Page 5 of 14
SU20.1-2 | Oropharyngeal Cancer — SDL Guide (Part 2)
Principles of Treatment
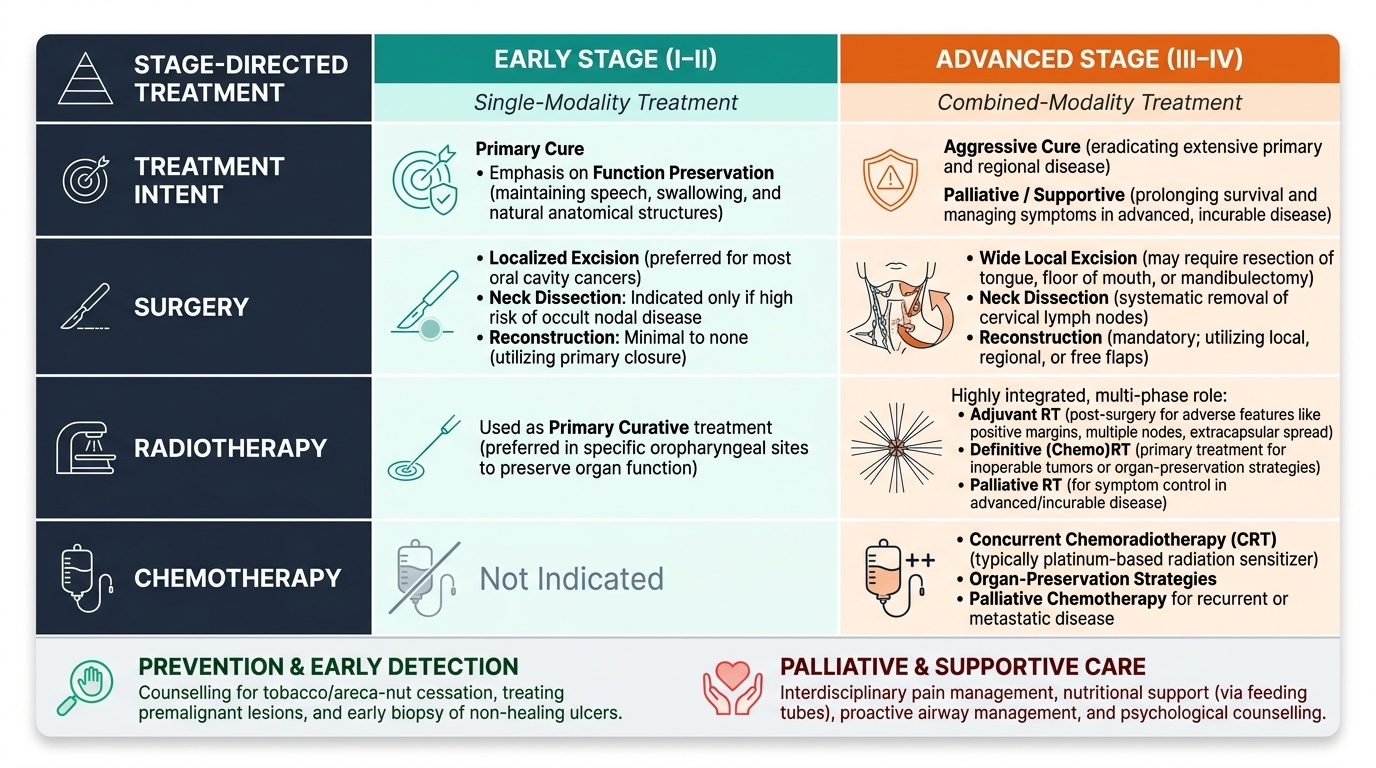
Treatment of oral and oropharyngeal cancer is stage-directed and multidisciplinary, decided by a tumour board and built on three modalities — surgery, radiotherapy and chemotherapy — used singly or in combination according to the site, stage and the patient's fitness and wishes. The first principle is that early-stage disease (stage I-II) is treated with a single modality — either surgery or radiotherapy — with the aim of cure while preserving function; for most oral-cavity cancers in this setting surgery is preferred, whereas radiotherapy has a larger role in some oropharyngeal sites. The second principle is that advanced disease (stage III-IV) requires combined-modality treatment, typically surgery followed by adjuvant radiotherapy or chemoradiotherapy, or definitive (chemo)radiotherapy. Surgically, the operation has two components: wide local excision of the primary tumour with an adequate margin (which may involve removing part of the tongue, floor of mouth, buccal mucosa or a segment of mandible — a mandibulectomy — when bone is involved), and management of the neck by lymph node (neck) dissection when nodes are involved or the risk of occult nodal disease is high. Because these resections can leave large, function-destroying defects, reconstruction — using local, regional (e.g. pectoralis major) or free flaps — is integral to restoring swallowing, speech and appearance. Radiotherapy is used as a primary curative treatment for suitable lesions, as adjuvant treatment after surgery for adverse features (positive margins, multiple nodes, extracapsular spread), and for palliation; chemotherapy (often platinum-based) is given concurrently with radiotherapy to enhance its effect in advanced disease, as part of organ-preservation strategies, and palliatively. Underpinning all of this are two further principles that are easy to forget in an exam but central in practice: prevention and early detection — counselling every patient to stop tobacco and areca-nut use, treating premalignant lesions, and biopsying non-healing ulcers early is the most effective way to reduce death from this disease — and palliative and supportive care, including pain control, nutrition (often via a feeding tube), airway management and psychological support, for patients who present with incurable disease.
