Page 7 of 14
SU21.1-2 | Disorders of Salivary Glands — SDL Guide
Learning Objectives
- Describe the surgical anatomy of the salivary glands and the pathology and clinical presentation of their disorders (SU21.1).
- Enumerate the appropriate investigations and describe the principles of treatment of disorders of the salivary glands (SU21.2).
INSTRUCTIONS
The salivary glands produce some of the commonest surgical swellings of the face and neck, and they sit in one of the most unforgiving pieces of surgical anatomy: the facial nerve runs straight through the parotid gland. The central clinical task is to read a salivary swelling correctly — to tell an obstructing stone from an inflamed gland from a tumour — and then to treat it without sacrificing the nerve that gives a person their smile. This module connects the surgical anatomy of the glands, especially the facial nerve and the salivary ducts, to the pathology and presentation of inflammatory, obstructive and neoplastic disorders and to their investigation and surgical management.
References
- Bailey & Love's Short Practice of Surgery, The Salivary Glands (textbook)
- SRB's Manual of Surgery, Salivary Glands (textbook)
- Sabiston Textbook of Surgery, Head and Neck — Salivary Glands (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients with swellings around the jaw are waiting to be seen, and the same anatomical region tells three completely different stories. The first is a 45-year-old woman with a slowly growing, painless, rubbery lump in front of and below her ear that she has noticed for two years and that has never troubled her. The second is a 30-year-old man whose submandibular swelling balloons up and aches every time he sits down to a meal, then subsides afterwards. The third is an elderly, dehydrated man recovering from abdominal surgery who has developed a hot, tender, rapidly swelling gland over his cheek. A painless lump, a swelling that comes with meals, and an acutely inflamed gland — neoplasm, obstruction and infection — and behind the first of them, threaded straight through the parotid, lies the facial nerve, the single structure that makes salivary surgery as much about what you preserve as what you remove. Learning to read these swellings, and to operate around that nerve, is the heart of salivary surgery.
WHY THIS MATTERS
Salivary gland disorders are common, span the whole spectrum from trivial to malignant, and are a favourite of clinical examinations because they test anatomy, pathology and operative judgement together. They matter for several reasons. The glands produce frequent, visible swellings of the face and neck that patients and clinicians notice, and the diagnostic challenge — distinguishing an obstructing stone from inflammation from a tumour, and a benign tumour from a malignant one — is a genuine clinical skill. Surgically, the parotid is dominated by the facial nerve, which runs through the gland and is the structure most at risk during parotid surgery; damaging it leaves the patient with a permanent facial palsy, so salivary surgery is a model of nerve-preserving dissection. The commonest tumour, the pleomorphic adenoma, is benign but has a tendency to recur and even to undergo malignant change if it is incompletely removed, which dictates how it must be operated upon. For a final-year student, knowing the surgical anatomy, the pattern of presentation and the principles of safe, gland-appropriate surgery is exactly the knowledge a long case or viva will demand.
RECALL
Recall some foundations before we build on them. There are three pairs of major salivary glands — the parotid (the largest, in front of and below the ear), the submandibular (below the jaw) and the sublingual (in the floor of the mouth) — together with numerous minor salivary glands scattered through the oral and oropharyngeal mucosa. Recall the duct anatomy: the parotid duct (Stensen's duct) opens into the mouth opposite the upper second molar, while the submandibular duct (Wharton's duct) runs forwards across the floor of the mouth to open beside the frenulum of the tongue. Recall, above all, the course of the facial nerve (cranial nerve VII): it emerges from the stylomastoid foramen and passes forwards through the substance of the parotid gland, dividing it conceptually into a superficial and a deep lobe and then fanning out into its terminal branches to the muscles of facial expression — this single relationship governs the whole of parotid surgery. Finally, recall that saliva is mucinous and alkaline; its composition and the upward, anti-gravity course of Wharton's duct help explain why stones form so readily in the submandibular system.
