Page 7 of 14
SU22.5-6 | Parathyroid Anatomy and Parathyroid Disorders — SDL Guide
Learning Objectives
- Describe the applied surgical anatomy of the parathyroid glands, including their number, position, embryology and blood supply (SU22.5).
- Describe and discuss the clinical features of hyper- and hypoparathyroidism and classify hyperparathyroidism into primary, secondary and tertiary forms (SU22.6).
- Outline the principles of management of parathyroid disorders, including pre-operative localisation and parathyroidectomy (SU22.6).
INSTRUCTIONS
The parathyroid glands are tiny, easily overlooked, and yet they govern one of the body's most tightly controlled variables — the serum calcium. They matter to the surgeon twice over: as glands that can be injured during thyroid surgery, causing dangerous hypocalcaemia, and as the site of disease in their own right, most often a small adenoma that drives the calcium up. This module connects the applied anatomy and the physiology of calcium control to the clinical pictures of too much and too little parathyroid hormone, the biochemical patterns that separate the types of hyperparathyroidism, and the principles of localisation and surgery that allow a pea-sized adenoma to be found and removed safely.
References
- Bailey & Love's Short Practice of Surgery, The Parathyroid and Adrenal Glands (textbook)
- SRB's Manual of Surgery, Parathyroid Glands (textbook)
- Sabiston Textbook of Surgery, The Parathyroid Glands (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old woman is referred with recurrent kidney stones, vague bone aches, constipation and a low mood her family describe as 'just not herself'. Her bones, her kidneys, her gut and her mind all seem to be complaining at once, and nothing on examination ties them together. Then a routine blood test shows a high serum calcium. Suddenly the scattered complaints fall into a single pattern — 'stones, bones, abdominal groans and psychiatric moans' — and the culprit is a gland most people have never heard of: a single overactive parathyroid the size of a pea. This is the recurring theme of parathyroid disease: a tiny gland with an outsized effect, betrayed not by a lump in the neck but by the calcium it controls.
WHY THIS MATTERS
Parathyroid disease reaches the surgeon along two routes, and both are common enough to matter. First, primary hyperparathyroidism is one of the commonest causes of hypercalcaemia and is eminently curable by removing a single adenoma — but only if the diagnosis is made and the gland is found. Second, every thyroidectomy puts the parathyroids at risk, so understanding their anatomy and the consequences of damaging them is essential to safe thyroid surgery. Recognising the biochemical fingerprints that separate primary, secondary and tertiary hyperparathyroidism, knowing how to localise an adenoma before operating, and treating post-operative hypocalcaemia promptly are skills that prevent both unnecessary suffering and life-threatening complications.
RECALL
Recall two anchors from earlier in this cluster. From the thyroid swellings SDL: the four parathyroid glands sit on the posterior surface of the thyroid lobes and depend largely on the inferior thyroid artery for their blood supply, which is exactly why they are at risk during thyroidectomy and why their inadvertent removal or devascularisation causes hypocalcaemia. From the thyroid cancer SDL: the MEN-2A syndrome links parathyroid disease with medullary thyroid carcinoma and phaeochromocytoma, while MEN-1 links it with pancreatic and pituitary tumours. Keep in mind, too, the basic physiology of calcium control from PY: parathyroid hormone raises serum calcium by acting on bone, kidney and (via vitamin D) the gut, regulated by negative feedback through the calcium-sensing receptor.
