Page 10 of 19
IM9.6-9 | Anaemia Diagnostic Testing — SDL Guide (Part 3)
Constructing an Integrated Diagnostic Plan
The ability to construct an integrated diagnostic plan — selecting the right sequence of investigations for a specific clinical presentation, interpreting them as a pattern, and knowing when to escalate to confirmatory or invasive testing — is the apex skill of anaemia diagnostics and corresponds directly to NMC competency IM9.9. The following worked examples demonstrate this reasoning in detail.
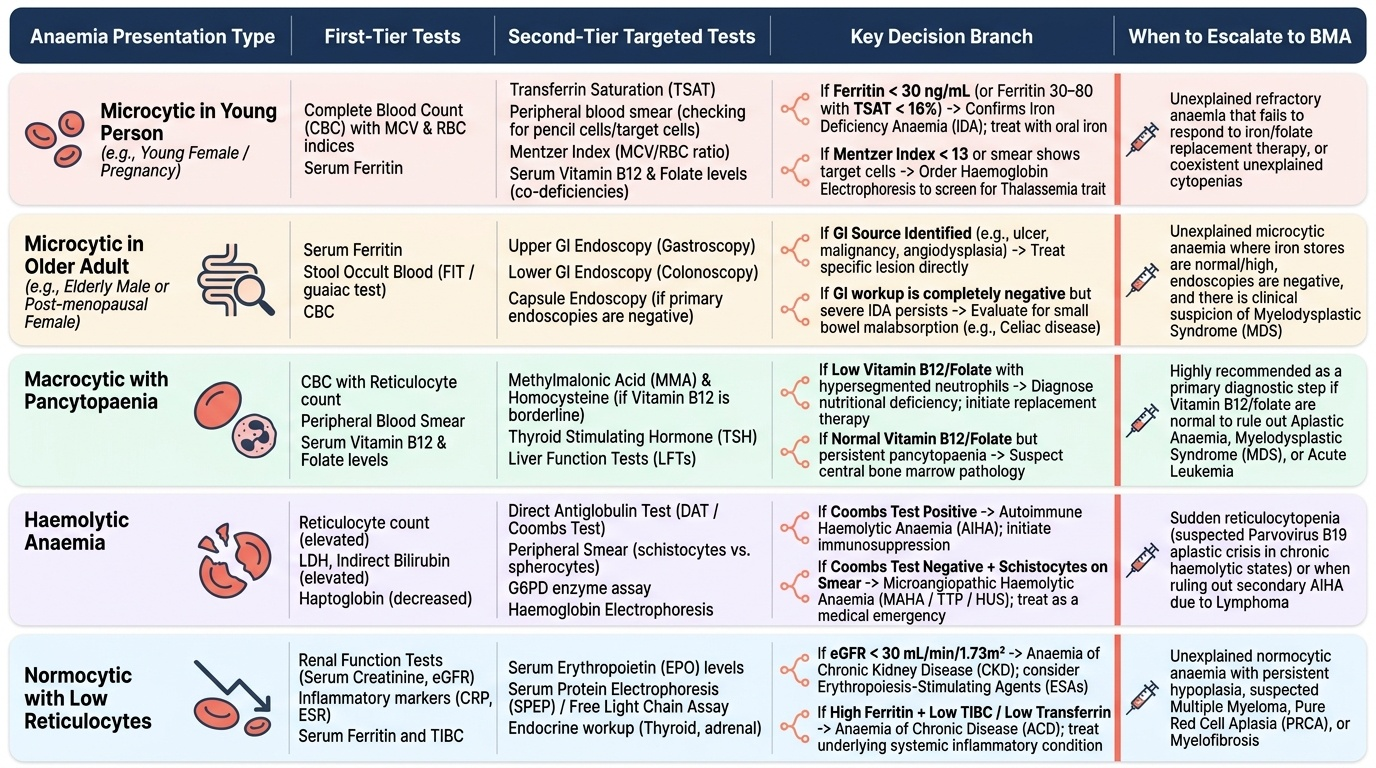
Provided image
Case 1: A 24-year-old primigravida in the third trimester, Hb 8.8 g/dL, MCV 72 fL, presenting at antenatal clinic.
