Page 11 of 20
SU17.7 | Soft Tissue Injury Assessment and Management — SDL Guide (Part 2)
Principles of Management — Cleaning, Closure, Tetanus and Antibiotics
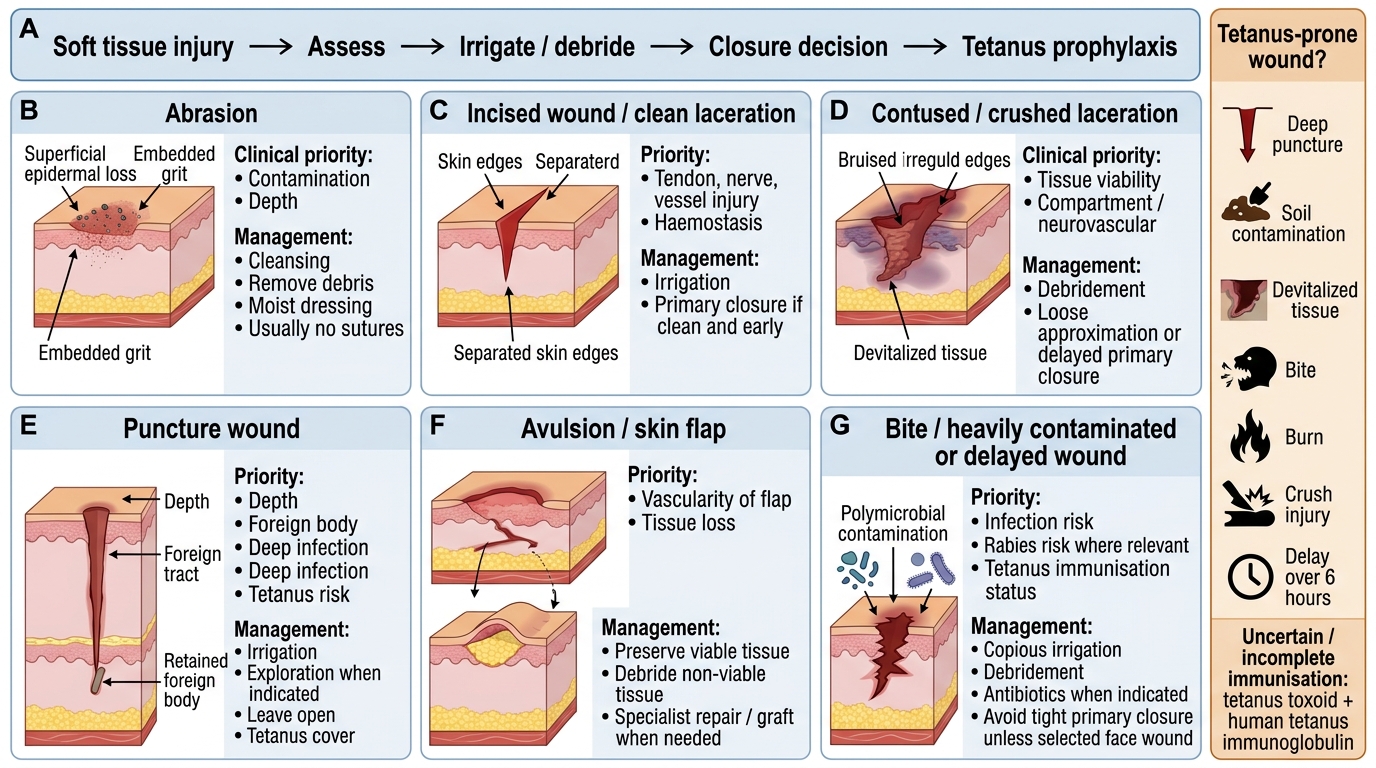
Management of a soft-tissue wound follows a logical order that protects life, limb and function while preventing infection. First control bleeding by direct pressure and elevation, then provide analgesia. The cornerstone of wound care is thorough cleaning and debridement: irrigate copiously with saline to wash out dirt and bacteria, remove foreign material, and excise clearly devitalised (dead) tissue, since dead, contaminated tissue is the seedbed of infection (including tetanus and gas gangrene). The decision on closure then depends on the wound. Primary closure (suturing the edges at once) suits a clean, recent wound with minimal contamination and viable edges. A heavily contaminated or older wound, or one with tissue loss or infection risk, is better managed by delayed primary closure (clean now, close after a few days once it is clean) or secondary closure (left open to heal by granulation, or later grafted) — closing a dirty wound primarily traps infection. Tetanus prophylaxis