Calcium Trouble: How Parathyroid Disease Presents
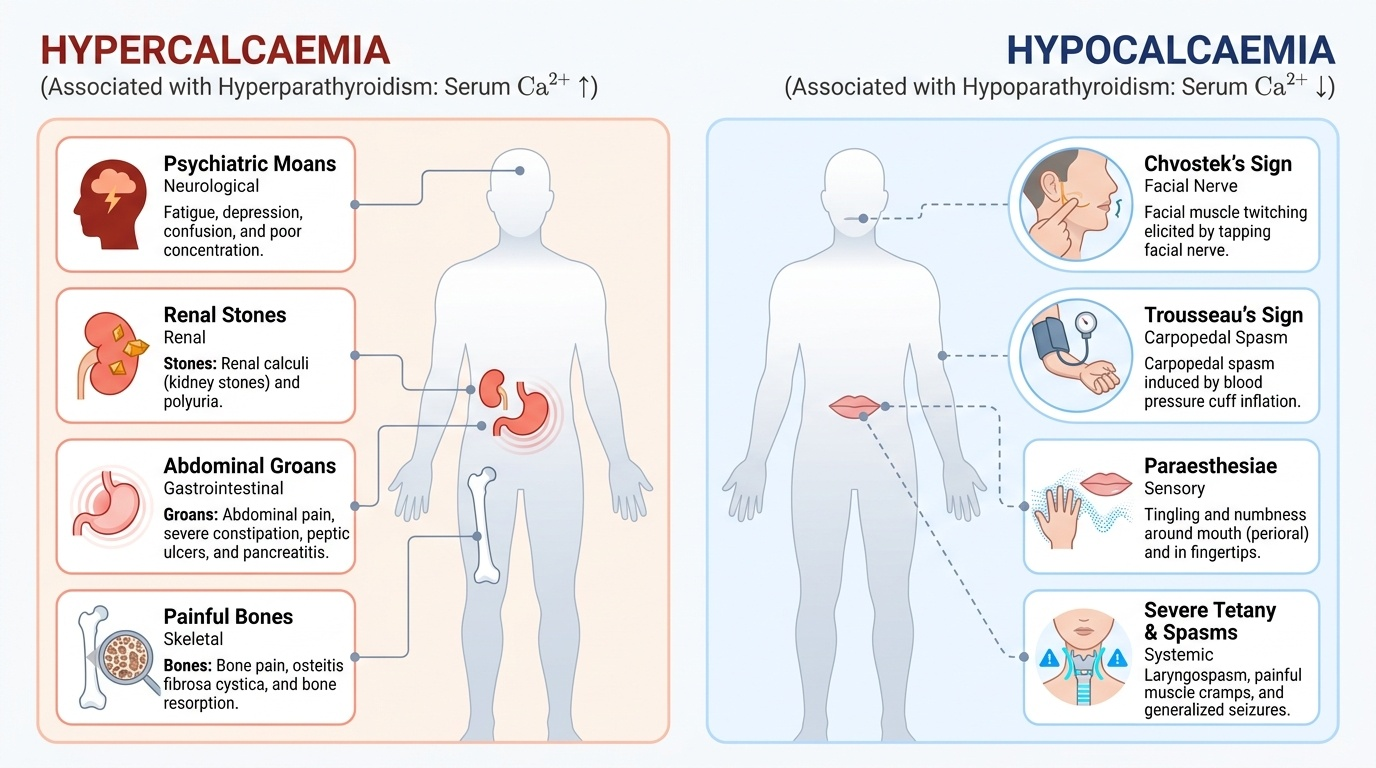
Parathyroid disorders almost never present as a neck lump; they present through the serum calcium, so the clinical features are those of hypercalcaemia or hypocalcaemia. Hyperparathyroidism, by driving the calcium up, produces the classic constellation captured as 'stones, bones, abdominal groans and psychiatric moans': renal calculi and polyuria from the high calcium load on the kidney; bone pain and, in severe long-standing disease, the characteristic bone resorption of osteitis fibrosa cystica; abdominal pain, constipation, peptic ulceration and pancreatitis; and neuropsychiatric features ranging from fatigue and poor concentration to depression and confusion. Many patients today, however, are detected incidentally with only mild biochemical hypercalcaemia and few symptoms. Hypoparathyroidism, by contrast, lowers the calcium and so causes neuromuscular irritability: perioral and digital paraesthesiae, muscle cramps, and the eponymous signs of latent tetany — Chvostek's sign (facial twitch on tapping the facial nerve) and Trousseau's sign (carpopedal spasm with arm cuff inflation) — progressing in severe cases to frank tetany, laryngospasm and seizures. Recognising which way the calcium has moved is the first step in every parathyroid problem.
