Page 1 of 14
SU18.1 | Cutaneous and Subcutaneous Infections — SDL Guide
Learning Objectives
- Describe the pathogenesis, causative organisms and classification of common cutaneous and subcutaneous infections (SU18.1).
- Distinguish clinically between cellulitis and an abscess, and recognise the special features of furuncle, carbuncle and necrotizing fasciitis (SU18.1).
- Outline the management of skin and soft-tissue infections, including when antibiotics suffice and when surgical drainage or debridement is mandatory (SU18.1).
INSTRUCTIONS
Infections of the skin and the tissue beneath it are among the commonest reasons a patient presents to a surgical clinic or emergency room. Most are everyday problems — a boil, a patch of cellulitis — that resolve with simple measures, but a small number are surgical emergencies in which delay costs a limb or a life. The single most useful skill this module builds is the ability to decide, at the bedside, whether you are looking at spreading infection that needs antibiotics, a collection of pus that needs the knife, or a necrotizing infection that needs the operating theatre now.
References
- Bailey & Love's Short Practice of Surgery, Surgical Infection (textbook)
- SRB's Manual of Surgery, Wound, Sinus, Fistula and Soft Tissue Infections (textbook)
- Sabiston Textbook of Surgery, Surgical Infections (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients sit in your evening clinic. The first is a young man with a single, tender, red lump on the back of his neck that has come to a yellow head — painful, but he is otherwise well. The second is a woman whose lower leg is hot, red and swollen over a hand's breadth, with a temperature of 38.5°C, but with no discrete lump to feel. The third is a diabetic man whose perineal pain seemed trivial yesterday and who now looks grey and unwell, with skin that is dusky, blistering and crackles under your fingers. All three have a 'skin infection', yet one needs a small incision, one needs antibiotics and rest, and one needs an emergency call to theatre. Telling them apart, quickly and correctly, is the whole point of this module.
WHY THIS MATTERS
Skin and soft-tissue infections are everyday surgical work and a frequent examination topic, but their importance lies in a single decisive distinction: is there pus, and is the infection spreading dangerously? Getting this wrong in either direction harms patients — incising a simple cellulitis achieves nothing and seeds infection, while treating an abscess with antibiotics alone lets the pus persist and the patient deteriorate. At the extreme, mistaking early necrotizing fasciitis for ordinary cellulitis is a lethal error, because that condition kills unless it is surgically debrided within hours. For a final-year student about to take responsibility in the ward and emergency room, the ability to recognise pus (fluctuance → drain it), recognise spread (cellulitis → antibiotics), and recognise the emergency (necrotizing infection → theatre) is core, transferable and frequently tested.
RECALL
Recall some foundations before we build on them. From anatomy: the skin has an outer epidermis, a vascular dermis carrying hair follicles and sweat glands, and beneath it the subcutaneous (subcutis) fat, which sits on the tough deep fascia; infections are described and classified by how deep they reach. From microbiology: the two organisms that cause most of these infections are Staphylococcus aureus, which tends to localise and form pus (abscesses, boils, carbuncles), and Streptococcus pyogenes (group A streptococcus), which tends to spread through tissue planes and lymphatics causing cellulitis and erysipelas. From pathology, recall that suppuration is the formation of pus — dead neutrophils, bacteria and liquefied tissue — and that a walled-off collection of pus is an abscess, which the body cannot clear without drainage.