The Patient with a Salivary Swelling
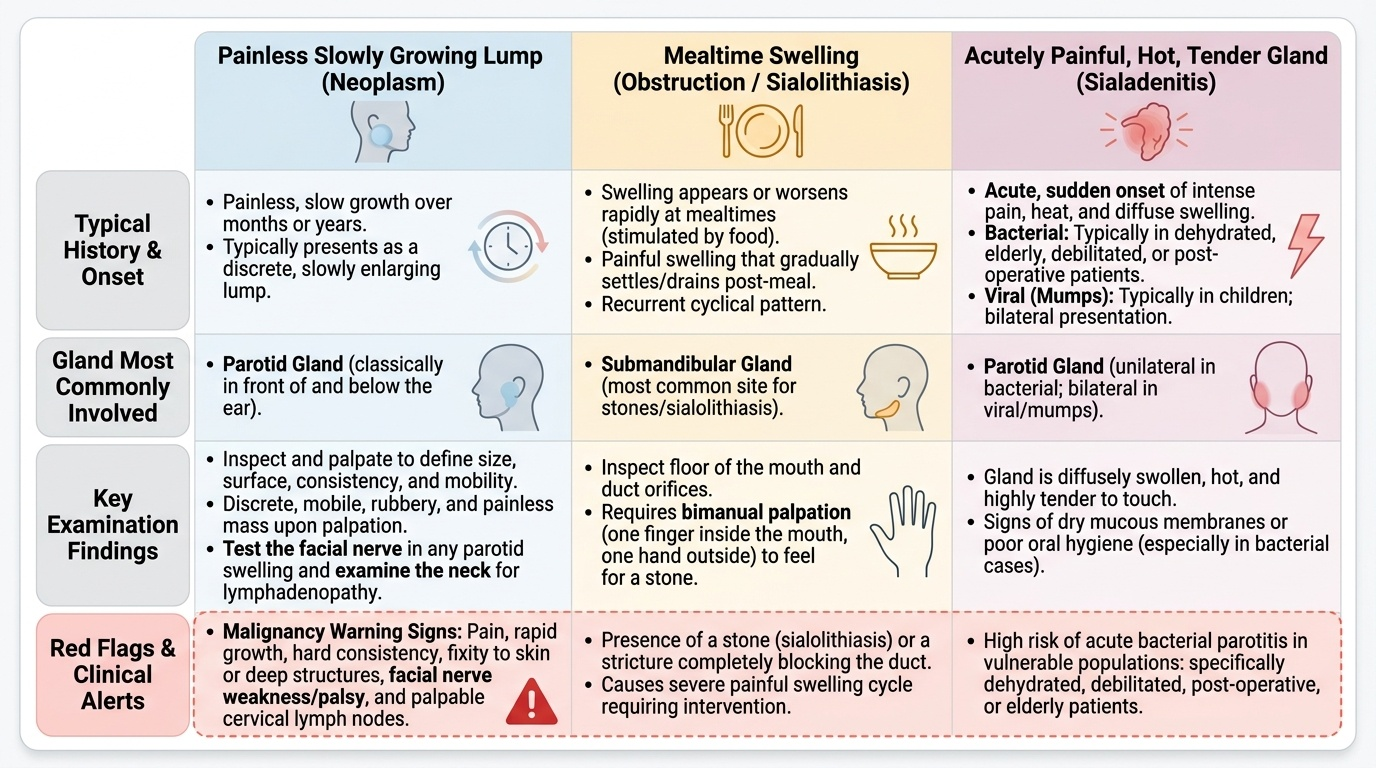
The presentation of a salivary gland disorder usually falls into one of three recognisable patterns, and taking a careful history of the swelling's behaviour does most of the diagnostic work before any test is ordered. The first pattern is the painless, slowly growing lump, which suggests a neoplasm: a benign tumour such as a pleomorphic adenoma typically presents as a discrete, mobile, rubbery, painless mass that has been enlarging slowly over months or years, classically in the parotid in front of and below the ear. Features that raise the alarm for malignancy — and which you must specifically seek — are pain, rapid growth, hardness, fixity to skin or deep structures, facial nerve weakness and palpable cervical lymph nodes; in particular, any facial nerve palsy in a parotid mass strongly suggests malignant infiltration of the nerve. The second pattern is the swelling that appears or worsens at mealtimes, the hallmark of obstruction: a stone (sialolithiasis) or a stricture blocking the duct causes the gland to swell painfully as saliva is stimulated by food and then to settle as the saliva slowly drains, a cycle the patient describes vividly as a recurrent mealtime swelling, most often in the submandibular gland. The third pattern is the acutely painful, hot, tender, diffusely swollen gland, the picture of acute sialadenitis (inflammation): acute bacterial parotitis classically afflicts the dehydrated, debilitated, post-operative or elderly patient with poor oral intake and reduced salivary flow, while viral parotitis (mumps) typically causes bilateral parotid swelling in a child. On examination the gland is inspected and palpated to define its size, surface, consistency and mobility; the floor of the mouth and the duct orifices are inspected and the duct is palpated bimanually (a finger in the mouth and a hand outside) to feel for a stone; the facial nerve is tested in any parotid swelling; and the neck is examined for lymphadenopathy.
