Page 2 of 14
SU19.1-2 | Cleft Lip and Palate — SDL Guide (Part 2)
Principles of Reconstruction
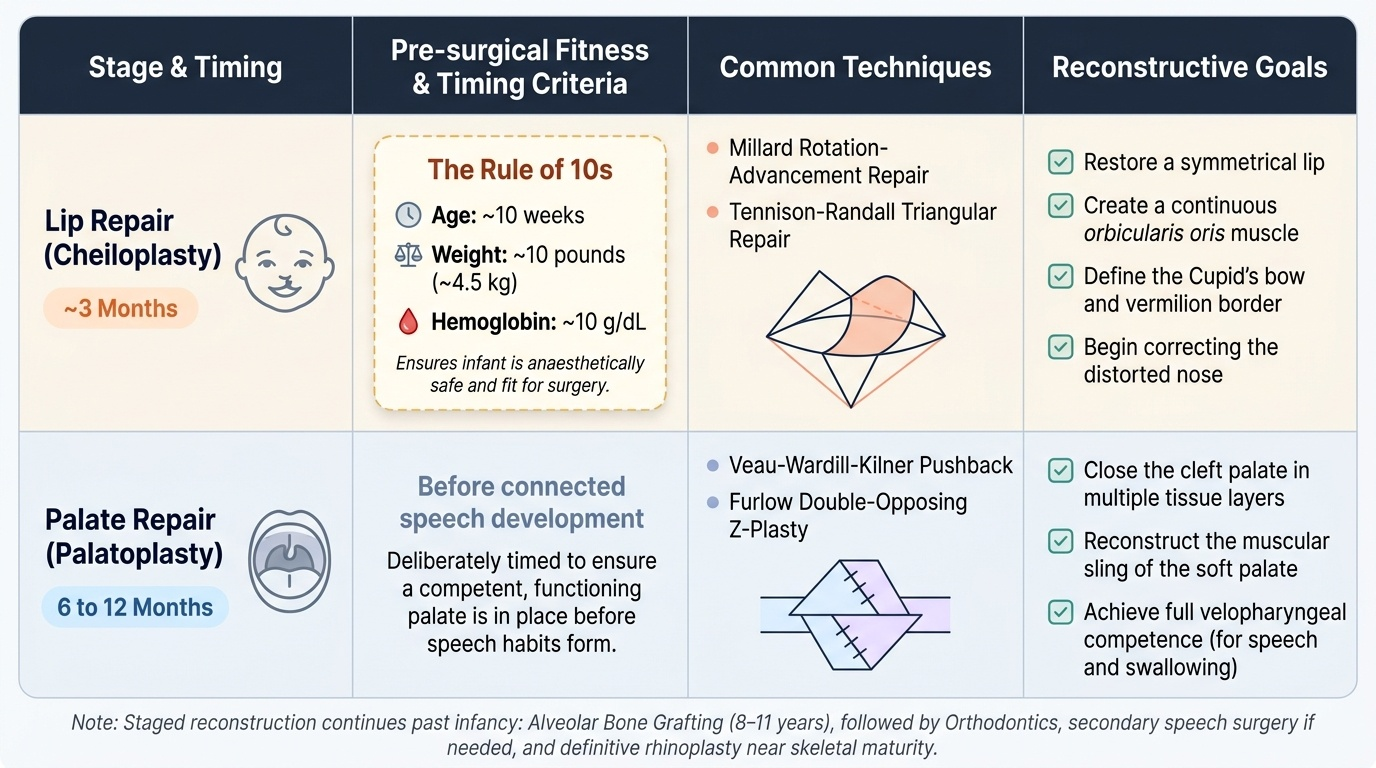
The reconstruction of cleft lip and palate is staged and follows a biological timetable, with two overriding principles: operate when the child is fit, and operate in time to allow normal function — appearance and bonding for the lip, and speech development for the palate. Fitness for the first operation, the lip repair, is classically summarised by the rule of 10s: the child should be about 10 weeks of age, weigh about 10 pounds (around 4.5 kg) and have a haemoglobin of about 10 g/dL before lip surgery, a simple shorthand that ensures the infant has grown, is anaesthetically safe and can tolerate the operation. The cleft lip is therefore repaired at around 3 months of age; the goal is to restore a symmetrical lip with a continuous orbicularis oris muscle, a well-defined cupid's bow and vermilion, and to begin correcting the distorted nose, using techniques such as the Millard rotation-advancement repair or the Tennison-Randall triangular repair. The cleft palate is repaired later, at around 6 to 12 months of age, deliberately timed before the child develops connected speech so that a competent palate is in place for normal speech to form; palatoplasty techniques (for example the Veau-Wardill-Kilner pushback or a Furlow double-opposing Z-plasty) close the cleft in layers and, crucially, reconstruct the muscular sling of the soft palate to achieve velopharyngeal competence. Reconstruction does not end there: alveolar bone grafting is performed in the mixed-dentition years (around 8 to 11 years) to provide bone for the erupting teeth, and some children later need secondary speech surgery (such as a pharyngoplasty) for persistent velopharyngeal incompetence, orthodontic treatment, and definitive rhinoplasty or lip revision near skeletal maturity. Throughout, the surgeon must counsel the family that early complications of repair include bleeding, infection and wound breakdown, and that the palate repair specifically risks an oronasal fistula and that residual speech and hearing problems may need ongoing care.
