Page 9 of 16
SU15.1,SU16.1 | Hospital Waste Disposal and Minimally Invasive Surgery — SDL Guide (Part 2)
What Minimally Invasive Surgery Is and How It Works
Minimally invasive surgery (MIS), of which laparoscopy is the abdominal form, is surgery performed through several small (typically 5–12 mm) incisions called ports, using a rod-lens telescope attached to a camera that displays the operative field on a monitor, together with long, slender instruments passed through the other ports — instead of a single large incision. The defining requirement that makes abdominal MIS possible is a working space inside the abdomen, created by a pneumoperitoneum: the peritoneal cavity is insufflated with gas to lift the abdominal wall away from the viscera, giving the surgeon room to see and to operate. The gas used is carbon dioxide (CO2), and the choice is deliberate — CO2 is inert and non-combustible (safe to use near diathermy), highly soluble in blood so any that is absorbed or accidentally enters a vessel is rapidly carried away and exhaled by the lungs, and it is cheap and readily available. The abdomen is insufflated to a controlled working pressure of about 12–15 mmHg. Access is gained either by a closed technique with a spring-loaded Veress needle or by an open (Hasson) cut-down to place the first port safely, after which further ports are inserted under vision. The camera magnifies the field, and because the surgeon operates by watching a screen and manipulating long instruments, MIS demands hand–eye coordination and training quite different from open surgery. Crucially, the absorbed CO2 and the raised intra-abdominal pressure are not without effect: the pressure reduces venous return from the inferior vena cava and splints the diaphragm, while absorbed CO2 raises blood carbon-dioxide levels (hypercarbia) — physiological consequences the anaesthetist must manage and which limit how high and how long the pressure can be sustained.
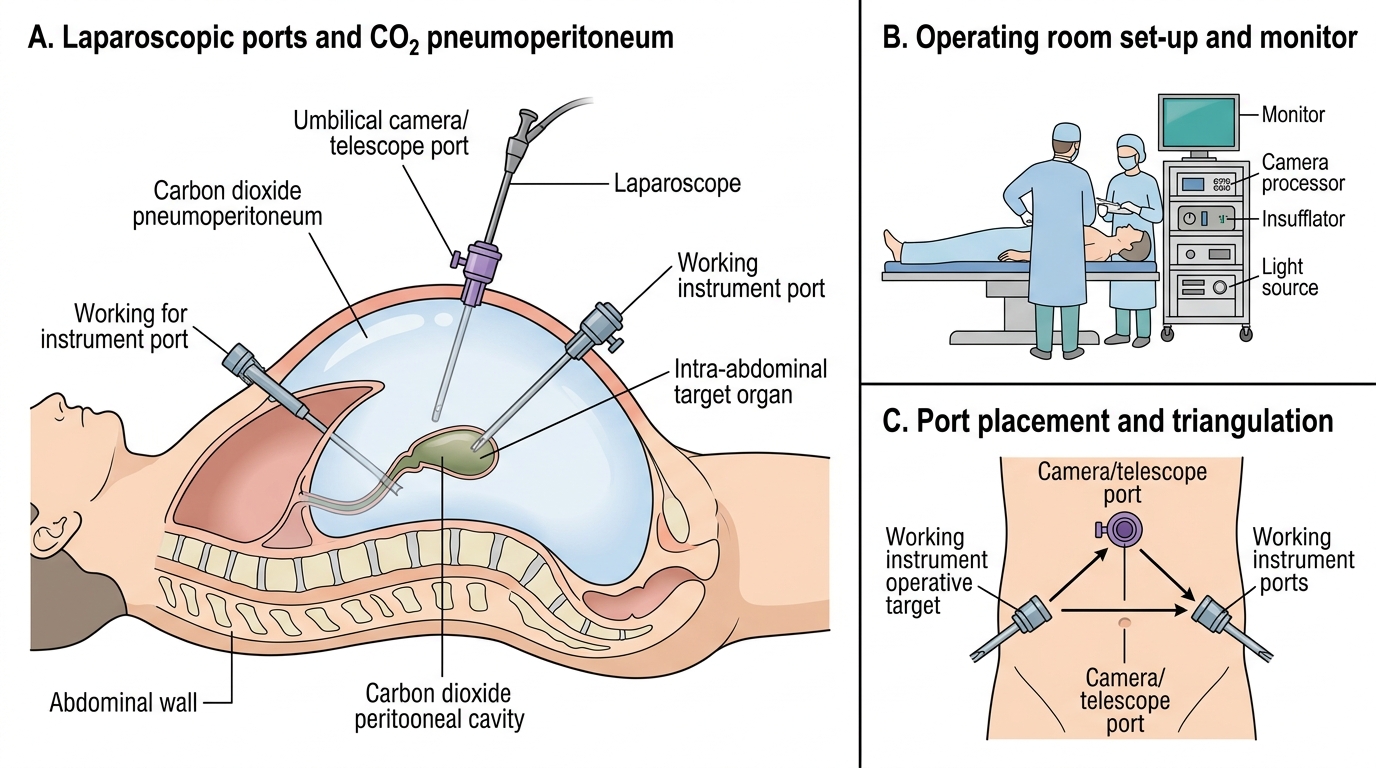
Laparoscopic Set-up with CO2 Pneumoperitoneum
Weighing Indications, Advantages and Disadvantages of MIS
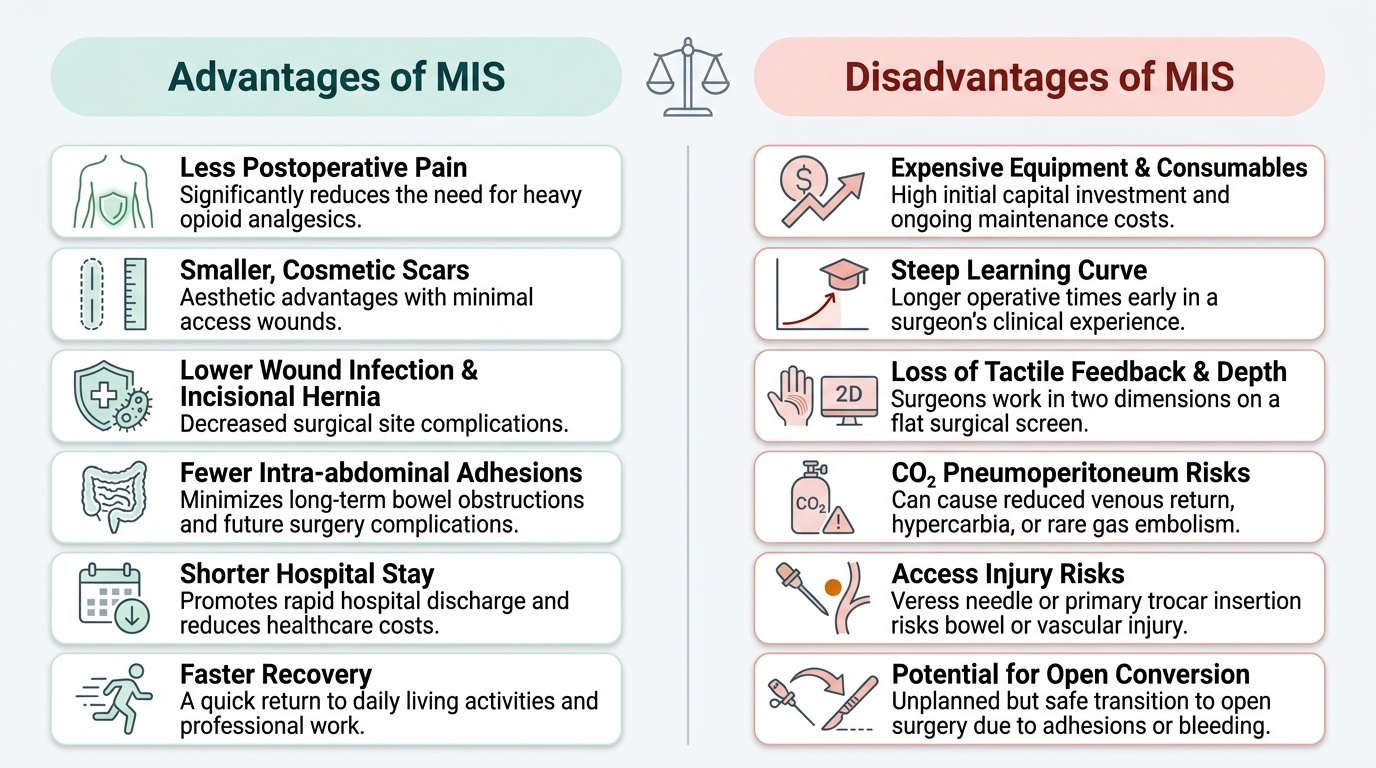
