Page 8 of 14
SU18.3 | Surgical Swelling Examination — SDL Guide (Part 2)
Interpreting the Findings and Forming a Differential
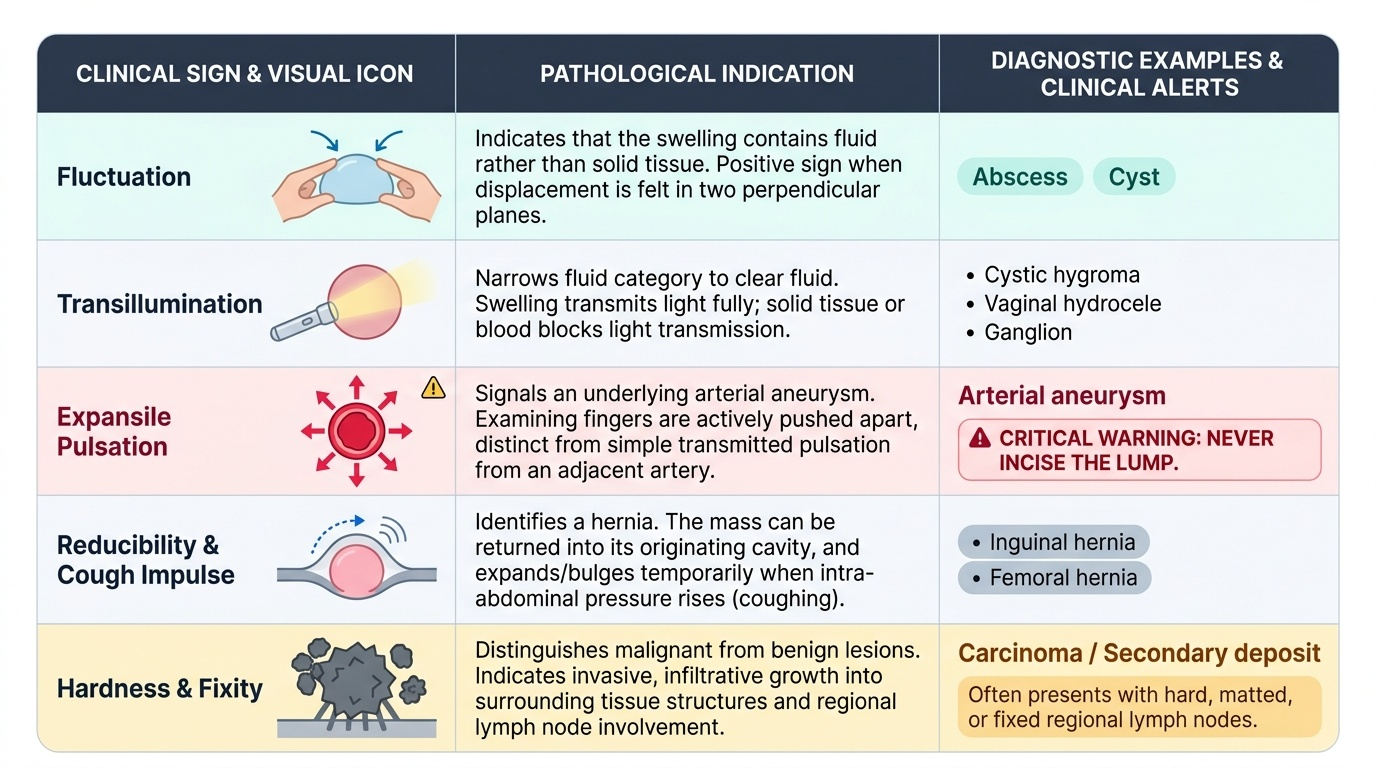
Each special sign points towards a particular tissue or pathology, and interpreting them together converts the description into a differential diagnosis. Fluctuation indicates that the swelling contains fluid — pus in an abscess, or fluid in a cyst — and a positive sign (in two planes) tells you the lump is not solid. Transillumination narrows fluid further: a swelling that transilluminates contains clear fluid (a cystic hygroma, a vaginal hydrocele, a ganglion), whereas blood or solid tissue does not transmit light. Expansile pulsation — the examining fingers pushed apart in all directions — signals an aneurysm and is a warning never to incise the lump, whereas a swelling that merely lifts (transmitted pulsation) is lying over an artery. Reducibility with a cough impulse over a hernial orifice identifies a hernia. Consistency and fixity distinguish the benign from the sinister: a soft, mobile, well-defined lump is usually benign (lipoma, cyst), whereas a hard, irregular, fixed swelling with hard or matted regional nodes suggests malignancy. The pathological sieve from earlier — congenital, traumatic, inflammatory, neoplastic — is now applied to the gathered signs to produce a short, ranked differential. A lump that is warm, tender and fluctuant is most likely an abscess; a soft, mobile, subcutaneous, non-tender lump with a slip sign is a lipoma; a hard, fixed lump with matted nodes is likely malignant; and a soft, reducible groin lump with a cough impulse is a hernia.
