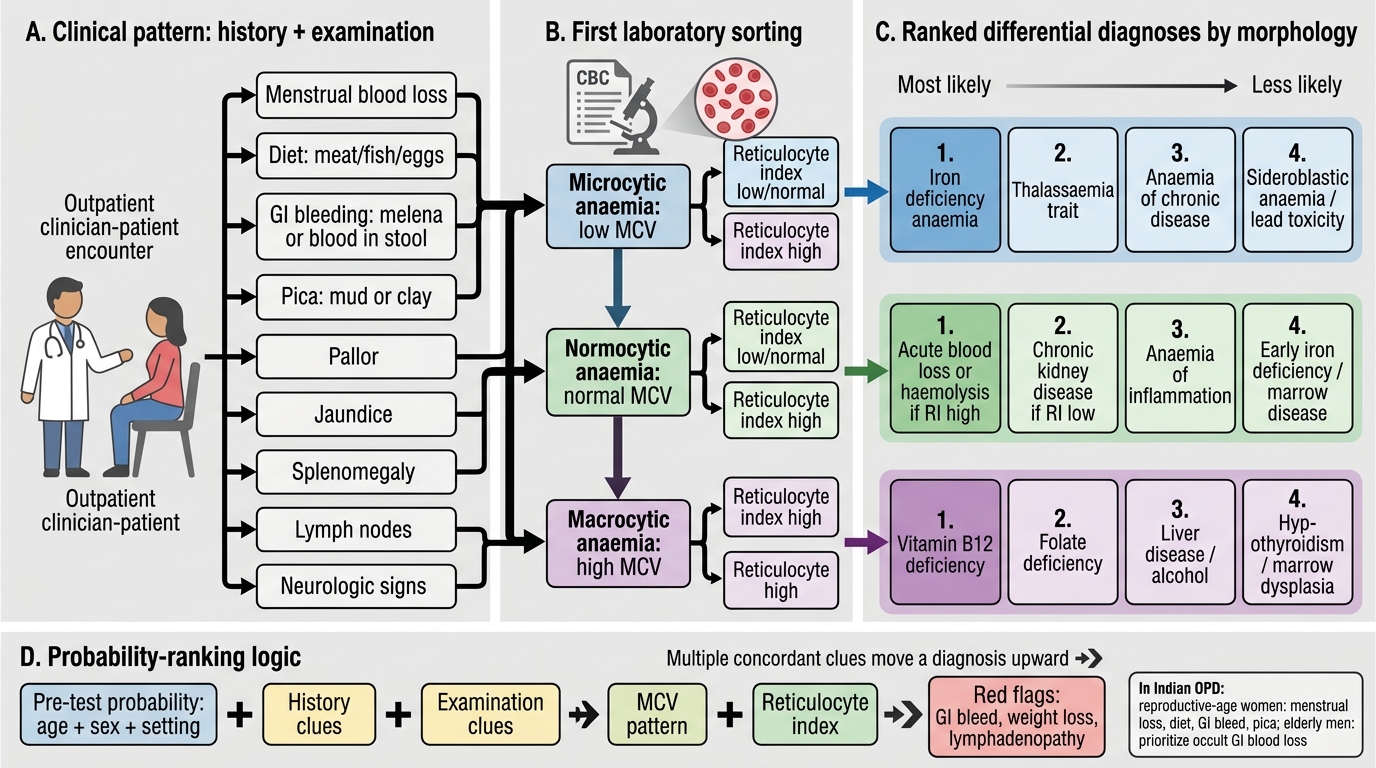
Anaemia Differential Diagnosis by Clinical Pattern, MCV, and Reticulocyte Index
Applied Practice: Integrating History, Examination, and Differential
Translating the individual skills of history-taking, examination, and differential diagnosis generation into a coherent, efficient, and patient-centred clinical encounter requires deliberate practice. The following principles guide the applied integration of these skills, with attention to the unique features of the Indian clinical environment where anaemia evaluation is frequently performed in resource-limited outpatient settings with limited time per patient.