is mandatory and must never be forgotten: assess whether the wound is tetanus-prone (contaminated with soil/faeces, devitalised tissue, deep puncture, delay over 6 hours, bites or burns) and combine this with the patient's immunisation history — a fully immunised patient with a clean minor wound may need nothing, while an incompletely immunised patient with a tetanus-prone wound needs both the tetanus toxoid vaccine and human tetanus immunoglobulin. Antibiotics are not needed for every wound but are indicated for contaminated wounds, bites, deep or devitalised wounds, and established infection (bites in particular need cover against their mixed flora). For closed soft-tissue injuries such as sprains, strains and contusions, first-line management is RICE — Rest, Ice, Compression and Elevation — with analgesia, which limits swelling and pain. Finally, give clear wound-care and follow-up advice, arrange suture removal, and refer wounds with deep-structure injury to the appropriate specialist.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
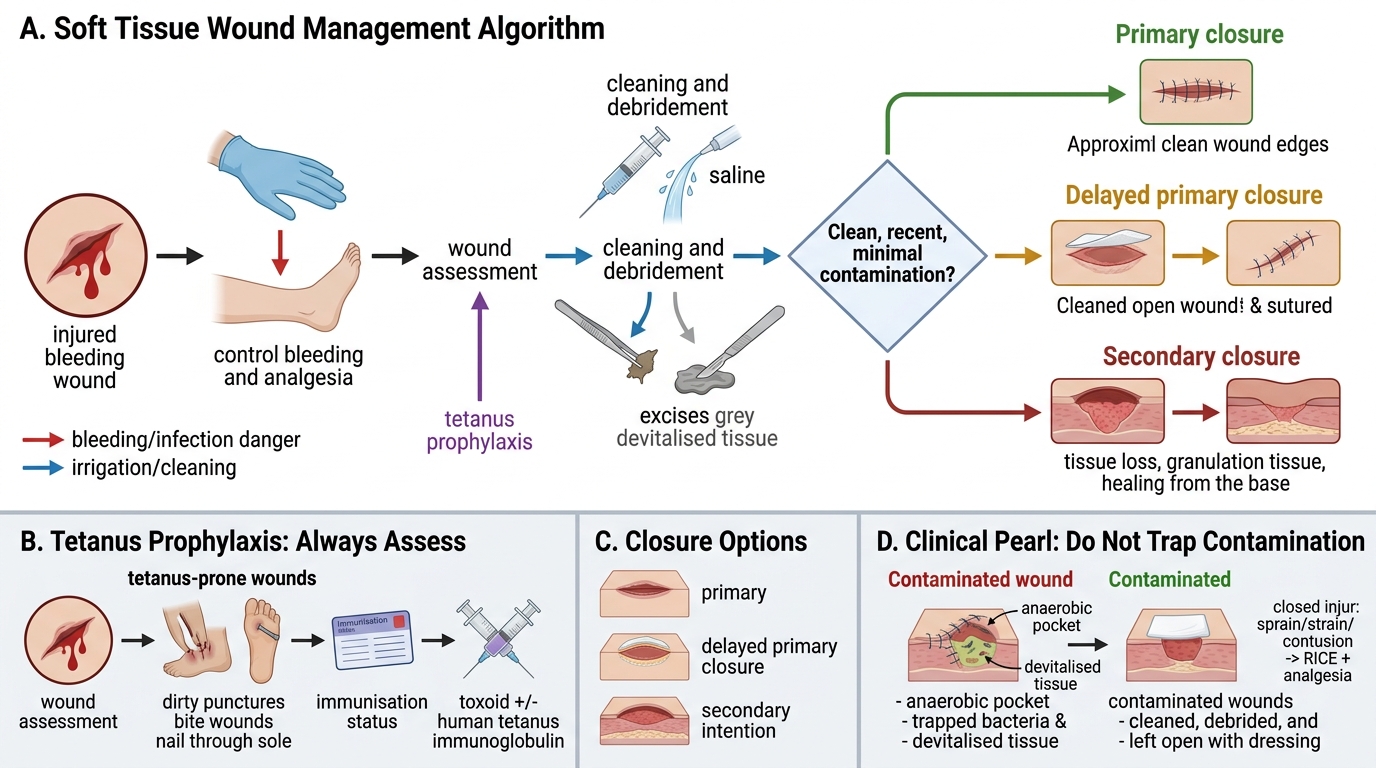
Soft Tissue Wound Management Flowchart
- Control bleeding (pressure, elevation) + analgesia.
