Page 10 of 17
SU25.5 | Breast Swelling Palpation — SDL Guide
Learning Objectives
- Describe the indication, governing principles (consent, chaperone, exposure) and applied surface anatomy of breast examination (SU25.5).
- Demonstrate the correct technique to inspect and palpate the breast and regional lymph nodes for a breast swelling on a mannequin or equivalent (SU25.5).
- Interpret and document the characteristics of a breast lump and relate them to benign versus malignant features and triple assessment (SU25.5).
INSTRUCTIONS
Examining the breast for a swelling is a fundamental clinical skill that every doctor must perform cleanly, respectfully and reproducibly. This module teaches the technique step by step — inspection in three positions, systematic palpation, and examination of the regional nodes — and how to interpret and document what you feel. You will practise the routine on a mannequin or simulator until it becomes automatic, building the discipline you will later carry to real patients with consent and a chaperone.
References
- Bailey & Love's Short Practice of Surgery, The Breast (Clinical Examination) (textbook)
- SRB's Manual of Surgery, Examination of the Breast (textbook)
- Sabiston Textbook of Surgery, Diseases of the Breast (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two students examine the same simulated breast lump. The first prods at the lump alone, declares it 'probably fine', and moves on. The second positions the model correctly, inspects in three poses, palpates every quadrant and the axillary tail with the flat of the fingers, then checks the axillary and supraclavicular nodes — and describes the lump precisely: a 2 cm hard, irregular, poorly mobile mass in the upper outer quadrant with overlying skin dimpling, and a palpable axillary node. The lump was identical. What differed was technique and discipline, and only the second examination gathered the information that would protect a real patient. Breast palpation is a skill you build by doing it the same careful way every single time.
WHY THIS MATTERS
A competent breast examination is the entry point to all of breast surgery: it is the 'clinical' arm of triple assessment, it decides who needs urgent imaging and biopsy, and it is performed countless times in surgical, gynaecological and primary-care practice. Done well, it reassures the many women with benign disease and flags the few with cancer; done poorly, it misses lumps, frightens patients, or breaches their dignity. Because the examination is intimate, it also tests your professionalism — consent, chaperoning, gentle exposure and clear communication are as much part of the skill as the palpation itself. Learning the routine now on a mannequin lets you build accurate, respectful technique and reproducible documentation before you ever examine a patient, which is exactly what competency SU25.5 asks you to demonstrate.
RECALL
Recall the anatomy this skill rests on, from the breast anatomy SDL. The breast lies on the chest wall over pectoralis major and is conventionally divided into four quadrants plus the central nipple-areolar zone, with the axillary tail of Spence extending towards the axilla — and most lumps and most cancers arise in the upper outer quadrant and tail, so you must examine them carefully. Recall that Cooper's ligaments, when tethered by cancer, cause skin dimpling, and that lymphatic drainage is chiefly to the axillary nodes — so the examination must always include the regional nodes. Recall too that the examination is the clinical component of triple assessment, feeding into imaging and pathology. Hold on to one idea: the examination is systematic and complete — breast, then axillary tail, then nodes, then the other side — never just the lump.
Why and When to Examine a Breast Swelling
The clinical indication for breast examination is any breast symptom — a lump, pain, nipple discharge, or a skin or nipple change — and it is also part of a general clinical and screening assessment in appropriate settings. The purpose of palpating a breast swelling is specific: to detect any mass, to characterise it accurately, and to decide how urgently it must be investigated, because the examination is the clinical arm of triple assessment. A careful examination answers several practical questions at once — is there really a discrete lump or only generalised nodularity; where is it and how big; does it feel benign (smooth, mobile) or suspicious (hard, irregular, fixed); are there red-flag skin or nipple signs; and are the regional lymph nodes involved. The findings then drive the next step: a clearly benign-feeling lump in a young woman still needs imaging to confirm, while a hard, fixed, node-positive lump needs urgent imaging and biopsy. Understanding why you examine — to gather the information that, combined with imaging and pathology, separates benign from malignant disease — is what makes the technique purposeful rather than a ritual. This relevance frames every later step: the anatomy tells you where to feel, the technique tells you how, interpretation tells you what it means, and practice builds the reliability.