Efficiency principle: In a busy OPD, the initial anaemia evaluation should target the high-yield domains first. The four highest-yield questions for aetiology in Indian women are: (1) How many days does your period last, and how many pads do you use on your heaviest day? (2) Do you eat meat, fish, or eggs? (3) Have you noticed any blood in your stools or black, tarry stools? (4) Have you been eating mud or clay? These four questions take less than 2 minutes and classify the vast majority of reproductive-age women into IDA-likely (positive answers to 1, 2, 4) or warrant-further-investigation (positive answer to 3). In elderly men, the single highest-yield question is about GI bleeding symptoms.
Documentation standard: The structured anaemia assessment must be documented to the SH competency standard. The written history should include: presenting complaint with duration and functional impact; all seven history domains (symptoms, diet, GI bleeding, menstrual/obstetric, medications, family history, systems review); examination findings at all four pallor sites plus cardiac and abdominal examination; a clearly stated differential diagnosis ranked by probability; and the investigation plan tied to the differential.
Patient communication: Many Indian patients present late because they attribute symptoms to 'weakness' or overwork and do not identify them as a medical problem requiring investigation. Communication at the end of the clinical evaluation should be simple, direct, and non-judgmental: explain that the blood count shows a low blood level, describe what this means for the body in simple terms (blood carries oxygen; low blood means less oxygen reaching the muscles and brain), explain why investigations are needed before starting treatment (because the treatment depends entirely on the cause), and set a clear timeline for the next steps. Avoid jargon; use the patient's own language where possible.
Referral indications (IM9.5 — identifying when specialist input is needed): Refer immediately to haematology or internal medicine specialist in any patient with: (a) unexplained pancytopenia (aplastic anaemia, myelodysplasia, acute leukaemia must be excluded urgently); (b) suspected haematological malignancy (lymphadenopathy, splenomegaly, weight loss, night sweats, bone pain); (c) haemolytic anaemia requiring specific typing (AIHA, hereditary spherocytosis, MAHA — specialist lab tests and management required); (d) thalassaemia major or confirmed sickle cell disease (specialist transfusion programme); (e) IDA unresponsive to 8–12 weeks of adequate oral iron therapy (malabsorption, occult bleeding, incorrect diagnosis); (f) anaemia with Hb <6 g/dL or haemodynamic compromise (urgent management needed). These indications should be memorised as they test a clinician's ability to recognise the limits of primary-care management.