- Clean and debride: copious saline irrigation, remove foreign material, excise devitalised tissue.
- Closure: primary (clean, recent, minimal contamination); delayed primary/secondary (contaminated, old, tissue loss).
- Tetanus prophylaxis (always assess): tetanus-prone wound + immunisation status → toxoid ± human tetanus immunoglobulin.
- Antibiotics: for contaminated/bite/deep/devitalised wounds and established infection.
- Closed injuries (sprain/strain/contusion): RICE + analgesia.
CLINICAL PEARL
Never close a contaminated wound primarily, and never close a wound without checking tetanus status. A dirty wound stitched up tight traps bacteria and devitalised tissue in an anaerobic pocket — the ideal home for tetanus and gas gangrene — so contaminated or old wounds are cleaned, debrided and left for delayed primary or secondary closure. And the apparently trivial wound — a nail through the sole, a dirty puncture, a bite — is exactly the tetanus-prone wound that kills if prophylaxis is skipped: every wound assessment must end with the question 'what does this patient need for tetanus?'.
Check Your Understanding
Return to the farmer with the forearm wound from the hook and reason through it as a complete case. First classify it: a clean-edged cut from a sharp blade is an incised wound, but because the blade came from soil it is contaminated, which changes the plan. Your assessment must go beyond the skin: examine the distal circulation, nerve sensation and power, and tendon function, because the wound overlies the structures that move and feel his hand — a partially divided flexor tendon could still allow some movement, so you test each one specifically, and you take an X-ray if a metal fragment or underlying fracture is suspected. Management then follows the order: control bleeding, give analgesia, clean and debride the contaminated wound thoroughly, and — because it is contaminated and possibly delayed — favour delayed primary closure rather than tight primary suturing; give antibiotics for the contamination and, above all, assess and provide tetanus prophylaxis based on the tetanus-prone wound plus his immunisation status, adding human tetanus immunoglobulin if he is incompletely immunised. Self-test on four links: can you classify open and closed soft-tissue injuries by mechanism and edges; can you assess a wound including the deep structures and choose targeted investigations; can you decide between primary, delayed primary and secondary closure; and can you state the indications for tetanus prophylaxis and antibiotics, and the RICE treatment of closed injuries? The questions in this module check exactly these.
Soft Tissue Injury Assessment and Management Summary
SELF-CHECK
A patient presents 8 hours after a deep puncture wound contaminated with soil and is uncertain about previous immunisation. What must the management definitely include?
A. Immediate tight primary closure of the wound
B. Reassurance only, as puncture wounds are trivial
C. Wound cleaning/debridement plus tetanus prophylaxis (toxoid and tetanus immunoglobulin)
D. Antibiotics alone, with no need for tetanus cover
Reveal Answer
Answer: C. Wound cleaning/debridement plus tetanus prophylaxis (toxoid and tetanus immunoglobulin)
This is a tetanus-prone wound (deep puncture, soil contamination, delay over 6 hours) in an incompletely/uncertainly immunised patient, so management must include thorough cleaning/debridement and BOTH tetanus toxoid and human tetanus immunoglobulin. A contaminated deep wound should NOT be closed primarily; antibiotics are given but do not replace tetanus prophylaxis.