Page 5 of 17
SU25.2 | Benign Breast Disease — SDL Guide (Part 2)
Principles of Management of Benign Breast Disease
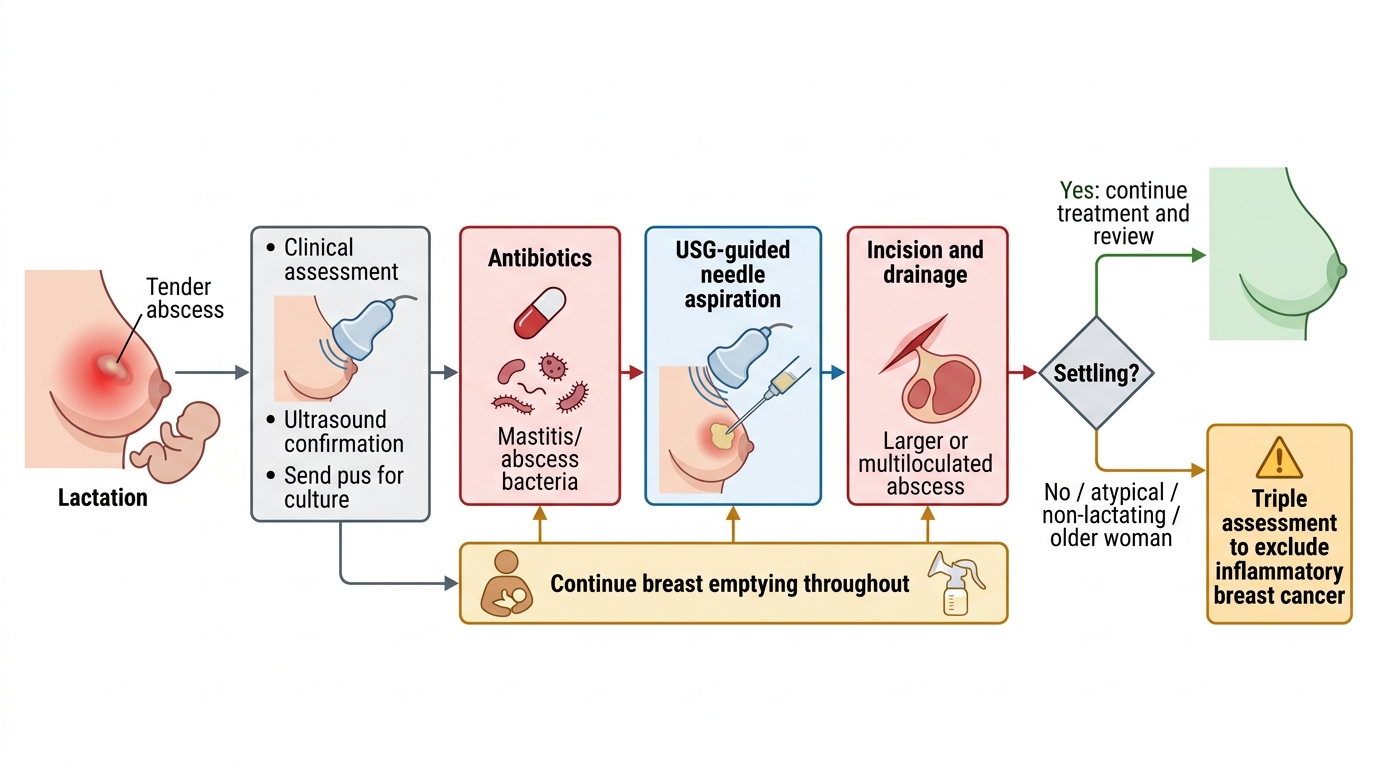
Once a condition is confirmed benign, management follows clear principles, ranging from reassurance to targeted intervention. A small, asymptomatic fibroadenoma with concordant benign triple assessment can simply be observed and reassured; excision is offered if it is large (often >3-4 cm), growing, symptomatic or the patient wishes. Fibrocystic change/cyclical mastalgia is managed with reassurance, a well-fitting supportive bra, simple analgesia and reduction of caffeine; refractory cases may need specific drug therapy, but most settle once cancer is excluded and the woman is reassured. A cyst is treated by aspiration as above. A duct papilloma causing troublesome bloody discharge is treated by microdochectomy (excision of the affected duct). A phyllodes tumour must be removed by wide local excision with a clear margin (not simple enucleation like a fibroadenoma) because it can recur locally and a minority are malignant. Breast infections are the active surgical part: early lactational mastitis/abscess is treated with anti-staphylococcal antibiotics (e.g. flucloxacillin), continued breast emptying (encourage breastfeeding or expression — do not stop), and analgesia; an established abscess is drained, preferably by ultrasound-guided needle aspiration (repeated as needed), reserving incision and drainage for large, multiloculated or skin-threatening collections. Always send pus for culture, and remember that a non-lactational abscess or a non-resolving 'abscess' in an older woman must be investigated to exclude inflammatory carcinoma.