Provided image
- Hypercalcaemia (hyperparathyroidism): stones (renal calculi), bones (pain, osteitis fibrosa cystica), groans (abdominal pain, constipation, pancreatitis), moans (depression, confusion).
- Hypocalcaemia (hypoparathyroidism): perioral/digital paraesthesiae, Chvostek's and Trousseau's signs, cramps, tetany, laryngospasm, seizures.
Applied Anatomy and the Physiology of Calcium Control
There are usually four parathyroid glands, each only a few millimetres across, lying on the posterior surface of the thyroid lobes: the superior pair are relatively constant in position, while the inferior pair are more variable and may lie low in the neck or even within the thymus, a fact that explains why an adenoma is sometimes hard to find. Embryologically the superior glands arise from the fourth pharyngeal pouch and the inferior glands from the third pouch (descending with the thymus, which is why the inferior glands are the more ectopic). Their blood supply comes largely from the inferior thyroid artery, so they are vulnerable during thyroid surgery. Functionally, parathyroid hormone (PTH) is the master regulator of calcium: it raises serum calcium by mobilising it from bone, increasing its reabsorption in the kidney while promoting phosphate excretion, and stimulating renal activation of vitamin D to enhance calcium absorption from the gut; the gland senses calcium through the calcium-sensing receptor and secretes PTH by negative feedback. Disease of these glands is classified by the calcium-PTH disturbance: hyperparathyroidism is primary (autonomous PTH excess — a single adenoma in about 85% of cases, hyperplasia, or rarely carcinoma), secondary (an appropriate compensatory rise in PTH driven by the chronic hypocalcaemia of chronic kidney disease or vitamin D deficiency), or tertiary (PTH secretion that has become autonomous after long-standing secondary disease, classically after renal transplantation); hypoparathyroidism is deficient PTH, most often iatrogenic after neck surgery.
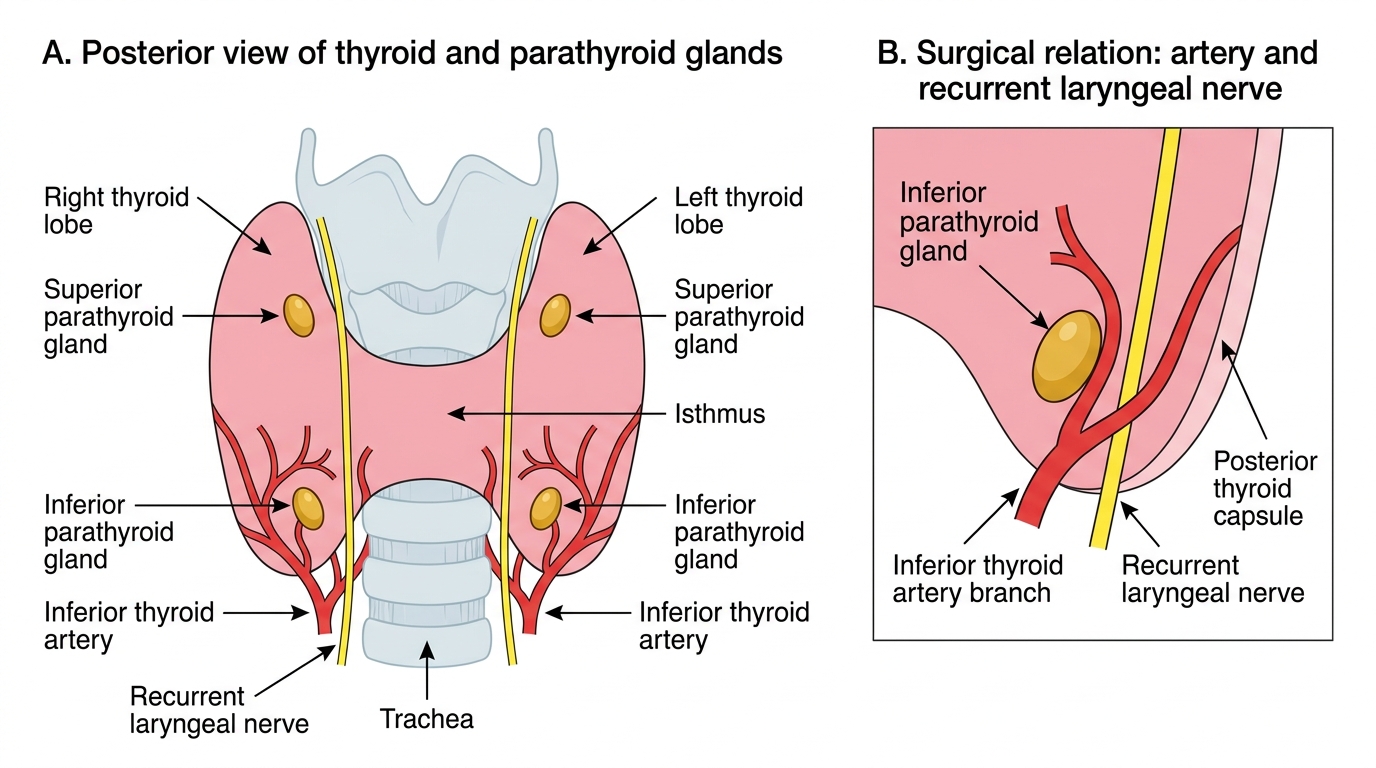
Posterior Thyroid: Parathyroid Glands and Surgical Relations
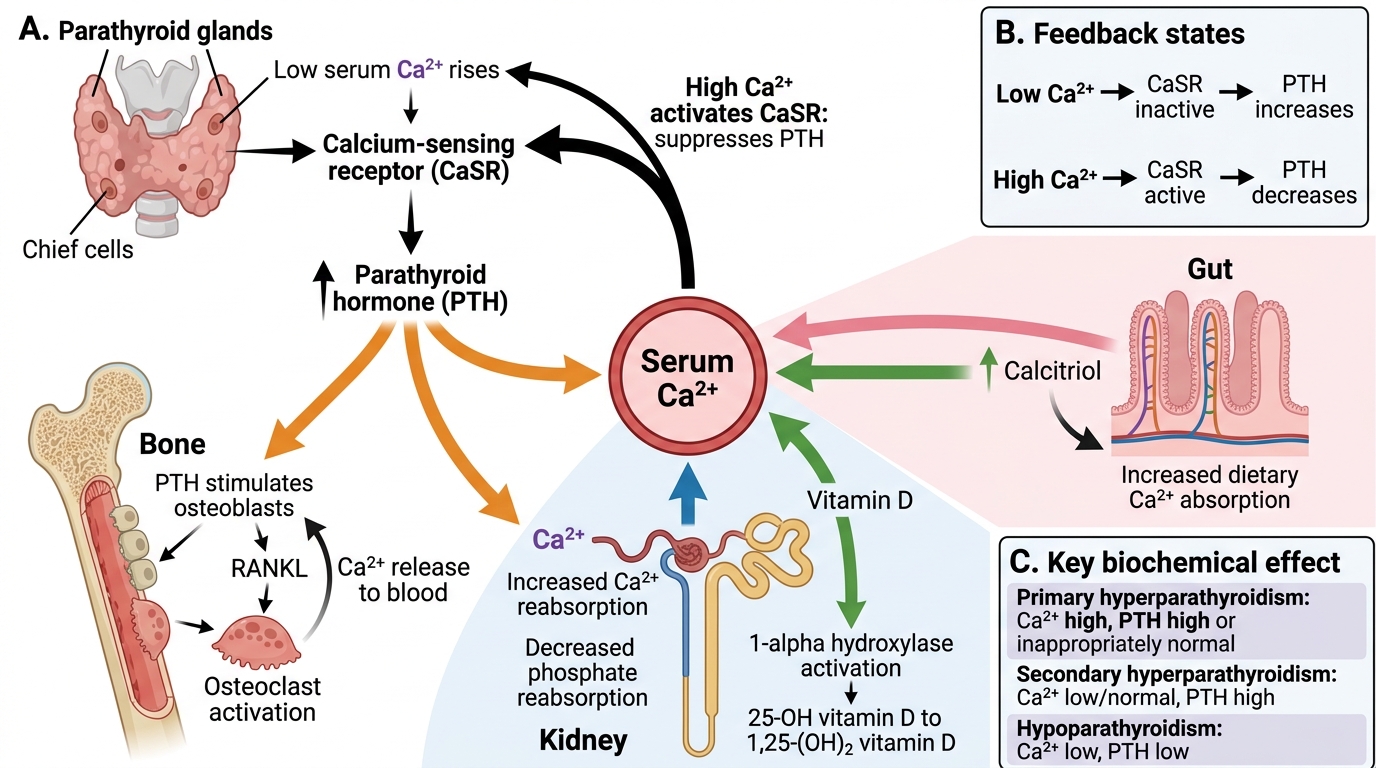
Calcium Homeostasis and Parathyroid Hormone Feedback
- Anatomy: usually 4 glands, posterior thyroid; superior from 4th pouch, inferior from 3rd pouch (more ectopic); supplied by inferior thyroid artery.
- Classification of hyperparathyroidism: primary (adenoma ~85%), secondary (CKD/vitamin D deficiency), tertiary (autonomous after long-standing secondary).