Clinical pre-test probability: IDA is overwhelmingly likely — pregnancy is a high-demand state for iron (foetal needs plus expanding maternal red cell mass), and the WHO reports that 40–50% of pregnant women in India are anaemic, predominantly from IDA. The diagnostic plan: (1) Serum ferritin — if <30 ng/mL, IDA confirmed without further tests; (2) if ferritin is 30–80 ng/mL (a range that can be physiologically raised in pregnancy despite depleted stores), add TSAT (<16% confirms iron-restricted erythropoiesis); (3) Peripheral smear to check for pencil cells confirming the microcytic-hypochromic picture; (4) MCV/RBC (Mentzer index) to screen for coexistent thalassaemia trait (important before starting iron if there is clinical suspicion); (5) Serum B12 and folate given the high prevalence of combined deficiency in pregnancy. Decision rule: ferritin <30 plus TSAT <16% — treat with oral iron plus folate without further workup; Mentzer index <13 or smear shows target cells — add haemoglobin electrophoresis before committing to treatment.
Case 2: A 62-year-old male farmer presenting with insidious weight loss and Hb 9.2 g/dL, MCV 75 fL.
Clinical pre-test probability: new-onset microcytic anaemia in an elderly man requires exclusion of occult gastrointestinal blood loss from colorectal carcinoma before a diagnosis of nutritional IDA is accepted. A fundamental principle of internal medicine is that IDA in an adult male or post-menopausal female must always prompt a search for a GI bleeding source. Diagnostic plan: (1) Serum ferritin — likely low, confirming IDA; (2) Stool occult blood test (guaiac or faecal immunochemical test); (3) Upper GI endoscopy (gastroscopy) — peptic ulcer, gastric carcinoma; (4) Lower GI endoscopy (colonoscopy) — colorectal carcinoma, angiodysplasia; (5) If both endoscopies are negative — capsule endoscopy or CT enterography for small bowel pathology. The key: IDA in this demographic is NEVER attributed to diet alone without complete GI investigation.
Case 3: A 19-year-old woman with Hb 7.1 g/dL, MCV 105 fL, marked macrocytosis with pancytopaenia (WBC 2.8 × 10⁹/L, platelets 96 × 10⁹/L), peripheral smear showing oval macrocytes and hypersegmented neutrophils.
Clinical pre-test probability: megaloblastic anaemia with pancytopaenia — severe deficiency causing haematological failure of all three cell lines. Diagnostic plan: (1) Serum B12 — likely very low; (2) Serum and red cell folate; (3) Anti-intrinsic factor antibodies and anti-parietal cell antibodies (to confirm pernicious anaemia, relevant in a young woman with autoimmune risk); (4) MMA and homocysteine — to confirm metabolic B12 deficiency and distinguish B12 from folate as the primary driver; (5) Thyroid function tests (hypothyroidism causes mild macrocytosis and can coexist); (6) Dietary and medication history. BMA is generally not required in pure megaloblastic pancytopaenia where the peripheral findings are diagnostic — but is indicated if dysplastic features on the smear raise concern for MDS.
SELF-CHECK
A 68-year-old woman with rheumatoid arthritis on long-term NSAIDs and methotrexate presents with Hb 8.4 g/dL, MCV 74 fL, serum ferritin 180 ng/mL, TIBC 200 µg/dL, and transferrin saturation 14%. She has no overt GI bleeding. Which interpretation and next step is MOST accurate?
A. Ferritin 180 excludes iron deficiency; treat as pure ACD with erythropoiesis-stimulating agent
B. Low TIBC alone confirms ACD; no further iron workup is needed
C. TSAT <16% with suppressed TIBC in an inflammatory setting suggests functional iron deficiency complicating ACD; check soluble transferrin receptor and stool occult blood given NSAID use
D. Start oral iron for confirmed IDA since ferritin is unreliable as an acute-phase reactant in rheumatoid arthritis
Reveal Answer
Answer: C. TSAT <16% with suppressed TIBC in an inflammatory setting suggests functional iron deficiency complicating ACD; check soluble transferrin receptor and stool occult blood given NSAID use
This is a complex case with overlapping contributors. TSAT of 14% (below the 16% threshold for iron-restricted erythropoiesis) indicates that iron is not being delivered adequately to the erythron, even with a ferritin of 180 ng/mL. In ACD from rheumatoid arthritis, hepcidin is elevated (driven by IL-6), blocking ferroportin and sequestering iron in macrophages — iron stores appear adequate on ferritin, but functional iron delivery to erythroid precursors is impaired. The microcytic MCV (74 fL) could reflect ACD or concurrent true IDA from NSAID-induced GI blood loss — a real possibility given long-term NSAID use. Soluble transferrin receptor (sTfR), which rises in true iron deficiency but is not elevated by inflammation, helps distinguish functional from absolute iron deficiency. Stool occult blood should be checked given NSAID use. Treating with an ESA without resolving the iron question would be incomplete.