The Patient with a Red, Painful Skin Lesion
Cutaneous and subcutaneous infections present along a spectrum from the trivial to the life-threatening, and the history and first look already begin to place a patient on that spectrum. The mildest is folliculitis, inflammation of hair follicles producing small pustules. A furuncle (boil) is a deeper infection of a single hair follicle and its surrounding tissue, presenting as a tender red nodule that points and discharges pus. A carbuncle is a more serious, coalescent infection of several adjacent follicles forming an indurated slough-filled mass with multiple discharging openings; it characteristically affects the nape of the neck or back and is strongly associated with diabetes mellitus, so every carbuncle should prompt a blood-sugar check. Cellulitis presents as a spreading area of hot, red, swollen, tender skin with an ill-defined edge, often with fever and malaise, and no discrete lump or pus to feel. An abscess presents as a localised, tense, tender swelling that becomes fluctuant as pus accumulates. The most dangerous presentation is necrotizing fasciitis: pain that is severe and out of proportion to the visible signs, rapidly spreading dusky or blistering skin, crepitus, and a systemically unwell, toxic patient. The history should always seek a portal of entry (a cut, bite, ulcer or injection site), the speed of progression, and risk factors such as diabetes, immunosuppression or peripheral vascular disease.
Pathogenesis and Classification of Skin and Soft-Tissue Infections
Skin and soft-tissue infection begins when organisms breach the protective epidermis — through a cut, bite, follicle, ulcer or surgical wound — and establish themselves in tissue whose defences are overwhelmed by the dose, the virulence of the organism, or impaired host resistance such as diabetes or ischaemia. The pattern of infection that follows is best understood by depth and by whether it forms localised pus (suppurative) or spreads diffusely (non-suppurative), and this is the basis of a simple, clinically useful classification. Folliculitis, furuncle and carbuncle are follicle-centred staphylococcal infections of increasing depth and severity. Cellulitis is a non-suppurative spreading infection of the dermis and subcutaneous tissue, usually streptococcal, while erysipelas is a more superficial, sharply demarcated, raised streptococcal infection of the upper dermis with lymphatic involvement. An abscess is a walled-off collection of pus that, once formed, the immune system and antibiotics alone cannot clear. At the far end lies necrotizing fasciitis, a rapidly advancing necrosis of the subcutaneous tissue and deep fascia, often polymicrobial or caused by group A streptococcus, in which thrombosis of small vessels causes the overlying skin to die — Fournier's gangrene is the form affecting the perineum and scrotum.