Deciding whether to offer a minimally invasive or an open operation is an act of judgement that balances real benefits against real costs for the individual patient. The indications for MIS are wide and still growing, spanning both diagnostic and therapeutic procedures: diagnostic laparoscopy to inspect the abdomen, and therapeutic operations such as laparoscopic cholecystectomy (now the standard of care for gallstone disease), appendicectomy, inguinal and other hernia repairs, anti-reflux (fundoplication) surgery, bariatric surgery and many colorectal and gynaecological procedures. The advantages flow directly from the smaller wounds: less postoperative pain, smaller and more cosmetic scars, lower rates of wound infection and incisional hernia, fewer intra-abdominal adhesions, a shorter hospital stay, and a faster return to normal activity and work — together a substantial reduction in the harm of access. The disadvantages are equally real and must be weighed: the equipment is expensive and the technique has a steep learning curve, so early in a surgeon's experience operating times are longer; the surgeon loses direct tactile feedback (haptics) and depth perception, working in two dimensions on a screen; and the CO2 pneumoperitoneum carries physiological risks — reduced venous return, hypercarbia and respiratory acidosis, and the rare but catastrophic gas embolism — while gaining access with the Veress needle or trocar risks injury to bowel or major vessels. MIS is therefore not suitable for everyone: it may be inadvisable or require conversion to open surgery in patients with severe cardiorespiratory disease (who tolerate pneumoperitoneum poorly), uncorrected coagulopathy, extensive prior adhesions, or in some emergencies, and any laparoscopic operation may need to be converted to an open operation if it cannot be completed safely — a planned safety step, not a failure. Reading the patient against this balance sheet is the skill the competency tests.
Provided image
| Advantages of MIS | Disadvantages of MIS |
|---|---|
| Less postoperative pain | Expensive equipment and consumables |
| Smaller, more cosmetic scars | Steep learning curve; longer early operative time |
| Less wound infection and incisional hernia | Loss of tactile feedback; two-dimensional view |
| Fewer adhesions | CO2 effects — reduced venous return, hypercarbia, rare gas embolism |
| Shorter hospital stay, faster recovery | Access (Veress/trocar) injury to bowel or vessels; may need conversion to open |
CLINICAL PEARL