Anatomy and Governing Principles of Breast Examination
Good technique combines surface anatomy with professional principles, and both must be in place before you touch the breast. The applied surface anatomy is simple and structures the whole examination: divide each breast into four quadrants — upper outer, upper inner, lower outer, lower inner — plus the central nipple-areolar complex, and remember the axillary tail running up towards the axilla; the upper outer quadrant and axillary tail hold the most glandular tissue and the majority of lumps, so they need the most attention. The governing professional principles are non-negotiable. First, obtain informed consent and explain what you will do and why. Second, offer and use a chaperone, and document their presence. Third, ensure privacy, warmth and dignity, exposing the chest only as needed and keeping the patient covered between steps. Fourth, examine in a good light, with the patient first sitting (for inspection) and then lying (for palpation). Fifth, examine both breasts and the regional nodes, comparing sides, and always start with the patient's account of where the lump is. Finally, be systematic and gentle — a fixed routine ensures nothing is missed and minimises discomfort. These principles are practised even on a mannequin so they become habit before any real patient.
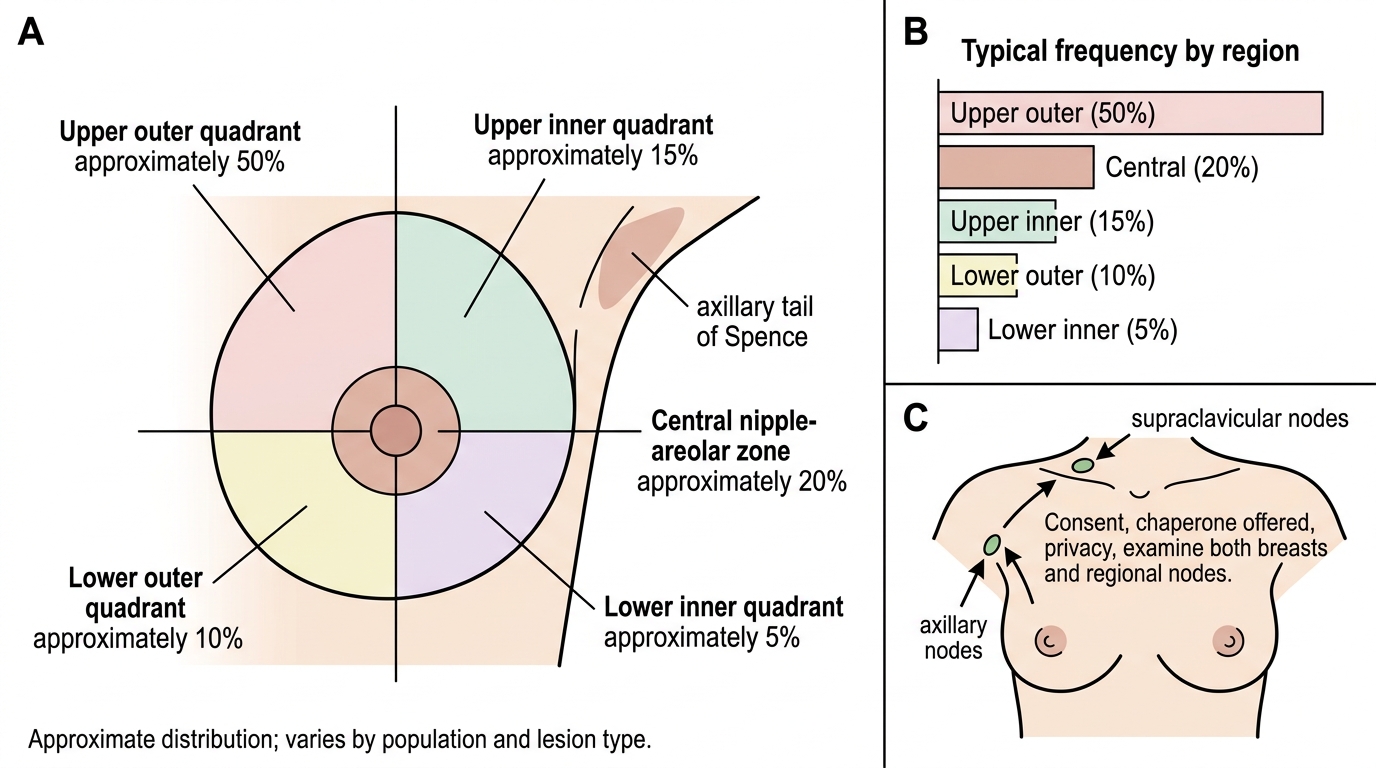
Breast Quadrants and Typical Lump Distribution
SELF-CHECK
Before examining a patient's breast in clinical practice, which professional step is essential?
