Page 4 of 11
SU4.3-4 | Burns Medico-Legal Care and Rehabilitation Counselling — SDL Guide
Learning Objectives
- Discuss the medico-legal aspects of burn injuries, including the doctor's statutory duties, documentation, the dying declaration, and the relevant Indian legal framework (SU4.3).
- Describe the principles of physical and psychological rehabilitation after burns (SU4.4).
- Communicate and counsel a burn patient and family on outcome and rehabilitation, demonstrating empathy and care (SU4.4).
INSTRUCTIONS
Surviving the first 48 hours of a major burn is only the beginning. What follows is a long road of scars, contractures, repeated surgery and profound psychological adjustment — and, in a large proportion of Indian burns, a parallel legal process, because the injury may not have been an accident. This module addresses the two skills the operating textbook rarely teaches: handling a burn as a medico-legal case, and counselling the survivor and family with honesty and empathy. Both are competencies you will be expected to perform, not merely recall. Doing them well protects the vulnerable, supports the law, and turns a frightened, disfigured patient into a partner in their own long recovery.
References
- Bailey & Love's Short Practice of Surgery, Burns (textbook)
- SRB's Manual of Surgery, Burns (textbook)
- Sabiston Textbook of Surgery, Burns and rehabilitation (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old woman, married eight months ago, is brought to casualty with deep burns over most of her trunk and arms. Her husband says her sari caught fire while she was cooking. She is conscious, in pain, and very frightened. As you begin to examine her, two duties begin at once — and they pull in different directions only if you let them. One is purely clinical: airway, fluids, wound. The other is medico-legal and human: this pattern of burns in a recently married woman must make you think, document with extreme care, and consider whether the law needs to be involved — while at the same time you must speak to her and her family with a calm, unhurried empathy that does not accuse anyone but also does not look away. How you handle this moment — the record you write, the questions you ask, the way you break difficult news — may matter as much to this woman's future as the fluids running into her arm.
WHY THIS MATTERS
Burns occupy a unique place in surgical practice because they sit at the meeting point of medicine, law and human suffering. In India, a substantial share of serious burns in young married women are not accidents but homicidal or suicidal, sometimes dowry-related, which means the doctor who first sees them carries real medico-legal responsibility: a careless or incomplete record can let a perpetrator go free or wrongly implicate the innocent. Equally, every survivor of a major burn faces months to years of rehabilitation — scar contractures that freeze joints, disfigurement that changes how they see themselves, and a heavy burden of anxiety, depression and post-traumatic stress. The doctor is the person who must explain all of this, set realistic expectations, and keep the family engaged through a long and demanding course. For these reasons the medico-legal and counselling skills in this module are not optional extras around the 'real' surgery; for the patient in front of you they often determine whether justice is done and whether recovery succeeds.
RECALL
Recall two foundations before applying them. First, from the companion burns-assessment module: you already know how to estimate a burn's depth and its percentage total body surface area (%TBSA), and you know that deep partial-thickness and full-thickness burns are the ones that scar and contract because they destroy the dermis and cannot re-epithelialise on their own. That same clinical assessment — the body-map, the mechanism, the time of the burn — is also the medico-legal record, so accuracy serves both purposes at once. Second, recall the general principles of clinical communication you have met across the curriculum: that consent must be informed, that bad news is broken in a private, unhurried setting in plain language, that you find out what the patient already understands before adding to it, and that responding to emotion with empathy comes before giving more facts. Holding these in mind, we now build the specific medico-legal duties and the burns-counselling skill on top of them.
Why Medico-Legal Care and Counselling Matter in Burns
Two situations make burns different from most surgical conditions and define the skills in this module. The first is that a burn is frequently a medico-legal case. Many serious burns are not accidents: they may be suicidal, homicidal, or assault (including acid attacks), and in the Indian context the burns of a young married woman within a few years of marriage must always raise the possibility of a dowry-related injury. The treating doctor is therefore not only a healer but also, by law, a recorder of evidence and a mandatory informant to the authorities. The second situation is that surviving a major burn opens a long chapter of rehabilitation — physical, in the form of scar and contracture management, and psychological, in the form of coping with disfigurement and trauma — through which the patient and family need to be guided with honest, empathic counselling. The first defines the competency to discuss the medico-legal aspects of burns (SU4.3); the second defines the competency to communicate and counsel on outcome and rehabilitation (SU4.4). Both are performance skills: you will be expected to demonstrate them, not merely describe them, and both begin the moment the patient arrives.