Self-Assessment: Diagnostic Reasoning in Anaemia
You have now covered the full spectrum of anaemia diagnostic investigation — from the structured tiered approach through the haemogram and red cell indices, peripheral smear morphology, iron studies, B12 and folate markers, haemolytic indices, and bone marrow examination, through to integrated diagnostic plan construction for common clinical presentations. This self-assessment section challenges you to apply that knowledge to clinical scenarios that test your reasoning rather than mere recall. For each scenario, construct your diagnostic plan before reading the analysis.
Scenario A: A 30-year-old tribal woman from Odisha presents with chronic haemolytic jaundice, splenomegaly, and recurrent episodes of severe anaemia requiring transfusions. Her current Hb is 6.8 g/dL, reticulocyte count 9%, LDH 680 IU/L, unconjugated bilirubin 4.2 mg/dL, and direct Coombs test is negative. The smear shows sickle cells and irreversibly sickled cells.
Analysis: The clinical features — haemolysis, splenomegaly, sickle cells on smear, tribal Odisha background — are diagnostic of sickle cell disease (HbSS). Confirmatory test: haemoglobin electrophoresis showing predominantly HbS and no HbA (or very little in HbSC disease). HbF level should be measured as higher HbF is protective and correlates with milder disease. Severity markers: LDH, unconjugated bilirubin, haptoglobin (will be undetectable in chronic intravascular haemolysis), reticulocyte count. Organ damage assessment: serum creatinine and urine protein-creatinine ratio (sickle nephropathy), ophthalmology review (proliferative sickle retinopathy), transcranial Doppler in children (stroke risk assessment).
Scenario B: A 50-year-old man with CKD stage 4 (eGFR 18 mL/min/1.73m²) has Hb 9.0 g/dL, MCV 84 fL (normocytic), reticulocyte count 0.8%, serum ferritin 220 ng/mL, and TSAT 22%.
Analysis: Normocytic anaemia with low reticulocyte count (RPI <2) and adequate iron stores in severe CKD = anaemia of chronic kidney disease, predominantly from relative erythropoietin (EPO) deficiency. The kidney produces 90% of circulating EPO; as eGFR falls below 30 mL/min, EPO production becomes inadequate and the marrow has insufficient stimulus to maintain haemoglobin. Iron studies here are reassuring — ferritin 220 ng/mL and TSAT 22% indicate adequate iron stores. No additional iron workup is required. Management: erythropoiesis-stimulating agent (ESA) — recombinant human erythropoietin (epoetin alfa or darbepoetin alfa) with target Hb 10–11.5 g/dL (KDIGO recommendation). Iron supplementation should be co-administered if TSAT falls below 20% during ESA therapy, because ESA drives rapid iron utilisation. Before starting ESA, other reversible causes of anaemia must be excluded — B12 or folate deficiency, hypothyroidism, blood loss.