Provided image
- Painless slow lump → neoplasm (e.g. pleomorphic adenoma); red flags for malignancy = pain, rapid growth, hardness, fixity, facial palsy, neck nodes.
- Mealtime swelling → obstruction (sialolithiasis/stricture), usually submandibular.
- Acute hot tender gland → sialadenitis (bacterial in the dehydrated/post-op/elderly; viral mumps, bilateral, in children).
- Examine: palpate the gland, bimanually palpate the duct for a stone, test the facial nerve, examine the neck.
Surgical Anatomy and Pathology
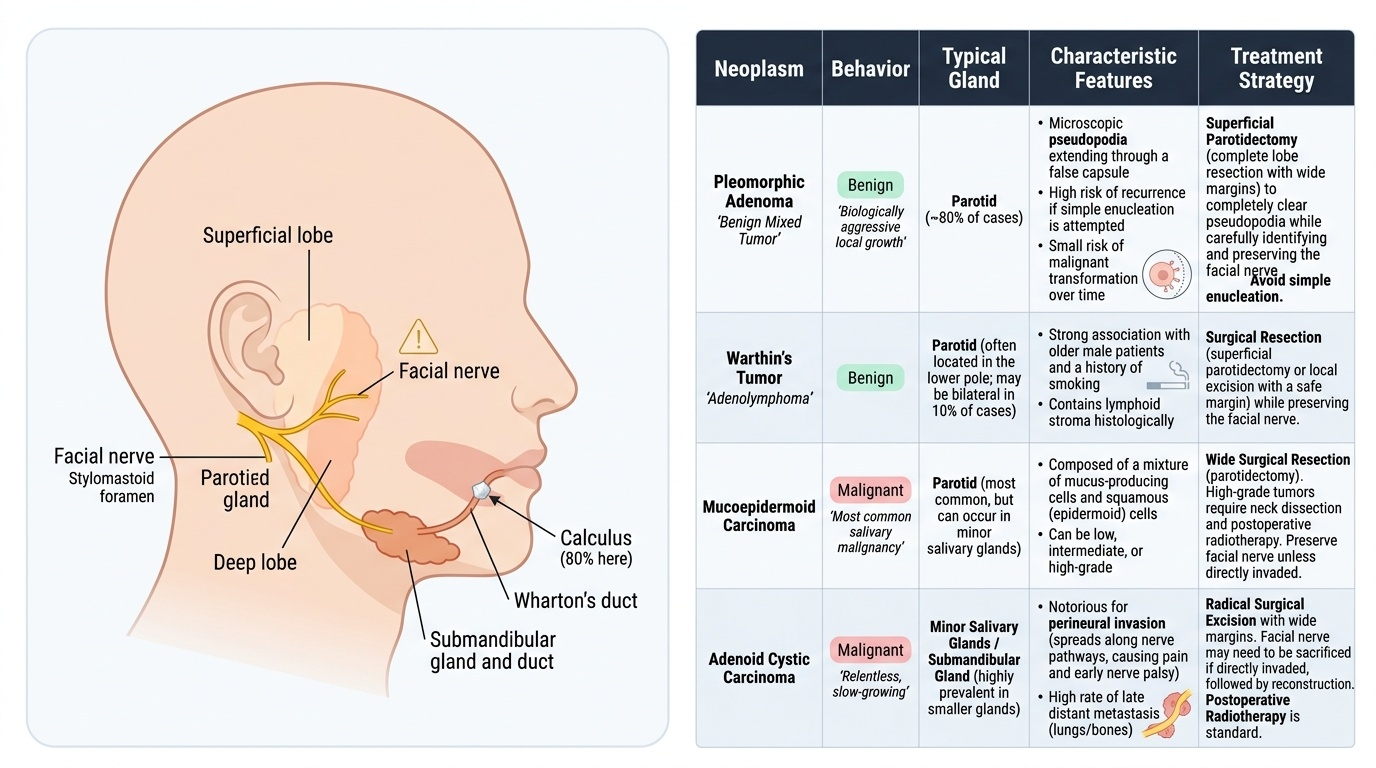
The surgical anatomy that matters most is the relationship of the facial nerve to the parotid gland. After leaving the stylomastoid foramen the facial nerve enters the parotid and divides within it, and surgeons use the plane of the nerve to describe a superficial lobe (lateral to the nerve, containing the bulk of the gland and most tumours) and a deep lobe (medial to the nerve). This is the single most important surgical fact about the parotid: because the nerve is embedded in the gland, it cannot simply be cut out, and any parotid operation is defined by identifying and preserving the facial nerve. The parotid (Stensen's) duct runs forwards over the masseter and pierces buccinator to open opposite the upper second molar; the submandibular (Wharton's) duct runs forwards and upwards across the floor of the mouth — an anti-gravity, uphill course through saliva that is rich in mucin and calcium — which is precisely why about 80% of salivary calculi form in the submandibular gland and its duct. Pathologically, salivary disorders divide into three groups. Inflammatory/infective disease — sialadenitis — includes acute bacterial parotitis (in the dehydrated/debilitated patient), viral parotitis (mumps) and chronic recurrent sialadenitis. Obstructive disease — sialolithiasis — is the formation of stones, overwhelmingly in the submandibular system, causing mealtime obstruction and predisposing to infection. Neoplastic disease follows useful rules of thumb: about 80% of salivary tumours arise in the parotid, about 80% of parotid tumours are benign, and about 80% of those benign parotid tumours are pleomorphic adenomas — but the smaller the gland, the higher the proportion of tumours