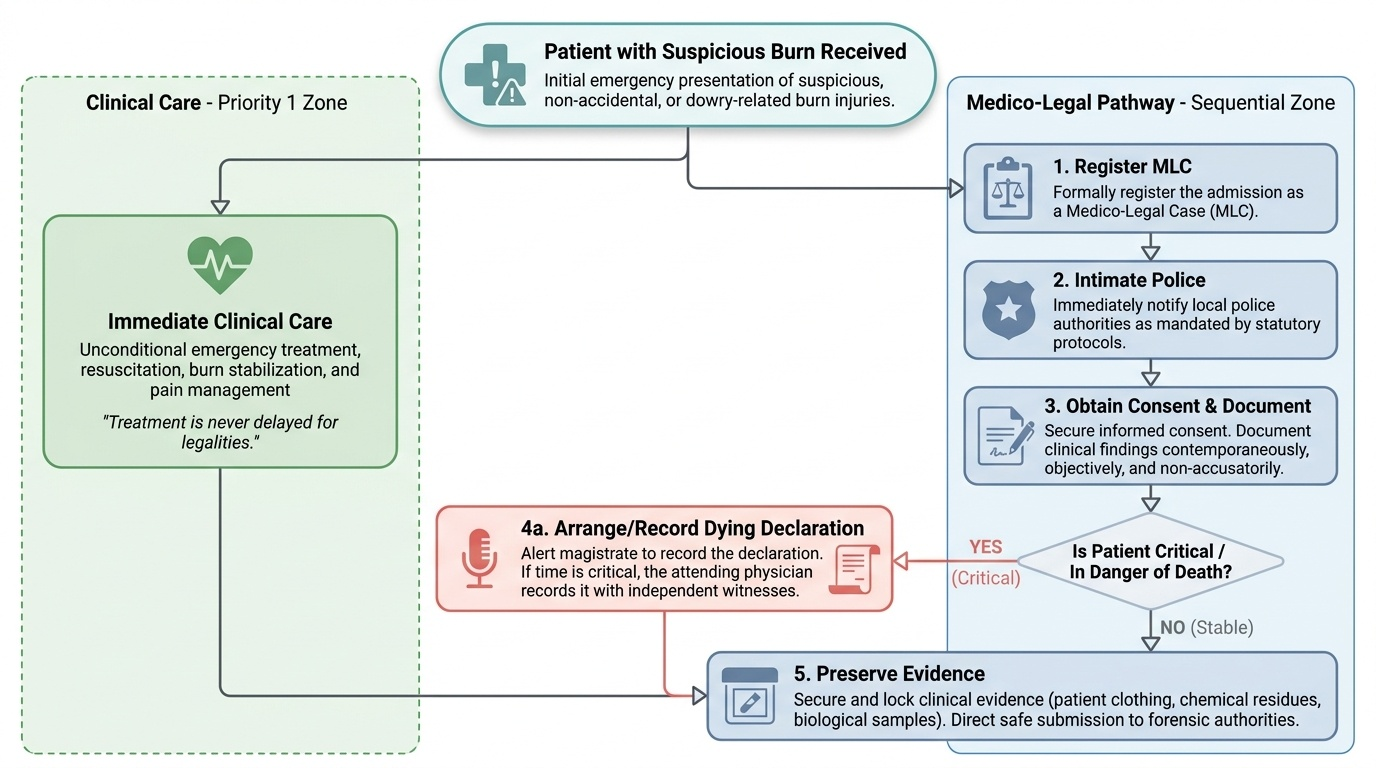
Governing Principles: The Doctor's Medico-Legal Duties and the Statutory Framework
When a burn may be non-accidental, the doctor has clear, non-negotiable duties that run alongside clinical care, and these are governed by a definite statutory framework that you must understand at the level of principle. The first duty is to recognise and register the case as a medico-legal case (MLC) and to intimate the police, because by law certain injuries cannot be treated as private clinical matters. Treatment is never delayed for legalities — saving life always comes first — but the legal process is set in motion in parallel. The doctor must obtain informed consent for examination and treatment wherever the patient is able to give it, document everything contemporaneously, and remain strictly objective and non-accusatory: the doctor records facts and the patient's stated (alleged) history, but it is the court, not the doctor, that decides guilt. A particular alertness is required for the dowry-related, homicidal or suicidal burn, classically in a married woman within seven years of marriage, where the law imposes additional safeguards. Understanding the relevant statutory provisions lets you appreciate why your record matters and what the authorities will need from it.