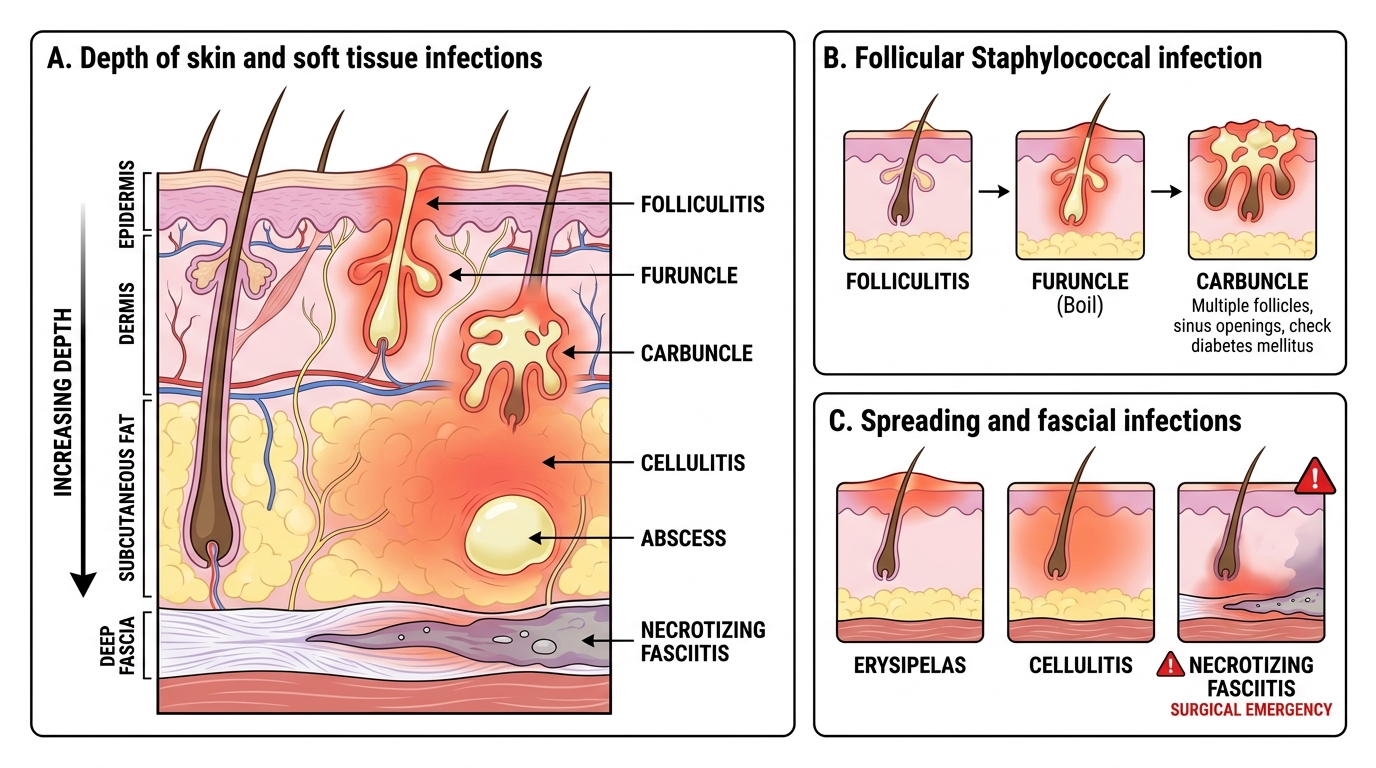
Depth of Common Skin and Soft Tissue Infections
- Follicular (Staph aureus): folliculitis → furuncle (boil) → carbuncle (diabetics, nape of neck).
- Spreading non-suppurative (Strep pyogenes): cellulitis (deep, ill-defined) and erysipelas (superficial, sharply demarcated).
- Suppurative collection: abscess — localised, walled-off pus.
- Necrotizing emergency: necrotizing fasciitis (polymicrobial / group A strep), Fournier's gangrene = perineal variant.
SELF-CHECK
A 55-year-old man presents with a painful, indurated swelling on the nape of his neck discharging pus through several openings. Which underlying condition should be actively excluded?
A. Hypertension
B. Diabetes mellitus
C. Hypothyroidism
D. Iron-deficiency anaemia
Reveal Answer
Answer: B. Diabetes mellitus
This describes a carbuncle — a coalescent infection of several adjacent hair follicles, typically on the nape of the neck or back, caused by Staphylococcus aureus. Carbuncles are strongly associated with diabetes mellitus, so blood glucose must always be checked; uncontrolled diabetes both predisposes to and impairs healing of the lesion.
Clinical Assessment and Investigation
The bedside assessment is built to answer the three decisive questions: is there pus, is the infection spreading, and is the patient systemically unwell. Inspect the lesion for the area and margin of redness (mark its edge with a pen so spread can be tracked), for any blistering, dusky discolouration or skin necrosis, and for a portal of entry. Palpate for warmth, tenderness and — crucially — for fluctuance, the sign of a fluid (pus) collection that tells you an abscess is present and must be drained; cellulitis, by contrast, feels diffusely firm and tender with no fluctuant point. Feel for crepitus (gas in the tissues) and elicit whether pain is grossly out of proportion to the signs, because both point to a necrotizing infection. Always examine the regional lymph nodes and look for red streaks of lymphangitis tracking towards them. Assess the whole patient for fever, tachycardia, hypotension and confusion — the markers of sepsis. Most simple cellulitis and small abscesses need no investigation, but in the unwell or diabetic patient check blood glucose, full blood count, CRP and renal function, take blood cultures and a pus swab/culture when drained, and where a necrotizing infection is suspected proceed to urgent surgical exploration rather than waiting for imaging — the diagnosis is clinical and operative, and delay for tests is dangerous.