Self-check reference:
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
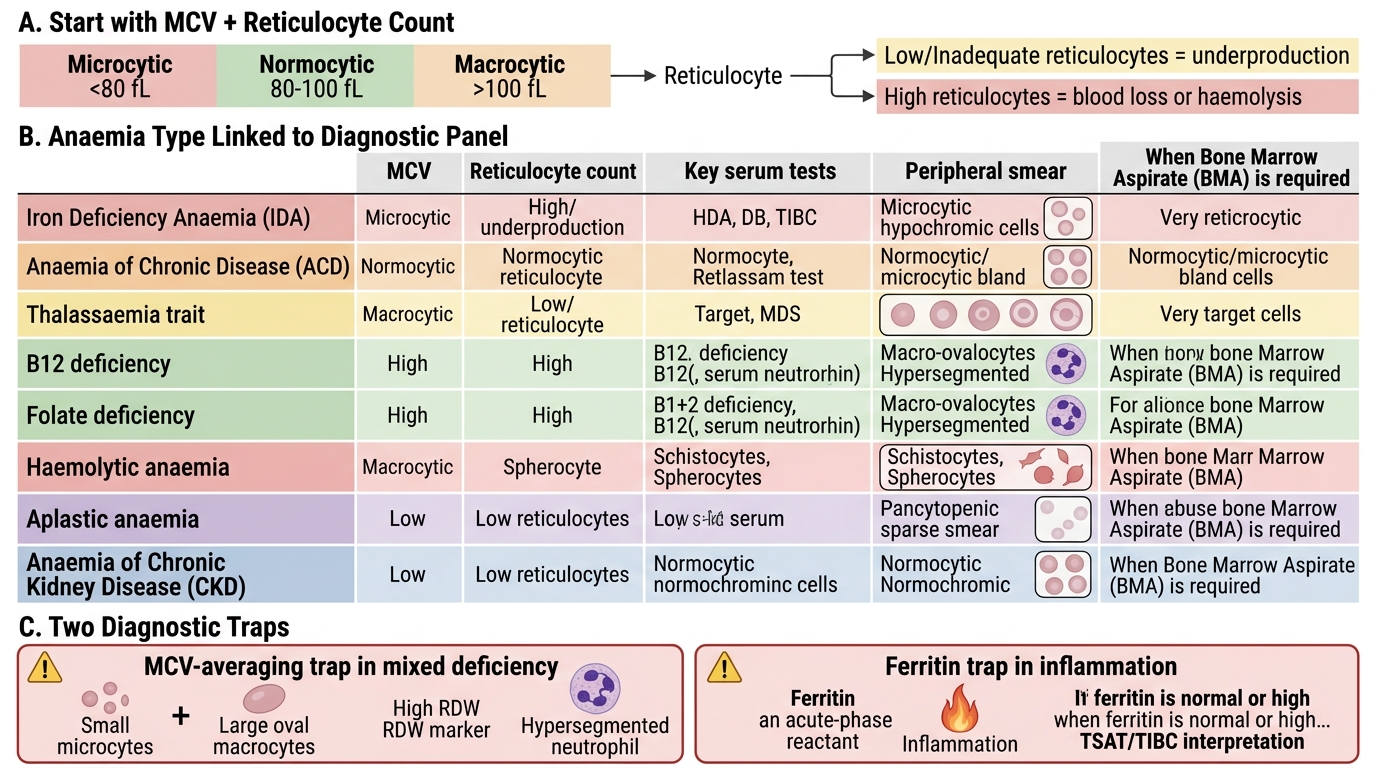
Anaemia Diagnostic Panel Summary
CLINICAL PEARL
Two high-yield diagnostic traps to commit to memory:
First, the MCV-averaging trap in mixed deficiency: when a patient has concurrent iron deficiency (causing microcytosis) and B12 or folate deficiency (causing macrocytosis), the MCV may be deceptively normal in the 85–95 fL range, because the two opposing size effects cancel each other out mathematically. The peripheral smear will betray the truth — a dimorphic population of both small microcytic cells and large oval macrocytes, alongside hypersegmented neutrophils. The RDW will be markedly elevated. Always request a peripheral smear and RDW when the clinical story suggests mixed deficiency — for example, a pregnant woman with menorrhagia and a strict vegetarian diet, or a long-term metformin user with dietary folate insufficiency.
Second, the ferritin trap in inflammation: a normal or high serum ferritin does NOT exclude iron deficiency in a patient with active infection, chronic inflammation, liver disease, or malignancy. Ferritin is an acute-phase reactant and can be elevated even when tissue iron stores are genuinely depleted. In these patients, transferrin saturation (<16%), soluble transferrin receptor (elevated in IDA even in the presence of inflammation, unlike ferritin), and — if needed — bone marrow Prussian blue staining are the reliable diagnostic tools for confirming or excluding iron deficiency.