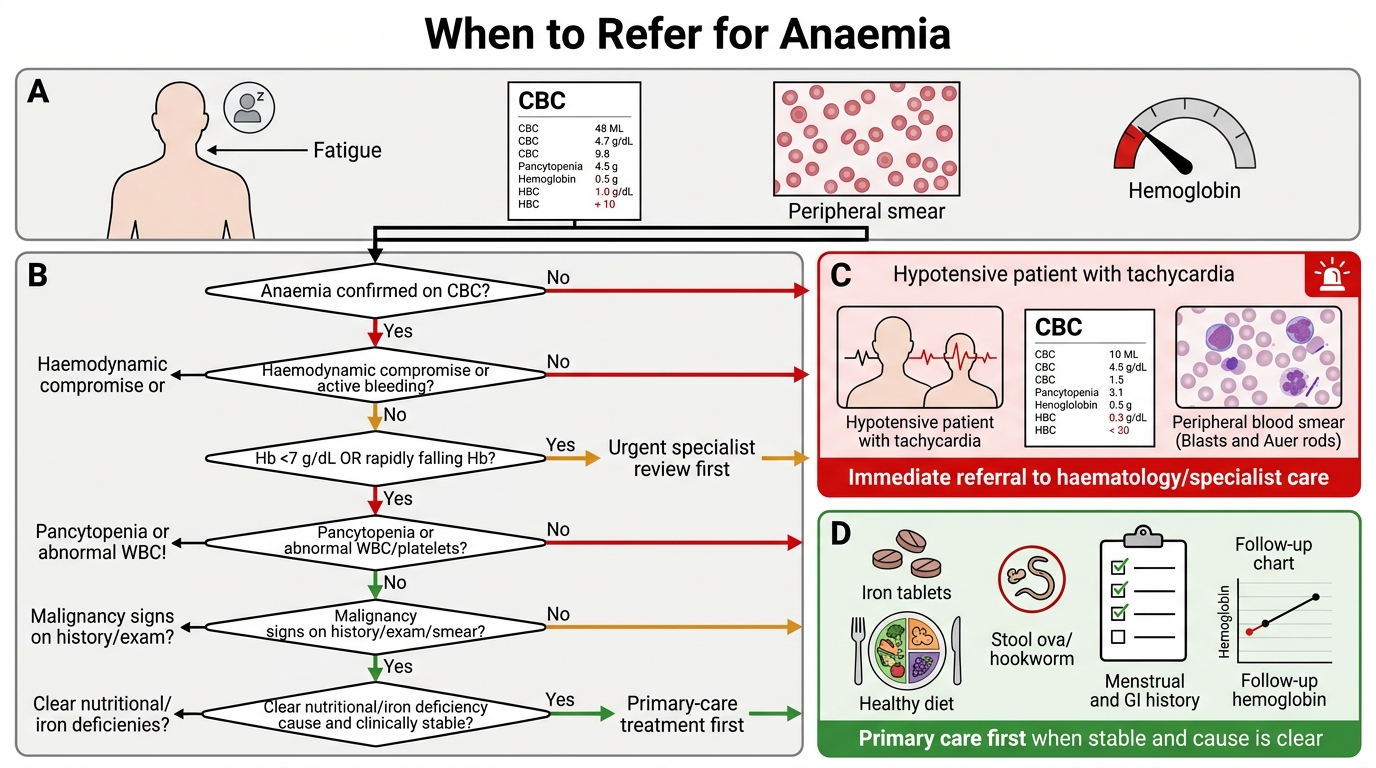
When to Refer for Anaemia
SELF-CHECK
A 45-year-old male farmer presents with fatigue and pallor for 4 months. He is from rural Karnataka and walks barefoot. His Hb is 7.6 g/dL, MCV 70 fL, RDW 19%, ferritin 6 µg/L. He has no GI symptoms. Which additional HISTORY DOMAIN would provide the most important clue to the likely cause of his IDA?
A. Family history of haemolytic anaemia
B. Dietary history focusing on B12 intake
C. Occupational and travel history including footwear practice and soil exposure
D. Neurological symptoms including paraesthesias and balance difficulty
Reveal Answer
Answer: C. Occupational and travel history including footwear practice and soil exposure
This is microcytic hypochromic anaemia with low ferritin = IDA. In a male (menstrual loss excluded), the two most important causes of IDA are GI blood loss and hookworm infestation. The history of bare-foot walking in a rural Karnataka farmer with IDA is a classic hookworm exposure profile — Ancylostoma duodenale penetrates skin through bare feet, migrates to the intestine, and causes chronic GI blood loss (2–5 mL per 100 worms per day). An occupational and travel history probing footwear practice and soil exposure (farming, walking through fields, open defecation proximity) directly addresses the most likely cause in this demographic. Family history of haemolytic anaemia would not cause microcytic IDA. B12 dietary history and neurological symptoms are relevant for macrocytic/megaloblastic anaemia.
CLINICAL PEARL
The four examination sites for pallor — conjunctivae, palms, tongue, nail beds — do not carry equal diagnostic weight. Conjunctival pallor is the most sensitive and reproducible single sign, with a sensitivity of approximately 85–90% for haemoglobin below 9 g/dL when assessed by an experienced examiner. Palmar pallor is less reliable because skin pigmentation and vasomotor tone confound the assessment. However, the COMBINATION of pallor at multiple sites substantially increases the specificity — a patient who is pale at all four sites with tachycardia and a flow murmur is very unlikely to have a normal haemoglobin. The most important bedside rule: pallor + jaundice = haemolysis until proven otherwise; pallor + purpura = bone marrow failure until proven otherwise; pallor + koilonychia + smooth tongue = IDA until proven otherwise. These three combinations are the highest-yield clinical signatures in anaemia examination.