Provided image
| Sign | What it indicates | Example diagnosis |
|---|---|---|
| Fluctuation | Fluid within the swelling | Abscess, cyst |
| Transillumination | Clear fluid | Cystic hygroma, hydrocele, ganglion |
| Expansile pulsation | Aneurysm (do NOT incise) | Arterial aneurysm |
| Reducibility + cough impulse | Hernia | Inguinal/femoral hernia |
| Hard, fixed + matted nodes | Malignancy | Carcinoma, secondary deposit |
Applying the Examination and Ordering Investigations
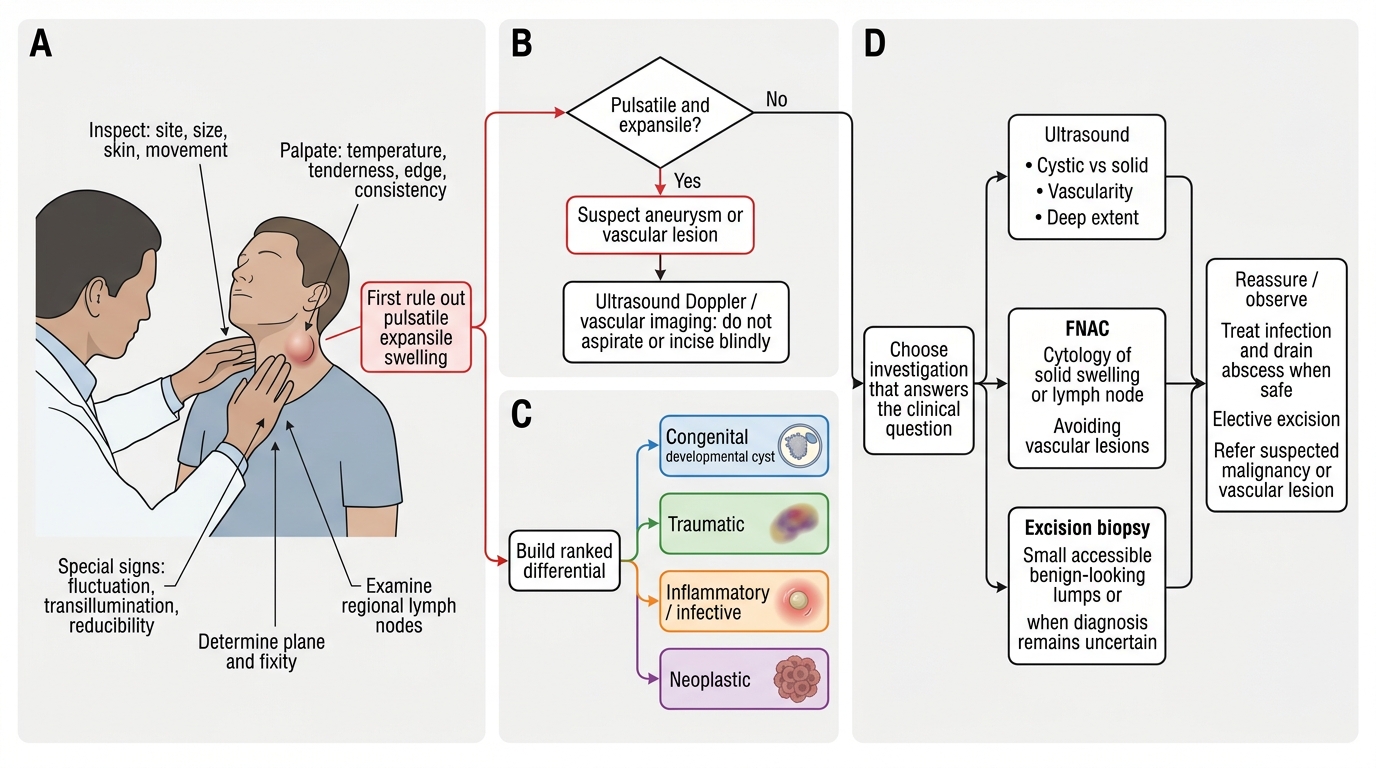
In supervised clinical practice the examination is used to drive a rational, stepwise plan, and the principle is that investigations follow the clinical examination, not replace it. Having described the swelling and formed a differential, you select investigations that answer the specific clinical question. Ultrasound is the usual first-line imaging for a soft-tissue lump or a neck swelling, distinguishing solid from cystic and characterising the regional nodes without radiation, and is the guide for needle procedures. Fine-needle aspiration cytology (FNAC) samples a solid lump or an enlarged node to look for malignant or infective cells, while core or excision biopsy is used when histological architecture is needed (and a clinically suspicious lump or pigmented lesion is removed by excision biopsy). Cross-sectional imaging (CT/MRI) is reserved for deep, large or potentially malignant swellings to define extent and stage. Crucially, the examination itself dictates safe choices: a swelling that shows expansile pulsation is investigated as a possible aneurysm with imaging and is never aspirated or incised, and a swelling that is in fact a hernia is managed as such rather than biopsied. The treatment plan then flows from the working diagnosis — reassurance or simple excision for a benign cyst or lipoma; incision and drainage for an abscess; referral and staged oncological management for a suspected malignancy; and surgical repair for a hernia. Under supervision, the student presents the swelling in the conventional vocabulary, states a ranked differential, and proposes the next investigation and an outline treatment plan.
Work-up of a Swelling: Examination to Management
CLINICAL PEARL
