Page 1 of 14
SU22.1-3 | Thyroid Anatomy, Physiology and Swellings — SDL Guide
Learning Objectives
- Describe the applied anatomy and physiology of the thyroid gland relevant to its surgery (SU22.1).
- Describe the etiopathogenesis of thyroidal swellings, including the classification of goitre and thyroid malignancy (SU22.2).
- Demonstrate and document a correct clinical examination of a thyroid swelling and outline its differential diagnosis and management (SU22.3).
INSTRUCTIONS
A swelling in the front of the neck is one of the commonest surgical referrals, and the thyroid sits behind most of them. The central clinical task is simple to state and demanding to execute: decide whether a thyroid swelling is benign or malignant, and treat it without injuring the nerves and parathyroid glands that lie millimetres away. This module connects the gland's surgical anatomy and physiology to a disciplined examination, an evidence-based nodule work-up, and safe operative decisions.
References
- Bailey & Love's Short Practice of Surgery, The Thyroid Gland and Thyroglossal Tract (textbook)
- SRB's Manual of Surgery, Thyroid Gland (textbook)
- Sabiston Textbook of Surgery, The Thyroid Gland (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old woman comes to clinic having noticed a lump in the front of her neck that moves when she swallows. She is otherwise well, with no change in weight, bowel habit or temperature tolerance, and no hoarseness. On the other side of the room sits a 70-year-old man whose neck lump appeared only six weeks ago, is already hard and fixed, and whose voice has become husky. The same anatomical region, two completely different stories — and your job is to tell, quickly and safely, which swelling can be reassured and watched and which demands urgent investigation. Everything you will examine, request and decide flows from understanding the gland that lies beneath that moving lump.
WHY THIS MATTERS
Thyroid swellings are common, and most are benign — but the minority that are malignant are highly treatable when caught early and dangerous when missed. The surgically critical point is that the thyroid is wrapped around the airway and shares its bed with the recurrent laryngeal nerves and the parathyroid glands; a careless thyroidectomy can leave a patient hoarse, breathless or hypocalcaemic for life. Knowing the applied anatomy turns the operation from a hazard into a controlled procedure, and knowing the orderly nodule work-up keeps you from either over-treating colloid nodules or under-investigating a cancer. For a final-year student, the thyroid is also a classic long case: a clean, reproducible examination and a clear differential are expected of you.
RECALL
Recall some foundations before we build on them. From anatomy: the thyroid develops from the foramen caecum at the base of the tongue and descends along the thyroglossal duct, which explains thyroglossal cysts and the gland's characteristic movement on swallowing (it is invested by the pretracheal fascia and bound to the larynx). From physiology: the gland traps iodide and synthesises the hormones T4 and T3, under the control of pituitary TSH within the hypothalamic-pituitary-thyroid axis, so serum TSH is the single most sensitive index of thyroid function. Hold on to two anatomical neighbours in particular — the recurrent laryngeal nerve supplying the larynx, and the four parathyroid glands controlling calcium — because protecting them defines safe thyroid surgery.
The Patient with a Neck Swelling
A thyroid swelling classically presents as a painless lump in the lower anterior neck that moves upwards on swallowing — because the gland is bound to the larynx by the pretracheal fascia — and, if it is a thyroglossal cyst, also on tongue protrusion. The history is what first separates the benign from the worrying. Ask about the rate of growth (a lump present for years that suddenly enlarges, or any rapidly growing mass, raises concern), about pressure symptoms (dysphagia, dyspnoea, stridor or a sensation of tightness from tracheal or oesophageal compression), and about voice change — hoarseness suggests recurrent laryngeal nerve involvement and is a red flag for malignancy. Screen for thyroid status: weight loss, heat intolerance, palpitations and tremor suggest hyperthyroidism, while weight gain, cold intolerance, constipation and lethargy suggest hypothyroidism; many goitres are euthyroid. Finally ask about risk factors — childhood neck irradiation, a family history of thyroid cancer or MEN syndromes, and residence in an iodine-deficient endemic-goitre area. This structured history already points you towards the likely diagnosis before you lay a hand on the neck.
Applied Anatomy, Physiology and the Pathogenesis of Goitre
Safe thyroid surgery is anatomy made practical. The gland has two lobes joined by an isthmus and is supplied by the superior thyroid artery (a branch of the external carotid, intimately related to the external laryngeal nerve, which supplies cricothyroid — injury causes a weak, easily tired voice) and the inferior thyroid artery (from the thyrocervical trunk, closely related to the recurrent laryngeal nerve, which supplies all the other intrinsic laryngeal muscles — unilateral injury causes hoarseness, bilateral injury threatens the airway). The four parathyroid glands lie on the posterior aspect of the lobes and depend largely on the inferior thyroid artery, so they are at risk during dissection; their inadvertent removal or devascularisation causes hypocalcaemia. Physiologically the gland makes T4 and T3 under TSH control. The term goitre simply means thyroid enlargement, and its causes are best classified by pattern and aetiology: diffuse swellings (simple/colloid goitre, physiological goitre of puberty or pregnancy, Graves' disease, and the thyroiditides) versus nodular swellings (a solitary thyroid nodule or a multinodular goitre). Neoplastic swellings — benign follicular adenoma and the thyroid carcinomas — usually present within the nodular group, which is precisely why a solitary nodule must always be worked up.