that are malignant. The pleomorphic adenoma (benign mixed tumour) is the commonest salivary neoplasm, a benign but biologically awkward tumour with microscopic pseudopodia extending through a false capsule, which is why simple enucleation leaves tumour behind and leads to recurrence, and why long-standing tumours carry a risk of malignant transformation. Warthin's tumour (adenolymphoma) is a benign tumour that is characteristically found in the parotid of older male smokers and may be bilateral. Among malignant tumours, mucoepidermoid carcinoma is the commonest salivary malignancy, and adenoid cystic carcinoma is notorious for perineural spread, late recurrence and distant metastasis.
Provided image
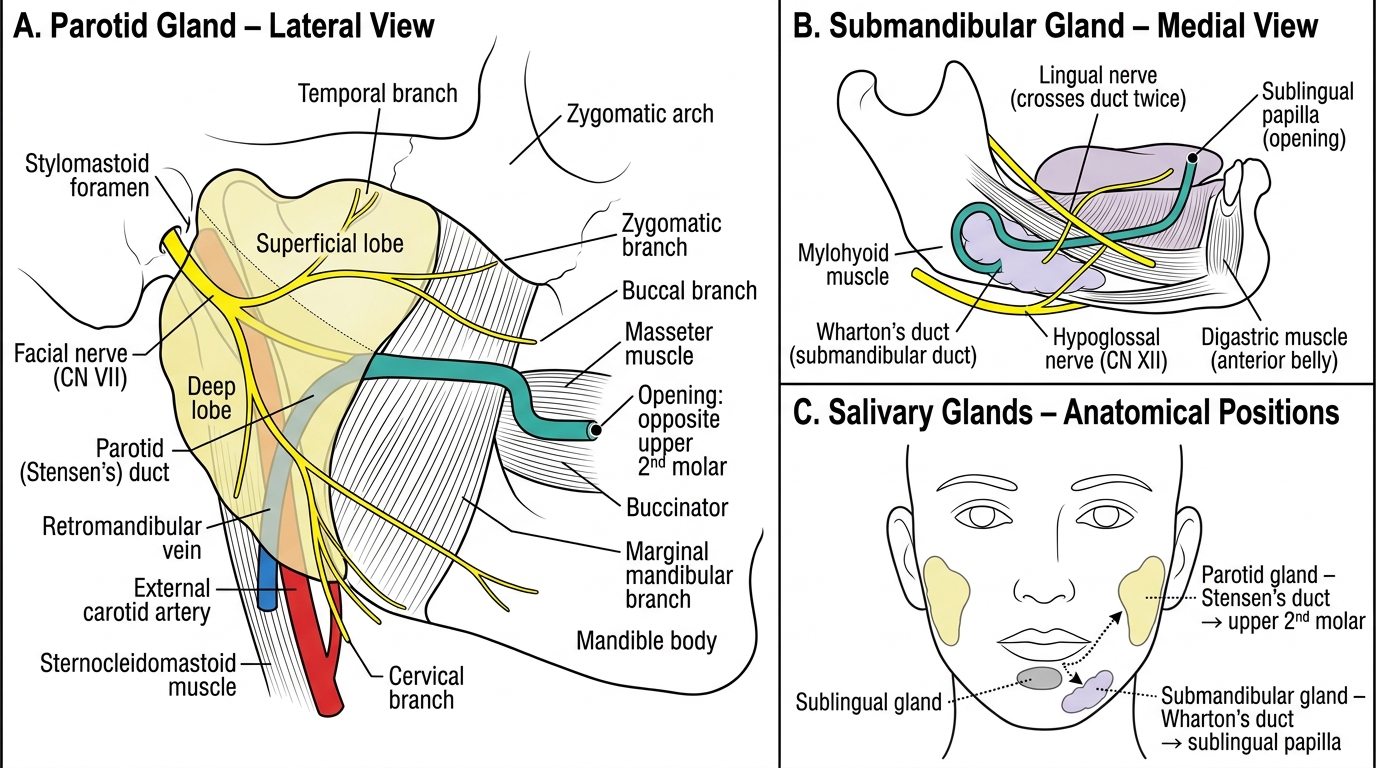
Major Salivary Glands: Parotid and Submandibular – Anatomy and Ductal Drainage
| Tumour | Behaviour | Typical gland | Characteristic feature | Treatment principle |
|---|---|---|---|---|
| Pleomorphic adenoma | Benign (commonest tumour) | Parotid (superficial lobe) | False capsule with pseudopodia; recurs if enucleated; risk of malignant change | Superficial parotidectomy with facial nerve preservation (not enucleation) |
| Warthin's tumour (adenolymphoma) | Benign | Parotid | Older male smokers; may be bilateral | Superficial parotidectomy / adequate local excision |
| Mucoepidermoid carcinoma | Malignant (commonest malignancy) | Parotid | Variable grade | Parotidectomy ± neck dissection ± radiotherapy |
| Adenoid cystic carcinoma | Malignant | Submandibular/minor glands | Perineural spread, late recurrence/metastasis | Wide excision ± nerve sacrifice ± radiotherapy |
SELF-CHECK
The facial nerve is the key surgical structure in parotid surgery because it:
A. Lies entirely deep to the gland and is rarely at risk
B. Passes through the parotid, dividing it into superficial and deep lobes, so it must be identified and preserved during surgery
C. Supplies sensation to the gland only
D. Can be safely divided because it regenerates fully
Reveal Answer
Answer: B. Passes through the parotid, dividing it into superficial and deep lobes, so it must be identified and preserved during surgery