Management of Lactational Breast Abscess
- Fibroadenoma: observe/reassure if small & benign; excise if large, growing or symptomatic.
- Cyst: aspirate; investigate if bloody, residual or rapidly refilling.
- Duct papilloma: microdochectomy.
- Phyllodes: wide local excision (NOT enucleation) — risk of recurrence/malignancy.
- Breast abscess: antibiotics + continued emptying + USG-guided aspiration or I&D; culture pus; exclude inflammatory cancer if atypical.
CLINICAL PEARL
Two traps protect patients and reputations. First, treat a phyllodes tumour by WIDE local excision with a clear margin, not the simple enucleation used for a fibroadenoma — it can recur locally and a minority are malignant, so the operation differs even though the lump can feel like a big fibroadenoma. Second, never accept a 'breast abscess' uncritically in a non-lactating or older woman: a non-resolving inflammatory mass may be inflammatory breast carcinoma, so any abscess that does not settle, or one outside lactation, demands triple assessment. And after aspirating a cyst, a bloodstained aspirate or a residual lump means cancer must be excluded.
Check Your Understanding
Bring the threads together by reasoning through the three patients from the hook. The 22-year-old with a smooth, mobile 'breast mouse' most likely has a fibroadenoma: clinical examination, ultrasound and (if any doubt) core biopsy confirm it, after which a small, concordant lesion can be reassured. The breastfeeding mother with a hot, red, tender, fluctuant swelling has a lactational breast abscess caused by Staphylococcus aureus: she needs anti-staphylococcal antibiotics, continued breast emptying, and ultrasound-guided aspiration or incision and drainage with pus sent for culture. The 60-year-old with a hard, tethered post-trauma lump most likely has fat necrosis, but because it mimics cancer she needs full triple assessment to prove it. Use these to self-test the competency. First, can you classify benign breast disease (ANDI, benign tumours, inflammatory, duct ectasia, fat necrosis) and give the pathogenesis of each? Second, can you describe the typical clinical features and confirm benignity by triple assessment, including the cyst-aspiration rules? Third, can you state the principles of management of each condition, including the practical treatment of a breast abscess and the wide excision required for phyllodes? The questions below check exactly these links.
SELF-CHECK
A breastfeeding woman has a fluctuant, tender, red breast swelling with fever. After starting anti-staphylococcal antibiotics, what is the preferred first method of drainage for an established abscess?
A. Wide local excision of the affected segment
B. Ultrasound-guided needle aspiration (repeated as needed)
C. Stopping breastfeeding immediately and observing
D. Mastectomy
Reveal Answer
Answer: B. Ultrasound-guided needle aspiration (repeated as needed)
An established lactational abscess is preferably drained by ULTRASOUND-GUIDED needle aspiration, repeated as needed, alongside anti-staphylococcal antibiotics and CONTINUED breast emptying (do not stop feeding/expression). Formal incision and drainage is reserved for large, multiloculated or skin-threatening collections. Pus should be cultured, and an atypical or non-resolving 'abscess' must be investigated to exclude inflammatory carcinoma.