Page 8 of 20
SU17.4-6 | Head Injury Assessment and Management — SDL Guide (Part 2)
Principles of Management — Resuscitation, Preventing Secondary Injury and Surgery
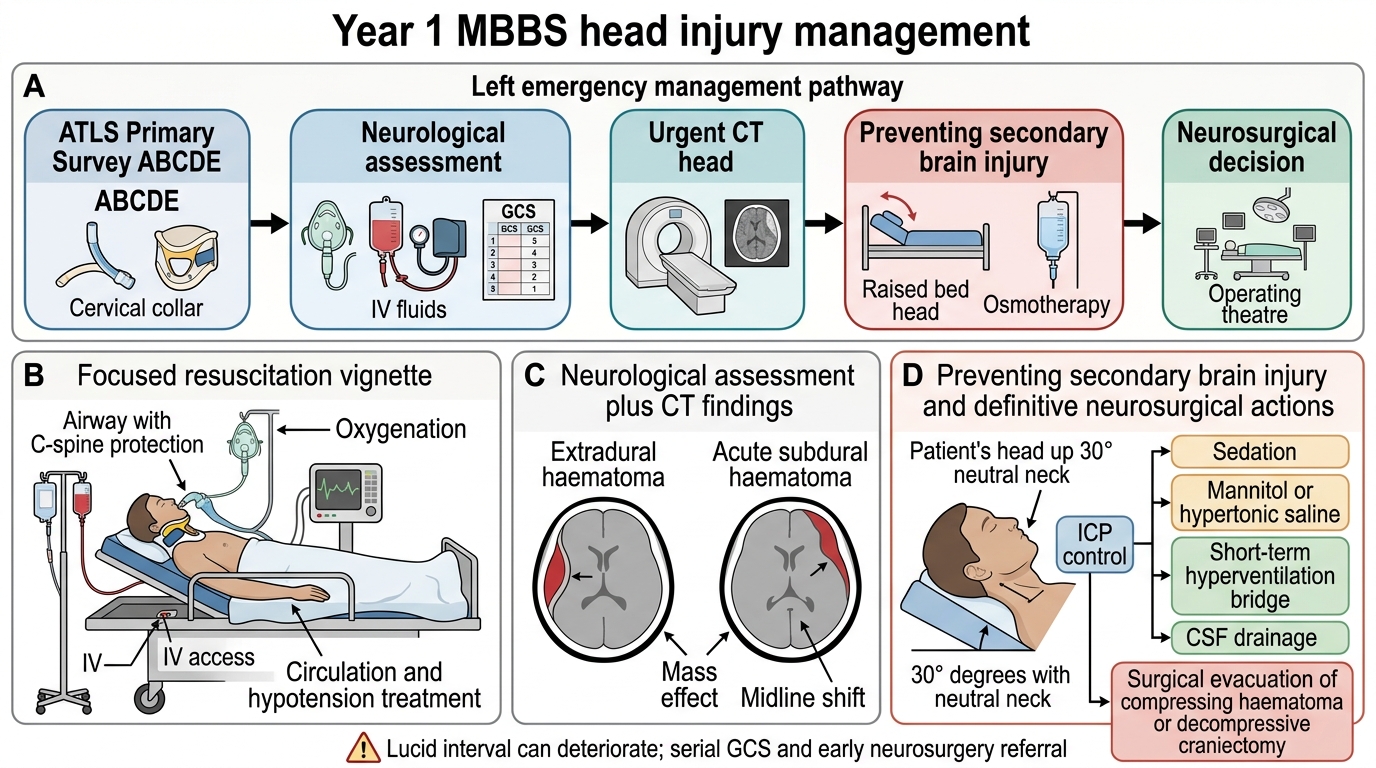
The management of head injury is built on a single overriding aim — prevent secondary brain injury — and it begins not with the brain but with resuscitation, because a hypoxic, hypotensive brain is being damaged every second. Care therefore starts with the ATLS primary survey (ABCDE): secure the Airway with cervical-spine control (intubate if GCS ≤8 or the airway is unsafe), ensure Breathing and oxygenation (avoid both hypoxia and excessive hypocapnia), and restore Circulation by treating hypotension and any bleeding, because a single episode of hypotension markedly worsens outcome. Only once the patient is physiologically stable does Disability (the neurological assessment with GCS and pupils) and Exposure follow, and a NCCT is obtained. The general neuroprotective measures that prevent secondary injury then run continuously: maintain oxygenation and blood pressure (cerebral perfusion), nurse with the head elevated about 30 degrees and the neck neutral to aid venous drainage, treat pain, fever and seizures, avoid hyponatraemia, and control raised ICP. Specific ICP-lowering measures for a deteriorating patient include adequate sedation and analgesia, osmotic therapy with mannitol or hypertonic saline, controlled short-term hyperventilation only as a temporising bridge, and CSF drainage; ICP may be monitored directly in severe injury. Surgery is indicated for a significant mass lesion causing compression — urgent craniotomy and evacuation of an extradural or large acute subdural haematoma is life-saving and time-critical (the talk-and-deteriorate extradural is a neurosurgical emergency), and a decompressive craniectomy may be used for refractory swelling; depressed compound fractures are elevated and debrided. Throughout, the patient is reassessed repeatedly and referred early to neurosurgery, because head injury is a dynamic condition in which timely escalation saves brain.