Two rules to carry to the wards. For waste: a used needle goes ONLY into the rigid white puncture-proof sharps container and is NEVER recapped — recapping is the single commonest cause of needle-stick injury, and segregation at source is always the responsibility of the person who generated the waste. For MIS: converting a laparoscopic operation to an open one is a sign of good judgement, not failure — if the anatomy is unclear or the operation cannot be completed safely, conversion is the safe choice, and CO2 is chosen for pneumoperitoneum precisely because it is non-combustible and highly soluble, so an accidental gas embolus is rapidly cleared.
Applying Safe Waste Handling and Recognising MIS in Practice
Knowing the rules is necessary but not sufficient — the competency is demonstrated by handling waste correctly at the point of use and by recognising and reasoning about a minimally invasive set-up in the clinical or simulated setting. For waste, the routine becomes automatic with practice: at every procedure, decide as you finish each item which colour it belongs to and place it there immediately — anatomical and soiled material into yellow, contaminated recyclable plastics (tubing, gloves, catheters, urine bags) into red, every sharp straight into the rigid white puncture-proof container without recapping, and broken glass or a removed metallic implant into blue. Keep the correct containers within arm's reach before you start, never overfill them past three-quarters, ensure each is labelled with the biohazard symbol, and report any spill or needle-stick at once so that post-exposure protocols can begin. For MIS, in the operating theatre or on simulated equipment, learn to recognise the components — the insufflator delivering CO2 to the set pressure, the camera and light source feeding the monitor, the ports through which the telescope and instruments pass — and to anticipate the physiology: watch how raised intra-abdominal pressure and absorbed CO2 are reflected in the patient's ventilation and circulation, and understand why the surgeon may ask for the pressure to be lowered or the operation converted. Box trainers and simulators let you practise the unfamiliar two-dimensional, long-instrument coordination of laparoscopy safely. Repeated, supervised practice of both routines is what converts knowledge into the reliable, safe behaviour expected of you around real patients.