Provided image
- Stage-directed: early (I-II) → single modality (surgery or radiotherapy); advanced (III-IV) → combined modality (surgery + adjuvant RT/chemoRT, or definitive chemoRT).
- Surgery: wide local excision with adequate margin (± mandibulectomy); neck dissection for nodal disease/high occult risk; reconstruction with flaps.
- Radiotherapy/chemotherapy: RT primary/adjuvant/palliative; concurrent platinum-based chemotherapy in advanced disease.
- Always: prevention and early detection (stop tobacco/areca, biopsy non-healing ulcers); palliative and supportive care when incurable.
CLINICAL PEARL
Treat any oral ulcer that has not healed in three weeks as cancer until proven otherwise, and remember that a RED patch (erythroplakia) is more dangerous than a WHITE one (leukoplakia). The cheapest, most effective intervention you can offer is not in the operating theatre — it is at the first consultation: examine the whole mouth and neck, biopsy the suspicious lesion promptly rather than treating it as an aphthous ulcer, and counsel the patient to stop tobacco and areca-nut use. Early oral cancer is highly curable; the commonest reason it is not cured is that nobody looked early enough.
Check Your Understanding
Bring the threads together by reasoning back through the tobacco-and-areca-nut chewer in the hook. His thirty-year habit is the dominant risk factor; the white patch he ignored for years was a premalignant leukoplakia; the two-month non-healing ulcer on the lateral tongue with an indurated base is the classic presentation of an invasive squamous cell carcinoma; his mouth stiffness suggests coexistent oral submucous fibrosis; and the hard neck lump signals lymph-node metastasis and therefore advanced disease. His correct work-up is triple assessment — bimanual palpation and neck examination, incisional biopsy of the ulcer (and FNAC of the node), CT/MRI of the head and neck with chest imaging, and panendoscopy to exclude a second primary — feeding into a TNM stage that will determine whether he is offered single-modality or combined-modality treatment. Use this case to self-test the two competencies this module covers. First, can you describe the aetiopathogenesis of oral cancer (SCC; tobacco/areca-nut/alcohol/HPV; the premalignant leukoplakia, erythroplakia and OSMF) and recognise its symptoms and signs, including the warning of a non-healing ulcer and a hard neck node? Second, can you enumerate the appropriate investigations (triple assessment, biopsy/FNAC, CT/MRI, chest imaging, panendoscopy, TNM staging) and discuss the stage-directed principles of treatment (single vs combined modality; surgery with neck dissection and reconstruction; radiotherapy and chemotherapy; prevention and palliation)? The questions that follow check exactly these links.
SELF-CHECK
A patient has a biopsy-proven oral squamous cell carcinoma with a hard, mobile cervical lymph node. Which statement best reflects the principles of staging and treatment?
A. Treatment can be planned on the biopsy alone without staging
B. TNM staging guides treatment; advanced disease with nodal involvement typically needs combined-modality treatment including neck dissection and adjuvant radiotherapy/chemoradiotherapy
C. Chemotherapy alone cures most advanced oral cancers
D. Radiotherapy is contraindicated once a node is involved
Reveal Answer
Answer: B. TNM staging guides treatment; advanced disease with nodal involvement typically needs combined-modality treatment including neck dissection and adjuvant radiotherapy/chemoradiotherapy
The TNM stage — incorporating the primary tumour, nodal involvement and metastasis — is the key determinant of treatment. A palpable metastatic node indicates more advanced disease, which is managed with combined-modality treatment: surgery (wide local excision plus neck dissection) typically followed by adjuvant radiotherapy or chemoradiotherapy, rather than any single modality alone.