Two habits make a swelling examination safe and complete. First, always examine the regional lymph nodes — they are part of the examination of every swelling, not an optional extra, and matted or hard nodes may be the only clue that an apparently localised lump is malignant or infective. Second, before you ever consider aspirating or incising a swelling, prove it is not pulsatile and expansile — an aneurysm transmits an expansile pulsation in all directions, and incising or aspirating it can be catastrophic. A pulsatile groin or limb swelling is imaged, never needled blindly.
Check Your Understanding
Consolidate the skill by walking the whole sequence on the neck lump from the hook. Inspect it — site against landmarks, size measured, surface, overlying skin, and any movement on swallowing. Palpate systematically — temperature, tenderness, edge, consistency — then test the special signs: is it fluctuant (fluid), does it transilluminate (clear fluid, e.g. a cystic hygroma), is it pulsatile and expansile (do not incise), is it reducible with a cough impulse? Determine its plane and fixity, then examine the cervical lymph nodes and complete a relevant general examination. From the gathered signs build a ranked differential using the congenital/traumatic/inflammatory/neoplastic sieve, then choose the investigation that answers your question — ultrasound first, then FNAC or excision biopsy as indicated — and outline a treatment plan. Self-test on five links: can you list the inspection and palpation sequence in order; can you elicit and interpret fluctuation and transillumination; can you recognise the expansile pulsation that forbids incision; can you explain why the regional nodes are always examined; and can you move from clinical findings to a rational investigation and treatment plan? The questions below check exactly these.
SELF-CHECK
A patient has a soft, non-tender swelling in the neck that glows red when a torch is held against it in a darkened room. Which special sign is positive, and what does it indicate?
A. Fluctuation, indicating a solid tumour
B. Transillumination, indicating clear fluid
C. Expansile pulsation, indicating an aneurysm
D. Cough impulse, indicating a hernia
Reveal Answer
Answer: B. Transillumination, indicating clear fluid
A swelling that transmits light (glows red) when transilluminated contains clear fluid — for example a cystic hygroma in the neck, a hydrocele in the scrotum, or a ganglion. Solid tissue, blood and pus do not transilluminate. Transillumination therefore narrows a fluctuant (fluid-containing) swelling specifically to one filled with clear fluid.