Self-Assessment: Clinical Evaluation in Practice
The following case scenarios consolidate the three integrated skills of this module — structured history, systematic examination, and prioritised differential diagnosis. For each case, read the clinical data and formulate: (a) the morphological hypothesis from available data, (b) the three most likely diagnoses in order of probability, (c) the one examination finding that most strongly supports the leading diagnosis, and (d) the mandatory investigation to confirm or exclude the most dangerous diagnosis in the differential. These four questions operationalise the IM9.3, IM9.4, and IM9.5 competencies at the SH (applied skill) level. Work through each case before reading the analysis — the disciplined practice of reasoning from clinical data to diagnosis, rather than passively reading the answer, is what builds durable clinical skill.
Provided image
Case 1: Sunita, 35-year-old housewife, Gujarat. Fatigue and exertional dyspnoea for 6 months. Eats no meat or fish, drinks tea with every meal. Heavy periods (8–10 pads/day for 7 days). Pallor at all four sites. Tongue smooth, angular stomatitis. No jaundice, no splenomegaly. Hb 7.2 g/dL.
Formulation: (a) Morphological hypothesis: microcytic hypochromic IDA pattern (heavy menorrhagia + dietary non-haem diet + tea inhibitor). (b) Differential: 1st IDA (menorrhagia + dietary); 2nd β-thalassaemia trait (Gujarat — high prevalence); 3rd ACD if chronic disease present (nothing to suggest here). (c) Most supportive examination finding: koilonychia + smooth tongue + pallor without jaundice — the IDA examination signature. (d) Mandatory investigation to exclude dangerous diagnosis: in a premenopausal woman, GI malignancy is a lower priority — but uterine cause (fibroids, endometrial pathology) should be excluded with pelvic ultrasound given severity of menorrhagia. However, the investigation to confirm/exclude thalassaemia as a concurrent aetiology is HPLC.
Case 2: Prakash, 60-year-old retired teacher, Kerala. 3 months of fatigue, one episode of melaena 6 weeks ago (told it was 'piles'). Now presents with Hb 7.8 g/dL, MCV 72 fL. No pallor at conjunctivae initially noted by the nurse — but on formal examination by the MBBS student, conjunctival pallor is present bilaterally. Pulse 98/min.
Formulation: (a) Morphological: microcytic IDA. (b) Differential: 1st GI malignancy (60-year-old male + melaena + IDA = GI malignancy until proven otherwise); 2nd peptic ulcer disease (melaena); 3rd colorectal carcinoma (specifically). (c) Most supportive examination finding: conjunctival pallor with tachycardia in the context of melaena. (d) Mandatory investigation: colonoscopy + upper GI endoscopy — cannot attribute IDA in a 60-year-old male to 'piles' without excluding proximal GI malignancy; haemorrhoids do not cause melaena.
Case 3: Kavitha, 22-year-old student, Tamil Nadu. Incidentally found to have Hb 10.2 g/dL at insurance medical. MCV 66 fL. Asymptomatic. Mother has 'mild anaemia'. Eats a mixed diet. No menorrhagia. No GI symptoms.
Formulation: (a) Morphological: microcytic with no symptoms and moderate family history — consider thalassaemia trait as the leading hypothesis (asymptomatic, family history, Tamil Nadu higher prevalence). (b) Differential: 1st β-thalassaemia trait; 2nd IDA (always possible); 3rd combined IDA + thalassaemia trait. (c) Most supportive examination finding: likely no specific signs (thalassaemia trait is clinically silent) — the diagnosis rests on investigations. (d) Mandatory investigation: serum ferritin (exclude concurrent IDA) + HPLC (HbA2 >3.5% confirms β-thalassaemia trait); if both positive, she has thalassaemia trait with concurrent IDA.