The facial nerve (CN VII) emerges from the stylomastoid foramen and passes through the substance of the parotid, dividing it into a superficial and a deep lobe. Because the nerve is embedded within the gland, parotid surgery is defined by identifying and preserving it; damage causes facial palsy. A new facial palsy in a parotid mass suggests malignant infiltration.
Assessment and Investigation
Investigation of a salivary swelling is directed by the clinical pattern and aims to confirm the nature of the disorder, define its extent and, for a tumour, obtain a tissue diagnosis before surgery. Clinical examination remains the foundation: palpation of the gland, bimanual palpation of the duct for a stone, testing of the facial nerve in every parotid mass, and examination of the neck for lymph nodes. For a suspected stone, a plain radiograph may show a radio-opaque calculus (most submandibular stones are radio-opaque), and where available a sialogram (contrast injected into the duct) or, increasingly, ultrasound and CT demonstrate the stone and any ductal dilatation; sialendoscopy can both diagnose and treat ductal stones. For a suspected tumour, the two pillars are fine-needle aspiration cytology (FNAC), which gives a pre-operative tissue diagnosis and helps distinguish benign from malignant lesions, and cross-sectional imaging — ultrasound as a first-line test, with MRI being especially valuable for delineating the soft-tissue extent of a tumour, its relationship to the facial nerve and deep-lobe or parapharyngeal extension, and CT for bony involvement and staging. It is important to know that open incisional biopsy of a parotid lump is avoided, because it risks injuring the facial nerve and seeding tumour into the wound; FNAC (and, where needed, core biopsy) is the appropriate way to sample these masses. For sialadenitis, the diagnosis is largely clinical, supported by inflammatory markers, pus swabs for culture in bacterial parotitis, and ultrasound to look for an abscess or an underlying obstructing stone. Routine blood tests assess fitness for surgery and, in mumps, the diagnosis is clinical and serological. The investigations therefore mirror the three clinical patterns: imaging and endoscopy for obstruction, FNAC plus ultrasound/MRI for neoplasm, and clinical assessment with cultures and ultrasound for inflammation.