Provided image
Provided image
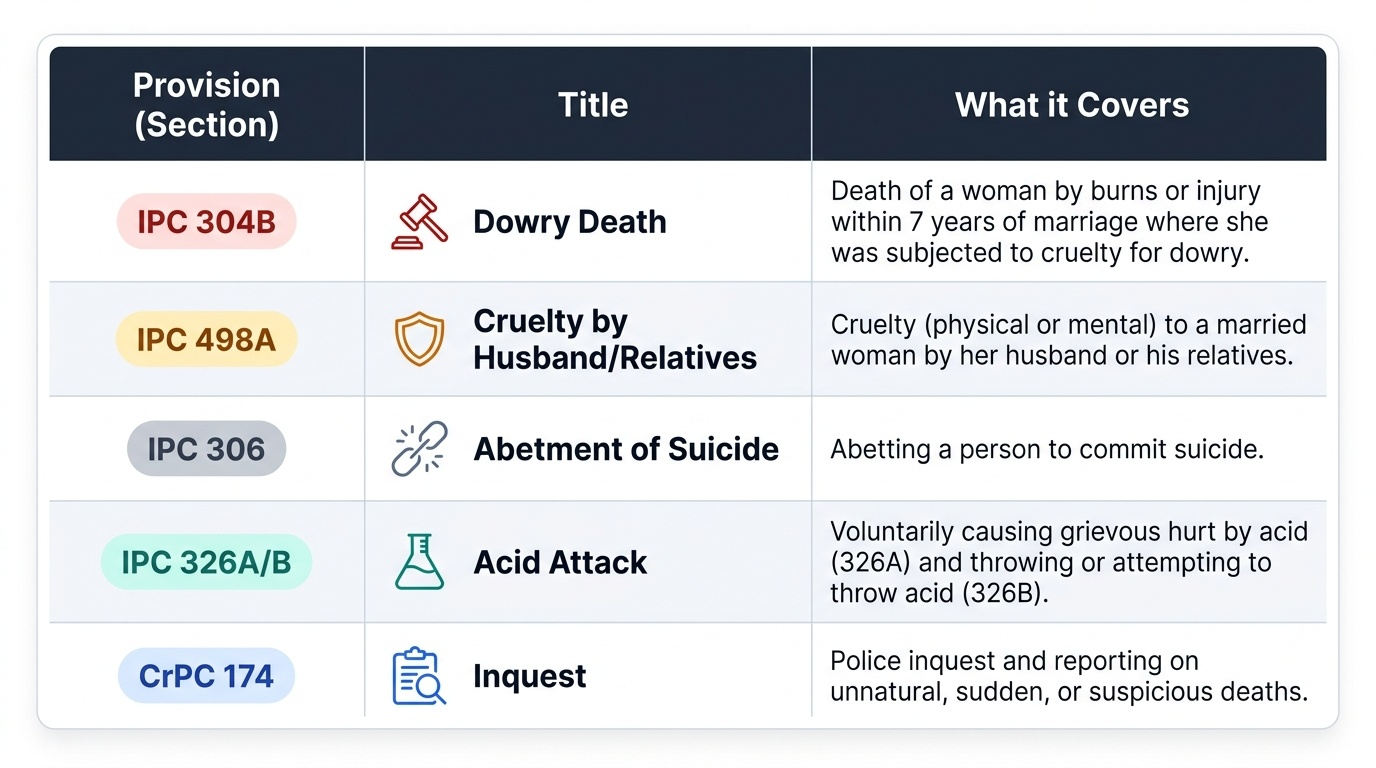
The key Indian statutory provisions a clinician should recognise are:
| Provision | Title | What it covers |
|---|---|---|
| IPC 304B | Dowry death | Death of a woman by burns or injury within 7 years of marriage where she was subjected to cruelty for dowry |
| IPC 498A | Cruelty by husband or relatives | Cruelty (physical or mental) to a married woman by her husband or his relatives |
| IPC 306 | Abetment of suicide | Abetting a person to commit suicide |
| IPC 326A / 326B | Acid attack | Voluntarily causing grievous hurt by acid (326A) and throwing or attempting to throw acid (326B) |
| CrPC 174 | Police inquest | Investigation into unnatural/suspicious death; for a married woman's death within 7 years of marriage the inquest is conducted by an Executive Magistrate |
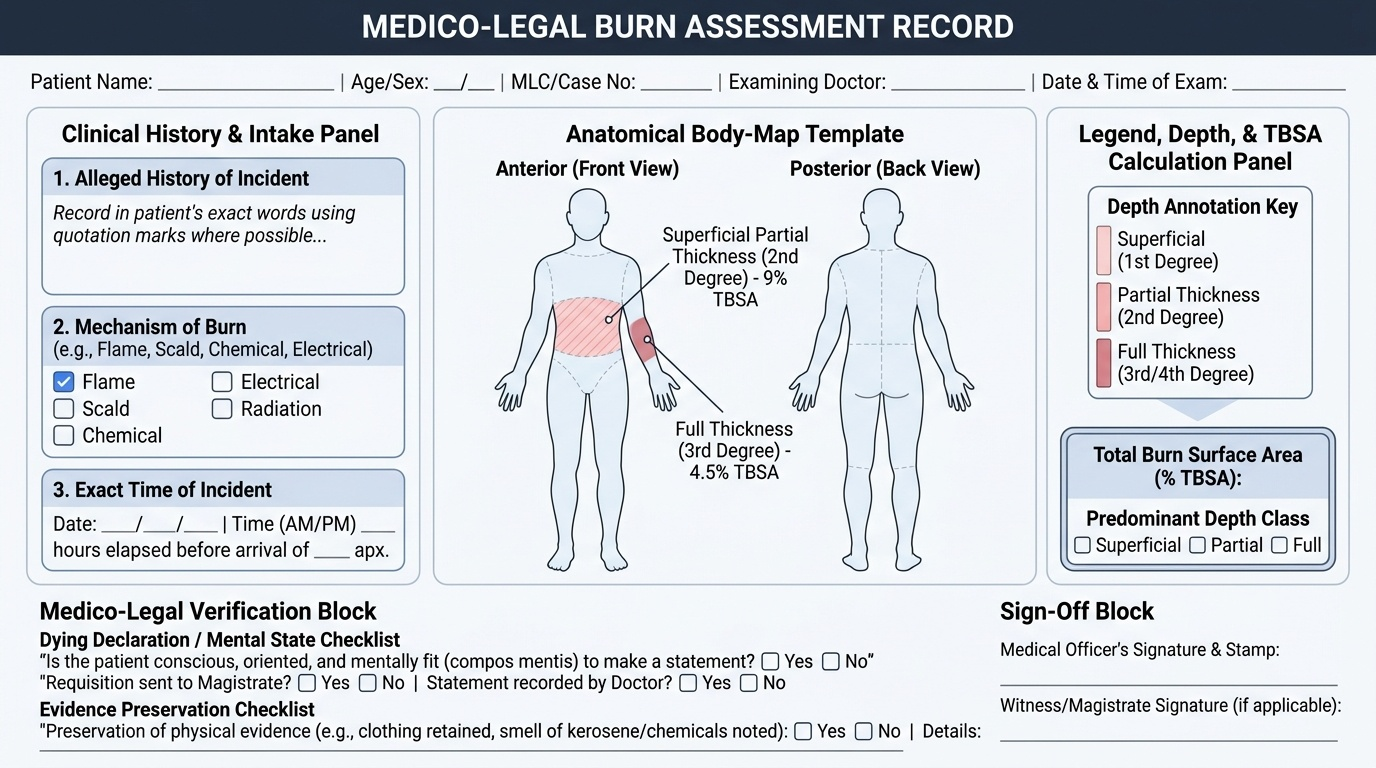
Method: Documentation, the Dying Declaration and Evidence Preservation
The practical method of medico-legal burns care rests on three pillars: meticulous documentation, the dying declaration, and preservation of evidence. Documentation must be contemporaneous, legible, dated and timed, and factual. Record the alleged history in the patient's own words (in quotation marks where possible), the mechanism, the exact time of the burn, and a careful body-map annotating the %TBSA and depth of each region — the very same assessment you make clinically now doubles as legal evidence, so it must be precise. Avoid opinions on culpability; record observations. The second pillar is the dying declaration: a statement made by a person who believes they are about to die concerning the cause and circumstances of their injury, which carries evidentiary value under the law because of the solemn belief in impending death. It is ideally recorded by a Magistrate, but when the patient's condition is critical and waiting would risk losing the statement, a doctor may record it, after first certifying that the patient is conscious and mentally fit (compos mentis) to make