Page 5 of 11
SU13.3-4 | Organ Donation Ethics and Counselling — SDL Guide (Part 2)
Interpreting the Family's Response and Reading the Room
Counselling a family for donation is a skill of reading and responding, not of reciting a script, and a large part of the skill is correctly interpreting where the family is emotionally and what their words and silences are telling you. The first thing to interpret is whether the family has actually accepted the death. A family who still speak of their relative in the present tense, who point to the rising chest on the ventilator as proof of life, have not yet understood that brain-stem death is death — and a donation request made before that understanding lands will feel, to them, like a request to kill. Recognising this tells you to slow down and re-establish the reality of death before anything else. The second thing to interpret is the family's readiness and cues: a family who begin to ask about what happens next, who mention that their relative was a kind or giving person, or who themselves raise the subject, are signalling openness; a flat, exhausted withdrawal or an immediate, firm 'no' signals that the answer is refusal and must be respected. The third is the presence of cultural and religious concerns, which you must take seriously and never dismiss — many traditions in fact support donation as an act of charity, and gently providing accurate information (for example that most faiths permit donation, and that the body is treated with respect) can resolve a fear without any pressure. Throughout, you are interpreting grief: tears, anger, denial and bargaining are normal responses to catastrophic loss, not obstacles to be overcome. The skill is to respond to the emotion in front of you — to make space for it — rather than to push past it toward the outcome you want. Misreading the room, and pressing a request on a family who are not ready, is the commonest and most damaging error in donation counselling.
Counselling a Family for Organ Donation: A Structured Approach (Simulated Practice)
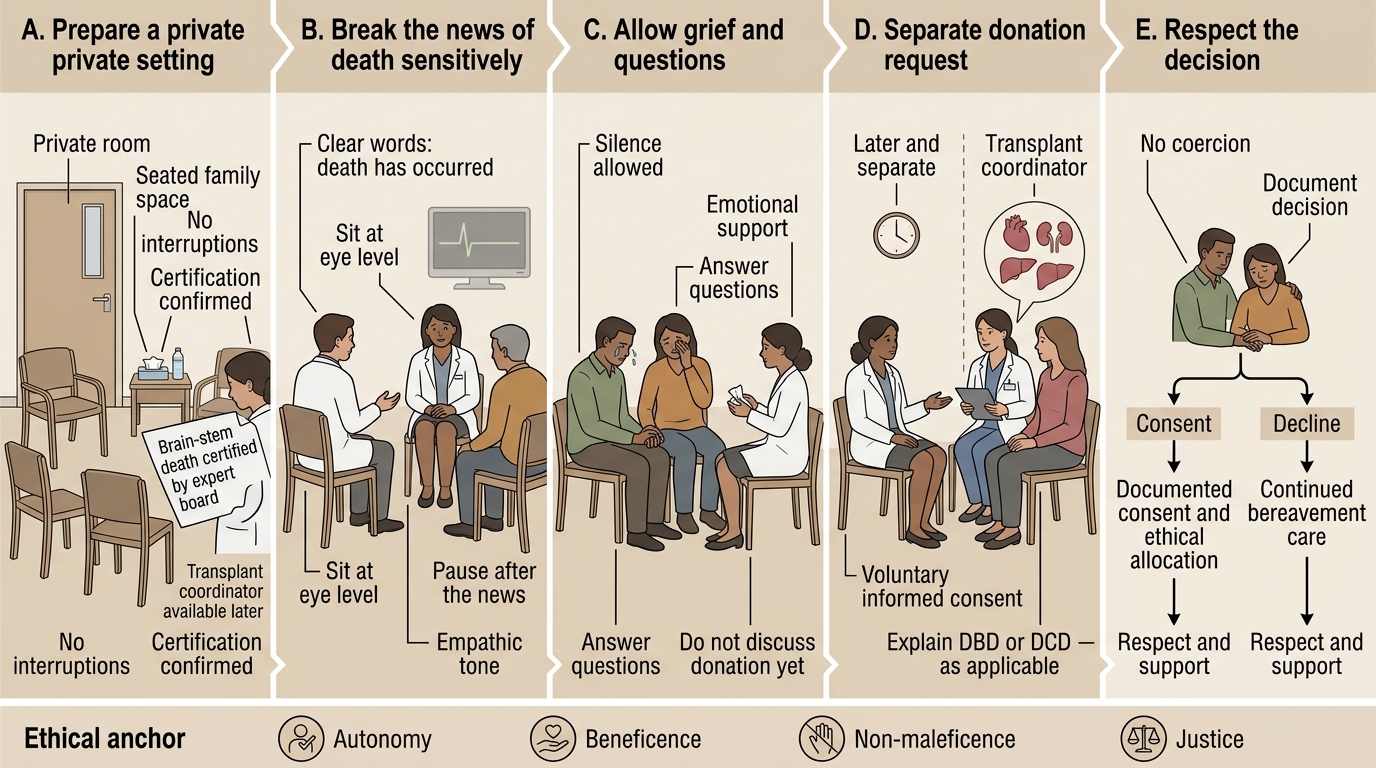
Knowing the law and reading the room come together in the actual conversation, and the competency is demonstrated by conducting that conversation cleanly and compassionately in simulation. The structured approach is practised until it is natural, and its single most important principle is decoupling: the notification of death and the request for donation must be handled as two distinct steps, separated in time, never merged into one breath. The sequence is as follows. First, prepare the setting: a private, quiet room, enough time, the right people present (ideally including a transplant coordinator), and your phone silenced. Second, break the news of death clearly and without jargon — say that the person has died, use the word 'death', explain brain-stem death simply if relevant, and then stop talking. Third, allow the family to grieve: be silent, let them react, answer their immediate questions, and confirm that they have understood that their relative has died. Only when the death has been understood and the family has had time do you move to the fourth step: introduce the possibility of donation, gently and without pressure — often best raised by the transplant coordinator — framing it as an opportunity to help others and as something the deceased may have wished, and giving the family time and space to decide. Fifth, make the request and respect the answer: provide honest information, answer concerns about the process and the body, never coerce or imply obligation, and accept a refusal graciously and with the same compassion as an acceptance. Throughout, you remain truthful, you protect the family's dignity, and you treat their decision — whichever way it falls — as the right one for them. Repeated supervised simulation of this sequence, with feedback, builds the muscle memory and the emotional steadiness that real families deserve.