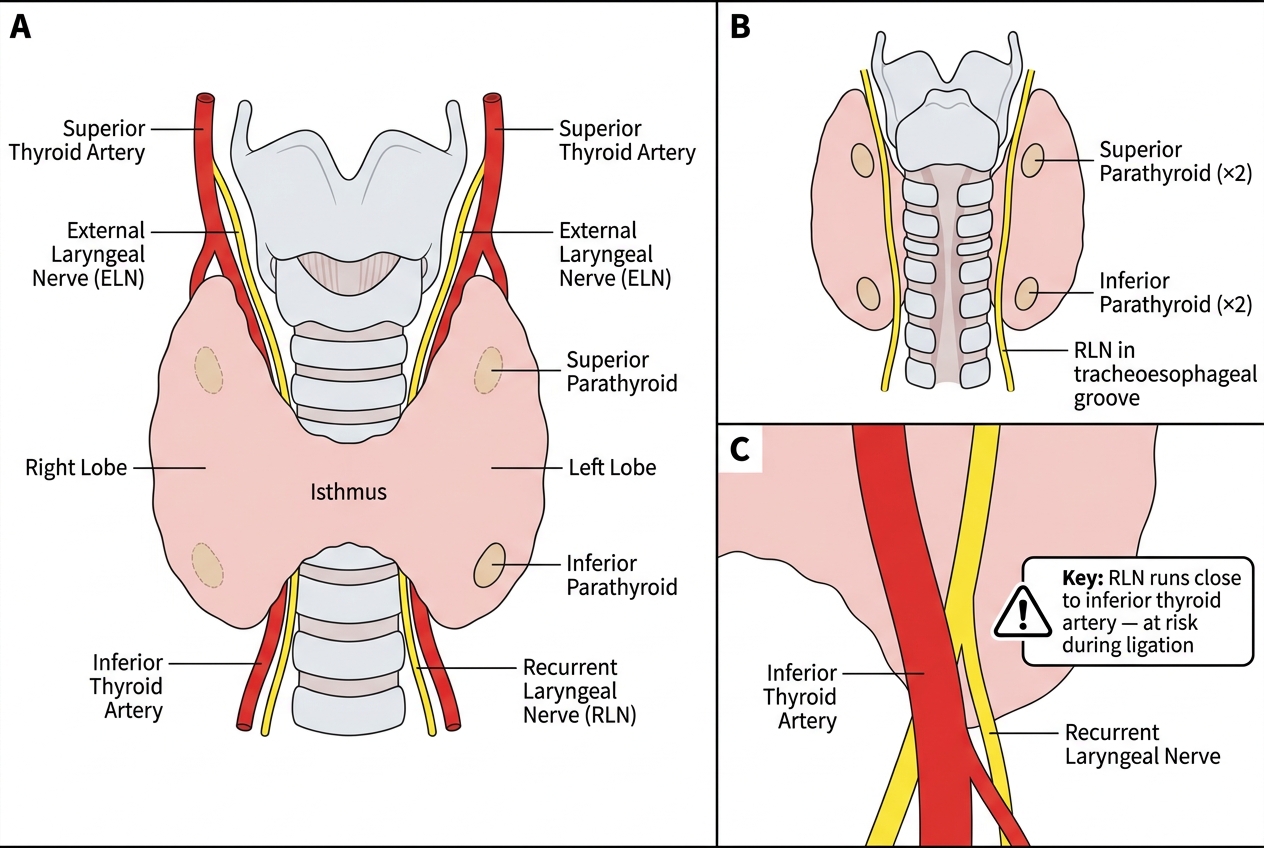
Surgical Anatomy of the Thyroid Gland: Vascular Supply, Nerves, and Parathyroid Relations
- Diffuse goitre: simple/colloid, physiological (puberty/pregnancy), Graves' disease, thyroiditis.
- Nodular goitre: solitary thyroid nodule, multinodular goitre.
- Neoplastic: benign (follicular adenoma); malignant (papillary, follicular, medullary, anaplastic, lymphoma).
SELF-CHECK
During thyroidectomy, the inferior thyroid artery is most closely related to which structure that must be preserved?
A. The external laryngeal nerve
B. The recurrent laryngeal nerve
C. The hypoglossal nerve
D. The phrenic nerve
Reveal Answer
Answer: B. The recurrent laryngeal nerve
The recurrent laryngeal nerve runs in close relation to the inferior thyroid artery and supplies all intrinsic laryngeal muscles except cricothyroid; the external laryngeal nerve is related to the SUPERIOR thyroid artery. Unilateral recurrent laryngeal nerve injury causes hoarseness; bilateral injury can obstruct the airway.