it; the declaration is taken in the patient's own words, witnessed, and signed/thumb-marked. The third pillar is preservation of evidence — retaining clothing, noting smell of kerosene or chemicals, and not discarding anything that may be material — and maintaining a clear chain of custody. Done together, these protect the patient, the innocent, and the integrity of any later trial.
Provided image
Practical points when recording a dying declaration:
- Certify and note that the patient is conscious and mentally competent (compos mentis) before starting.
- Record the statement in the patient's own words, asking open questions and avoiding leading them.
- Have it witnessed, and obtain the patient's signature or thumb impression.
- Note the date and time, and that the declaration was made voluntarily; preserve it with the records.
SELF-CHECK
A critically burned woman wishes to state how her burns occurred, but she is deteriorating rapidly and no Magistrate can reach the hospital in time. What is the correct action regarding a dying declaration?
A. Wait for a Magistrate, as only a Magistrate may legally record a dying declaration
B. The treating doctor may record the dying declaration after certifying that the patient is conscious and mentally fit, taking it in her own words and having it witnessed
C. A dying declaration is not valid for burns cases and should not be recorded
D. Ask a family member to write down what she says and sign on her behalf
Reveal Answer
Answer: B. The treating doctor may record the dying declaration after certifying that the patient is conscious and mentally fit, taking it in her own words and having it witnessed
A dying declaration is ideally recorded by a Magistrate, but when the patient's condition is critical and delay would risk losing the statement, the treating doctor may record it. The doctor must first certify the patient is conscious and mentally fit (compos mentis), record the statement in her own words, have it witnessed, and obtain her signature or thumb impression with the date and time.