Empathic Family Counselling for Organ Donation
Check Your Understanding
Before moving on, consolidate the competency by reasoning through it rather than recalling isolated facts. Walk the whole pathway from a potential donor to a respected decision. Start with the law: under the Transplantation of Human Organs Act 1994 (amended 2011), brain-stem death is recognised as death and certified by an expert board, commercial dealing is forbidden, a near-relative may donate without special scrutiny while a non-near-relative needs Authorisation Committee approval, and deceased donation proceeds as DBD or DCD. Next the ethics: every step is anchored in autonomy (voluntary informed consent), beneficence, non-maleficence (protecting the living donor) and justice (fair allocation). Then the skill: when you sit with the brain-stem-dead patient's family, you break the news of death first and let it land, and only later — separately, ideally with a transplant coordinator — do you gently raise donation, respecting whatever they decide. Test yourself on four links: can you state the four key provisions of THOTA; can you say who needs Authorisation Committee approval and why; can you distinguish DBD from DCD; and can you explain why decoupling the death notification from the donation request is the central counselling rule? The short question below checks exactly these connections.
CLINICAL PEARL
The single most important rule in donation counselling is DECOUPLING: never break the news of death and ask for organs in the same conversation. Tell the family their relative has died, then stop — let the death be understood and grieved first. Only after the family has accepted the death, and ideally with a trained transplant coordinator, do you separately and gently raise donation. Families approached this way are far more likely to consent and, just as importantly, are spared the lasting trauma of feeling that the doctor was 'after the organs' before their relative was even cold. And whatever they decide — yes or no — their answer is respected without pressure.
SELF-CHECK
A family has just been told their ventilated relative is brain-stem dead and are visibly shocked and tearful. What is the most appropriate immediate next step in counselling?
A. Immediately ask them to consent to organ donation while the organs are still viable
B. Allow them silence and time to grieve and to understand the death, and only later — separately — raise donation
C. Tell them donation is expected of them as a moral duty
D. Avoid mentioning donation at all, since the family is upset
Reveal Answer
Answer: B. Allow them silence and time to grieve and to understand the death, and only later — separately — raise donation
The principle of decoupling requires that breaking the news of death and the donation request be separate steps. Immediately after the news, the family needs silence, time and the chance to understand that their relative has died; pushing a donation request now is coercive and damaging. The request is raised gently and separately once the death is accepted — neither merged with the news nor (the opposite error) omitted altogether, since most families wish to be given the choice.