Examining the Thyroid and Investigating the Nodule
The clinical examination of the thyroid is a set-piece that should be performed and documented the same way every time. Inspect from the front with the patient seated, looking for the swelling and asking the patient to swallow a sip of water (a thyroid swelling rises) and then to protrude the tongue (a thyroglossal cyst rises). Palpate from behind with both hands, defining the size, surface, consistency, mobility and lower border of each lobe and the isthmus, noting whether the lump is solitary or multinodular, smooth or hard, and whether the lower border is reachable (if not, suspect retrosternal extension). Then assess the cervical lymph nodes and check for tracheal deviation. Percuss the manubrium for retrosternal dullness and auscultate for a bruit (Graves'). Complete the examination with an assessment of thyroid status. Once a discrete nodule is found, it is investigated in a fixed, evidence-based order: first serum TSH (a suppressed TSH points to an autonomously functioning, usually benign, 'hot' nodule warranting a radionuclide scan; a normal or raised TSH proceeds to imaging), then ultrasound to characterise the nodule and node fields, then fine-needle aspiration cytology (FNAC) of suspicious nodules, reported by the Bethesda system (categories I–VI) which stratifies the risk of malignancy and guides management.
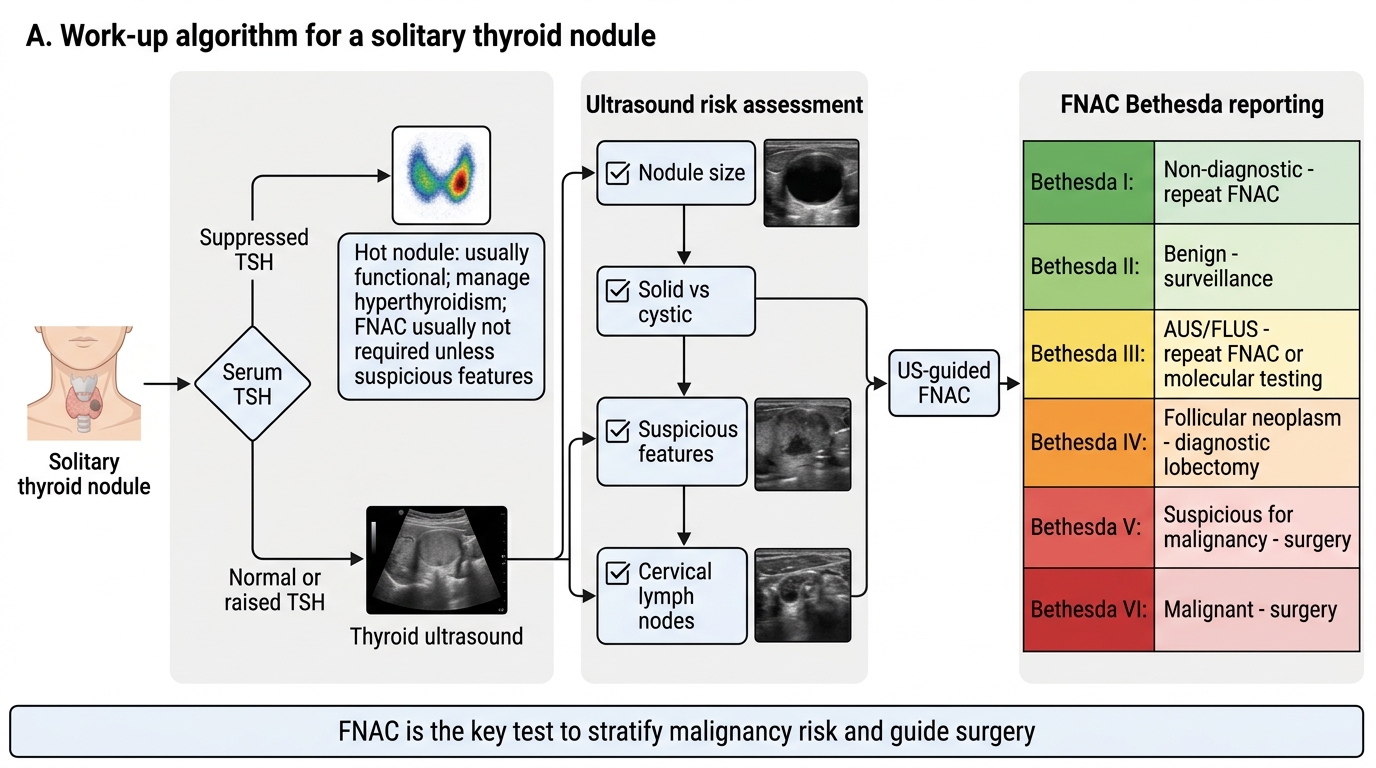
Solitary Thyroid Nodule Work-Up Algorithm
- TSH first: suppressed → consider 'hot' nodule (radionuclide scan); normal/raised → imaging.
- Ultrasound: size, solid vs cystic, suspicious features, lymph nodes.
- FNAC (Bethesda I–VI): the key test to stratify malignancy risk and direct surgery.