SELF-CHECK
Which biochemical pattern is characteristic of PRIMARY hyperparathyroidism?
A. Low serum calcium with high PTH
B. High serum calcium with high or inappropriately normal PTH
C. Low serum calcium with low PTH
D. Normal serum calcium with low PTH
Reveal Answer
Answer: B. High serum calcium with high or inappropriately normal PTH
Primary hyperparathyroidism is autonomous PTH excess, so the calcium is HIGH while the PTH is high or inappropriately normal (it should be suppressed by the high calcium but is not). Low calcium with high PTH is secondary hyperparathyroidism; low calcium with low PTH is hypoparathyroidism.
Diagnosing and Localising Parathyroid Disease
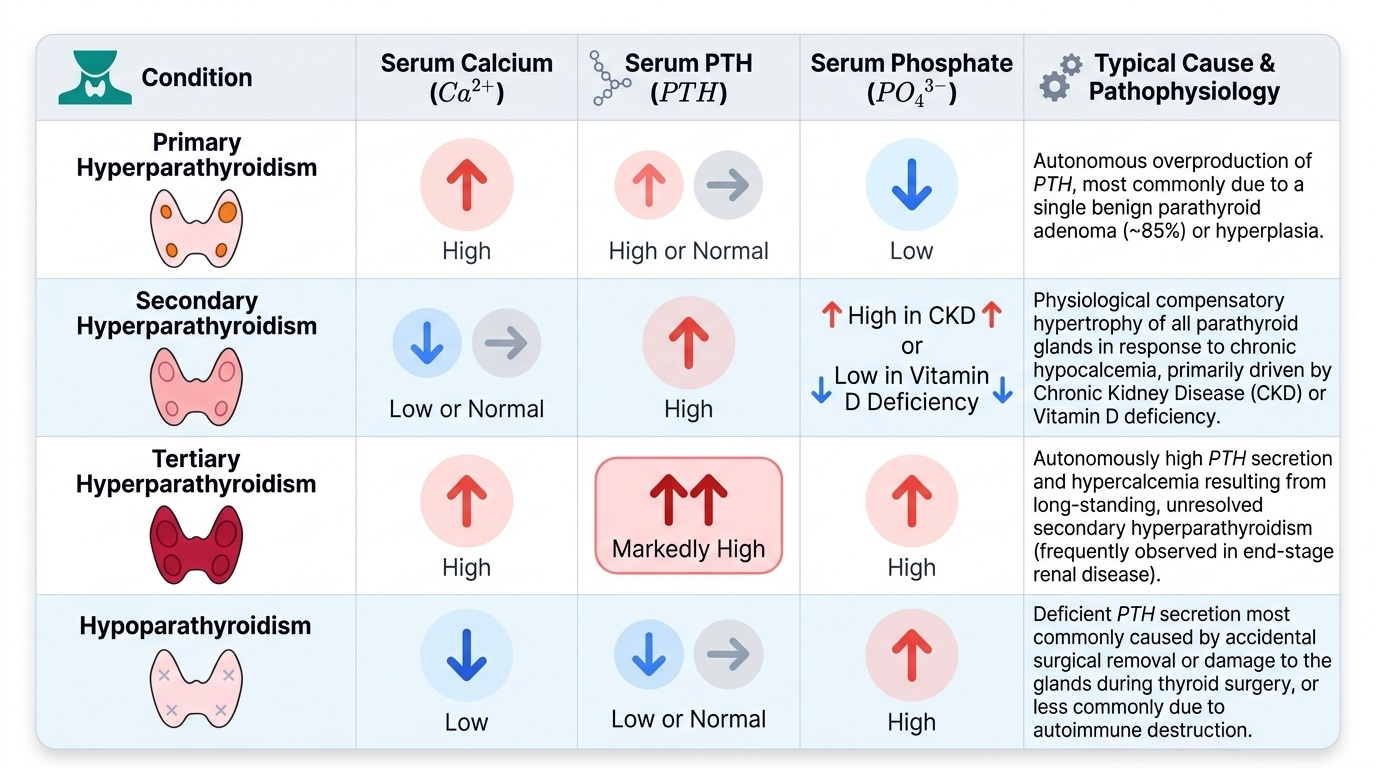
Parathyroid disease is diagnosed biochemically and only then localised anatomically — the sequence matters because surgery is never planned on imaging alone. The core tests are serum calcium, PTH and phosphate, and their pattern separates the diagnoses. In primary hyperparathyroidism the calcium is high with a PTH that is high or inappropriately normal, and the phosphate tends to be low. In secondary hyperparathyroidism the calcium is low or normal with a high PTH, reflecting an appropriate response to the hypocalcaemia of chronic kidney disease or vitamin D deficiency. In tertiary hyperparathyroidism the PTH remains autonomously high but the calcium has risen to high after long-standing secondary stimulation. In hypoparathyroidism the calcium is low with a PTH that is low or inappropriately normal and a high phosphate. Once a surgical diagnosis of primary hyperparathyroidism is confirmed, the offending gland is localised pre-operatively to allow focused surgery: neck ultrasound and technetium-99m sestamibi scintigraphy are the standard combination, with cross-sectional imaging reserved for ectopic or re-operative cases. Twenty-four-hour urinary calcium helps exclude the benign mimic familial hypocalciuric hypercalcaemia, which must not be operated on.
Provided image
| Disorder | Calcium | PTH | Phosphate | Typical cause |
|---|---|---|---|---|
| Primary hyperparathyroidism | High | High / inappropriately normal | Low | Adenoma (~85%), hyperplasia |
| Secondary hyperparathyroidism | Low / normal | High | High (in CKD) | CKD, vitamin D deficiency |
| Tertiary hyperparathyroidism | High | High (autonomous) | Variable / high | Long-standing secondary (e.g. post-transplant) |
| Hypoparathyroidism | Low | Low / inappropriately normal | High | Post-surgical, autoimmune |