Provided image
| Stage | Timing | Technique (examples) | Goal |
|---|---|---|---|
| Lip repair (cheiloplasty) | ~3 months (rule of 10s: 10 weeks, 10 lb, Hb 10 g/dL) | Millard rotation-advancement; Tennison-Randall | Symmetrical lip, continuous orbicularis oris, cupid's bow; begin nasal correction |
| Palate repair (palatoplasty) | ~6-12 months (before connected speech) | Veau-Wardill-Kilner pushback; Furlow Z-plasty | Layered closure, reconstruct soft-palate muscle sling for velopharyngeal competence and speech |
| Alveolar bone graft | ~8-11 years (mixed dentition) | Cancellous bone graft to alveolar cleft | Bone for erupting teeth, arch continuity |
| Secondary procedures | Later childhood to skeletal maturity | Pharyngoplasty, orthodontics, rhinoplasty/lip revision | Correct residual speech, dental and nasal/lip deformity |
CLINICAL PEARL
Remember the timetable through its purpose, not just the numbers: the lip is repaired early (around 3 months, when the child satisfies the rule of 10s — ~10 weeks, ~10 lb, Hb ~10 g/dL) because the family needs a normal-looking lip for bonding, and the palate is repaired later (around 6-12 months) but deliberately BEFORE the child starts to form connected speech, because the whole point of palate repair is to build a competent palate in time for normal speech to develop. If you ever invert the order or repair the palate too late, you accept the lifelong speech penalty that the entire timetable is designed to prevent.
Check Your Understanding
Bring the threads together by returning to the two families in the hook. The newborn boy with the visible gap in the lip extending into the nostril has a unilateral complete cleft lip; the immediate task is not surgery but securing safe feeding with cleft teats so he gains weight, and then, once he satisfies the rule of 10s at around 10 weeks, repairing the lip at about 3 months to restore the orbicularis sling, the cupid's bow and the nose. The three-year-old girl whose palate was repaired but who now has unclear speech and recurrent ear infections shows you the two long-term consequences of a palatal cleft — velopharyngeal incompetence affecting speech, and Eustachian-tube dysfunction causing otitis media — and reminds you that cleft care is a years-long multidisciplinary process, not a single operation. Use these to self-test the two competencies this module covers. First, can you describe the embryology of the cleft and classify any given cleft by site, laterality and completeness, using the incisive foramen to separate primary from secondary palate, and distinguish non-syndromic from syndromic aetiology? Second, can you state the principles of reconstruction — the rule of 10s, lip repair at ~3 months, palate repair at ~6-12 months before speech, then alveolar bone grafting and secondary procedures — and explain WHY each is timed as it is? The questions that follow check exactly these links.
SELF-CHECK
By the rule of 10s, at approximately what age is primary cleft lip repair usually performed, and why is cleft palate repair timed later?
A. At birth; palate repair is delayed only for anaesthetic safety
B. At about 3 months (10 weeks, 10 lb, Hb 10 g/dL); palate is repaired at ~6-12 months, before connected speech develops
C. At 2 years; palate is repaired first to allow feeding
D. At 5 years; palate repair waits until permanent dentition
Reveal Answer
Answer: B. At about 3 months (10 weeks, 10 lb, Hb 10 g/dL); palate is repaired at ~6-12 months, before connected speech develops
The rule of 10s (≈10 weeks of age, ≈10 lb / 4.5 kg, haemoglobin ≈10 g/dL) governs fitness for LIP repair at around 3 months. Palate repair is deliberately timed at about 6-12 months — later than the lip but before the child develops connected speech, so that a competent palate is in place for normal speech to form.