Head Injury Management Flow Diagram
- Resuscitate first (ABCDE): airway + C-spine (intubate if GCS ≤8), oxygenate, treat hypotension — avoid hypoxia and hypotension above all.
- Prevent secondary injury: head up ~30°, neck neutral, treat fever/seizures/pain, maintain perfusion.
- Control ICP: sedation, osmotherapy (mannitol/hypertonic saline), short-term hyperventilation as a bridge, CSF drainage.
- Surgery: urgent evacuation of a compressing extradural/acute subdural; decompressive craniectomy for refractory swelling; elevate depressed fractures.
- Reassess serially; refer to neurosurgery early.
CLINICAL PEARL
A talking head-injured patient is NOT a safe head-injured patient. The classic extradural haematoma victim is lucid after the impact and deteriorates an hour or two later as the arterial clot expands — the 'lucid interval'. Never discharge or relax monitoring on the basis of an alert presentation alone; it is the serial GCS, not the first GCS, that protects the patient. And remember the Cushing reflex — rising blood pressure with a SLOWING pulse and irregular breathing — is a late, dangerous sign of raised ICP demanding immediate ICP-lowering measures and a neurosurgeon, not a wait-and-see.
Check Your Understanding
Reason back through the motorcyclist from the hook. His lucid arrival followed by drowsiness, an enlarging pupil and a slowing pulse with rising blood pressure is the textbook talk-and-deteriorate course of an extradural haematoma — an arterial bleed from the middle meningeal artery, biconvex on CT — now raising intracranial pressure and triggering the Cushing reflex and uncal herniation (the dilated pupil marks the side of the clot). The damage he is sustaining now is secondary and therefore preventable, which is exactly why management would have started with ABCDE resuscitation (airway with C-spine control, oxygenation, blood-pressure support), a serially repeated GCS, and an urgent NCCT that would show the clot. His treatment is emergency craniotomy and evacuation plus measures to lower ICP, and the lesson is that serial assessment, not the reassuring first look, is what saves him. Self-test on four links: can you distinguish primary from secondary brain injury and name the four intracranial haematomas with their CT shapes and bleeding sources; can you score a GCS from its three components and state the severity bands and the ≤8 intubation threshold; can you state the first-line investigation; and can you outline management from ABCDE through secondary-injury prevention to surgical evacuation? The questions in this module check exactly these.
SELF-CHECK
In a head-injured patient, what is the single most important principle that governs ongoing management?
A. Give prophylactic antibiotics to every patient
B. Prevent secondary brain injury by avoiding hypoxia and hypotension and controlling raised ICP
C. Operate on every head injury regardless of CT findings
D. Keep the patient flat and avoid all sedation
Reveal Answer
Answer: B. Prevent secondary brain injury by avoiding hypoxia and hypotension and controlling raised ICP
Primary injury (at impact) is largely irreversible, so management focuses on preventing SECONDARY brain injury — chiefly by avoiding hypoxia and hypotension, maintaining cerebral perfusion, and controlling raised intracranial pressure. Resuscitation (ABCDE) precedes neurological assessment, and surgery is reserved for compressing mass lesions.