A. Examine only the lump the patient points to, to save time
B. Obtain informed consent and offer a chaperone, ensuring privacy and dignity
C. Expose both breasts fully for the entire consultation
D. Skip the unaffected breast and the lymph nodes
Reveal Answer
Answer: B. Obtain informed consent and offer a chaperone, ensuring privacy and dignity
Breast examination is intimate, so informed consent, the offer of a chaperone (documented), and attention to privacy, warmth and dignity are essential governing principles. Exposure should be only as needed and the patient kept covered between steps. A complete examination always includes BOTH breasts and the regional (axillary and supraclavicular) nodes, not just the symptomatic lump.
The Technique: Inspection, Palpation and Regional Nodes
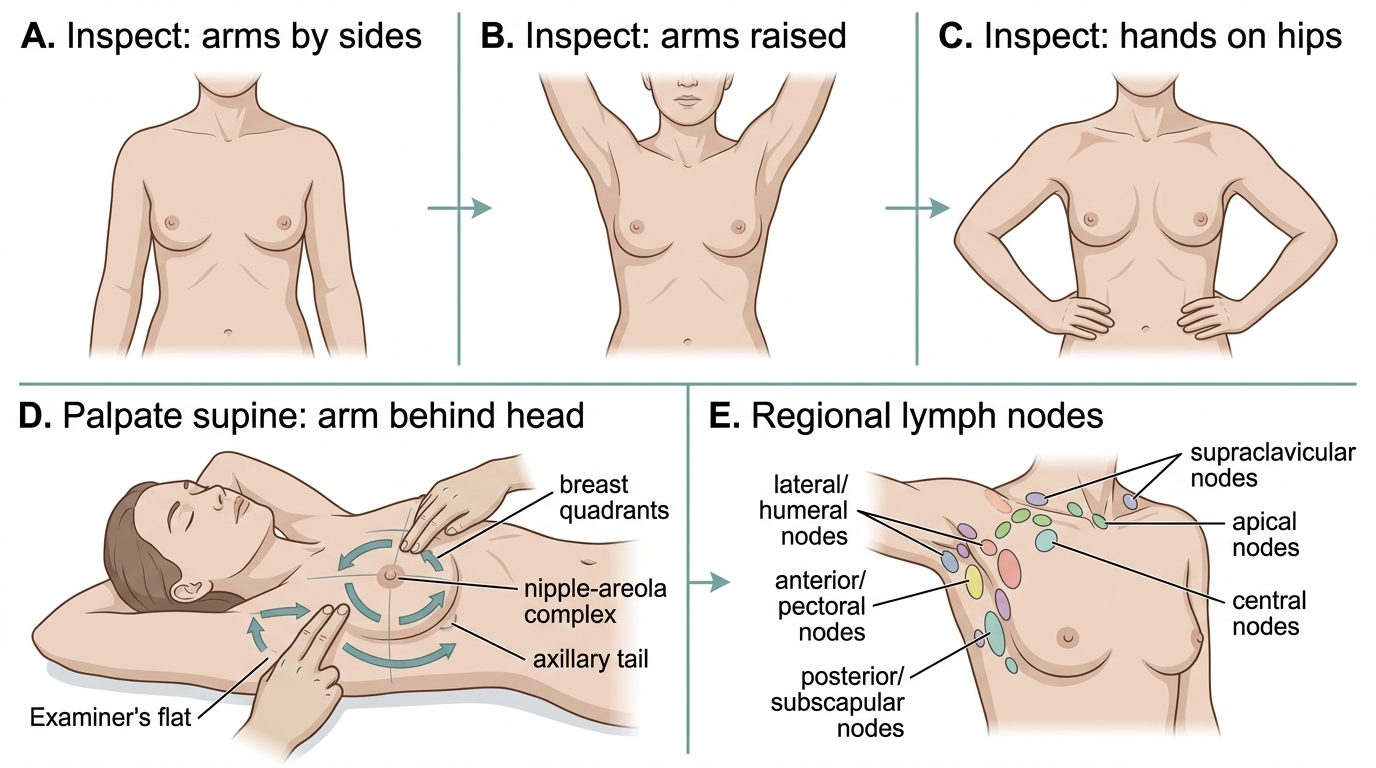
The examination is a fixed three-part sequence performed the same way every time: inspect, palpate the breast, then examine the regional nodes. Inspection is done with the patient sitting and the chest exposed, viewed from the front in three positions to bring out subtle signs: first with the arms relaxed by the sides, then with the arms raised above the head (which can reveal tethering or a fixed mass moving abnormally), and then with the hands pressed firmly on the hips to tense pectoralis major (which accentuates skin dimpling and fixity to the muscle). Look for asymmetry, a visible lump, skin dimpling or puckering, nipple retraction or distortion, an eczematous nipple, ulceration and peau d'orange. Palpation is then performed with the patient lying supine and the arm of the side being examined placed behind the head, which spreads the breast tissue over the chest wall. Using the flat of the fingers (the palmar surface, not the tips), palpate systematically through every quadrant, the nipple-areolar complex, and the axillary tail, with a gentle rotary or strip pattern so no area is missed; gently test the nipple for discharge if indicated. Finally, examine the regional lymph nodes: support the patient's arm and palpate the axilla in its node groups — anterior (pectoral), posterior (subscapular), lateral (humeral), central and apical — and then the supraclavicular fossa. Always examine the contralateral breast for comparison. The same disciplined sequence is rehearsed on the mannequin.