- All swellings: clinical examination incl. bimanual duct palpation, facial nerve testing, neck examination.
- Suspected stone: plain radiograph (radio-opaque stones), sialogram/ultrasound/CT, sialendoscopy (diagnostic + therapeutic).
- Suspected tumour: FNAC for tissue diagnosis + ultrasound (first line) and MRI (soft-tissue extent, nerve relationship) / CT (bone, staging); AVOID open incisional biopsy of a parotid lump.
- Sialadenitis: clinical + inflammatory markers, pus culture, ultrasound for abscess/stone.
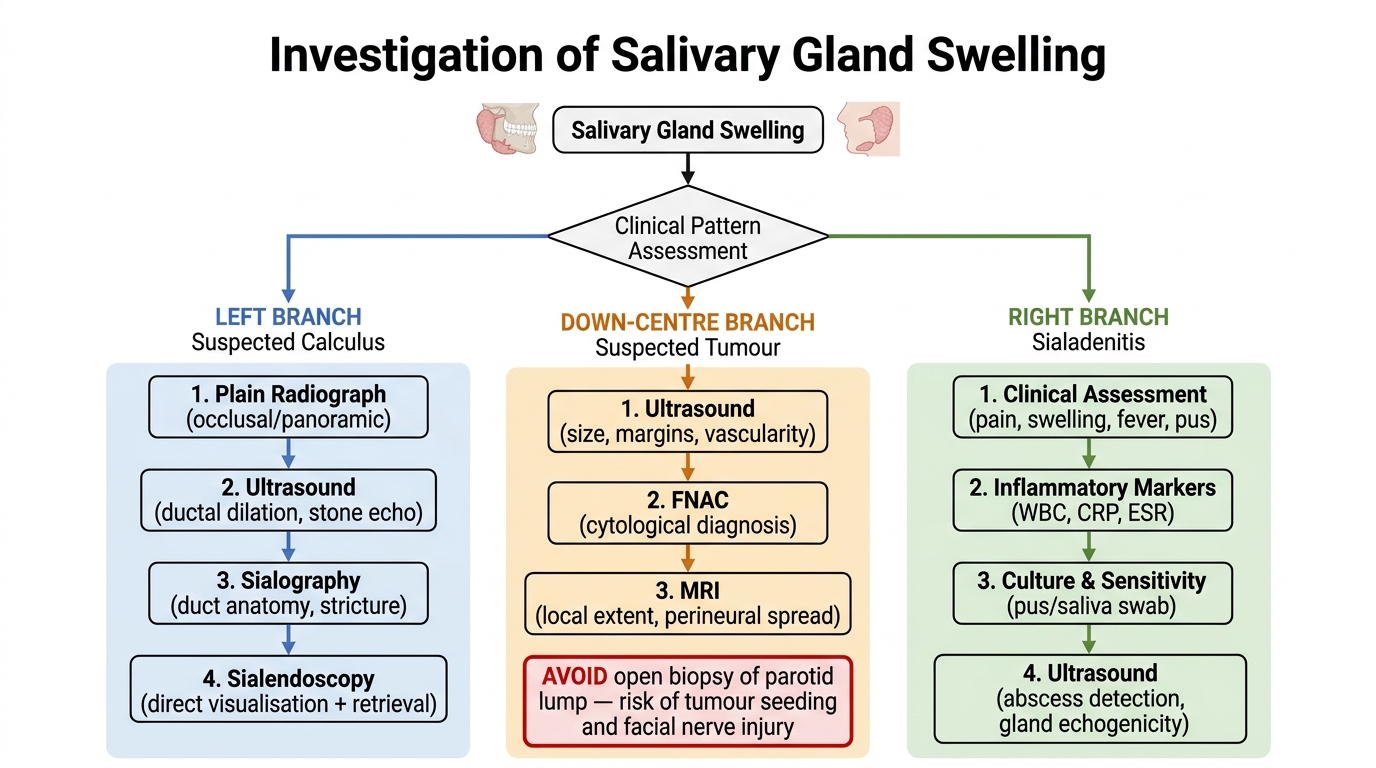
Algorithm for Investigation of Salivary Gland Swelling