Provided image
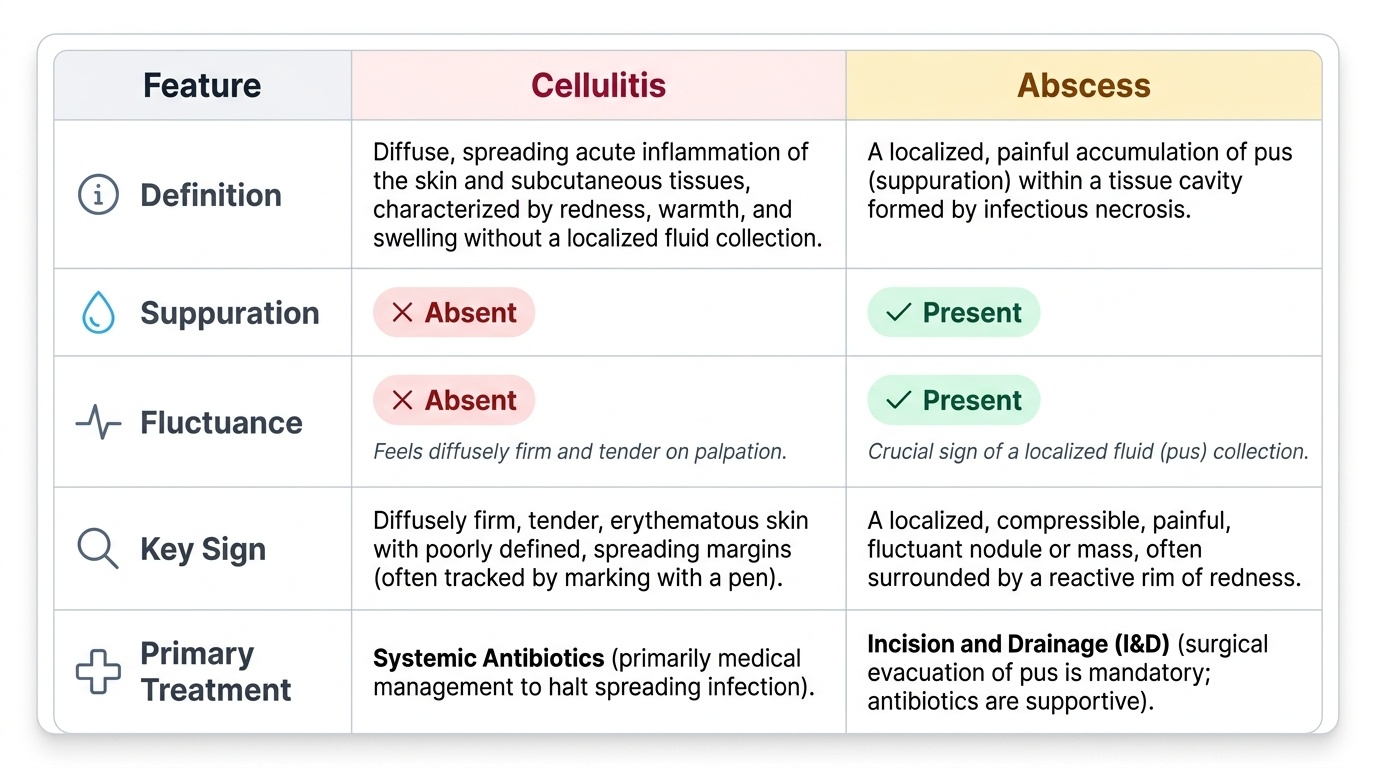
| Feature | Cellulitis | Abscess |
|---|---|---|
| Definition | Spreading non-suppurative infection of dermis/subcutis | Localised walled-off collection of pus |
| Usual organism | Streptococcus pyogenes | Staphylococcus aureus |
| Pus present | No | Yes |
| Fluctuance | Absent (diffusely firm) | Present |
| Primary treatment | Antibiotics + elevation | Incision and drainage |