Breast Examination: Inspection, Palpation, and Regional Nodes
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
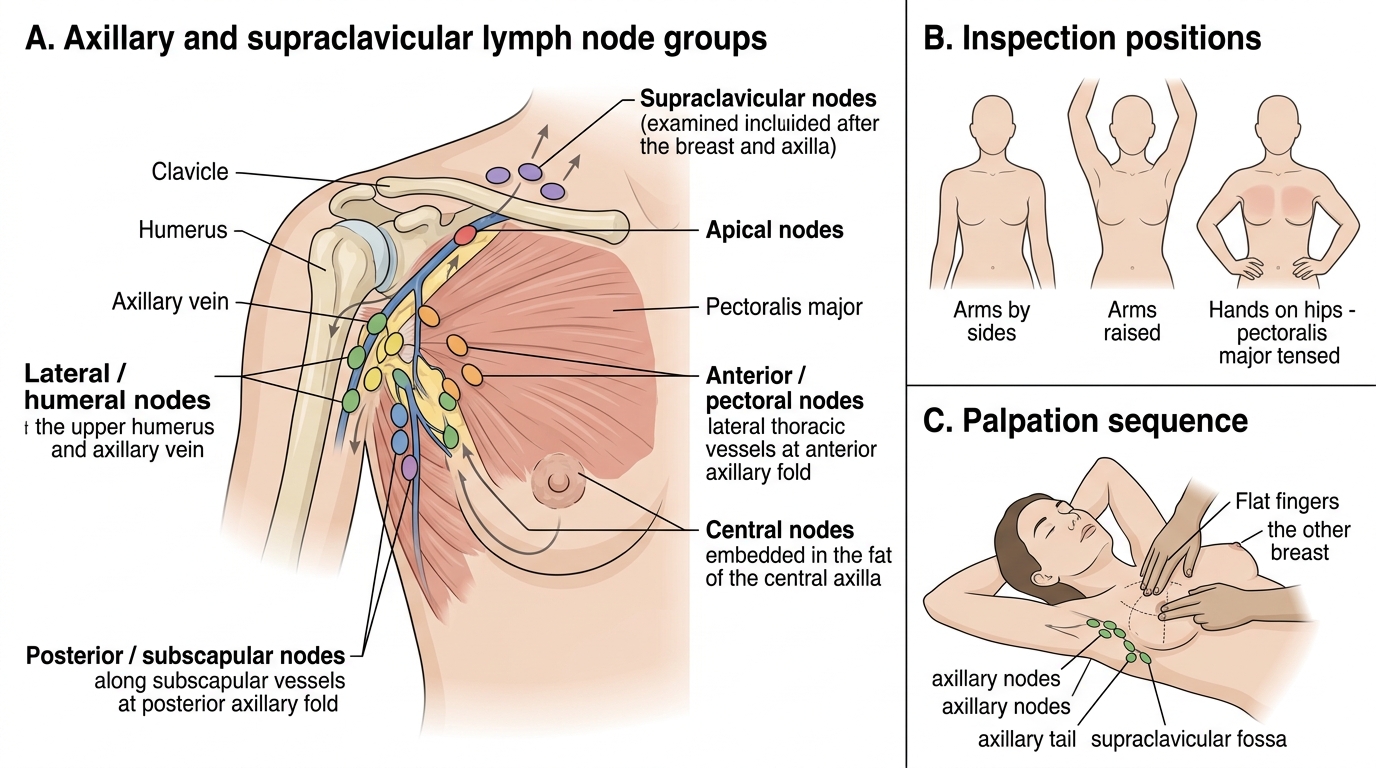
Axillary and Supraclavicular Lymph Nodes in Breast Examination
- Inspect (sitting): arms by sides → arms raised → hands on hips (tense pectoralis major).
- Palpate (supine, arm behind head): flat of fingers through all quadrants + nipple-areola + axillary tail.
- Nodes: axillary groups (anterior, posterior, lateral, central, apical) + supraclavicular; then the other breast.