Page 2 of 11
SU2.1-2 | Shock Pathophysiology and Resuscitation — SDL Guide (Part 2)
Principles of Resuscitation and Fluid Replacement
Resuscitation rests on two simultaneous principles: restore tissue perfusion and treat the underlying cause — and the two must happen together, because fluid alone will never resuscitate a patient who is still bleeding or whose heart is being compressed by tamponade. For hypovolaemic and haemorrhagic shock the volume strategy is staged: begin with a warmed balanced crystalloid such as Ringer's lactate to refill the vascular compartment, but recognise early that a patient who is bleeding needs blood, not endless crystalloid, and in major haemorrhage move quickly to a balanced, haemostatic transfusion of packed red cells, fresh frozen plasma and platelets in roughly equal (1:1:1) proportions to replace what is being lost and to correct the developing coagulopathy. Two modern principles temper the old habit of pouring in large fluid volumes. Permissive (hypotensive) resuscitation accepts a lower target blood pressure — enough for a palpable radial pulse, a systolic around 80–90 mmHg, and an alert patient — in the patient with uncontrolled haemorrhage until the bleeding is surgically controlled, because driving the pressure up before haemostasis simply dislodges clot, dilutes clotting factors and worsens bleeding. Damage-control resuscitation combines this restrained, blood-product-led approach with aggressive prevention of the lethal triad of hypothermia, acidosis and coagulopathy and early surgical or radiological control of the source. Treatment then diverges by cause, and this is the heart of cause-directed therapy: obstructive shock is relieved mechanically (needle/finger decompression and a chest drain for tension pneumothorax, pericardiocentesis or surgery for tamponade) — fluid is only a holding measure; anaphylactic shock is treated with prompt intramuscular adrenaline plus fluids, oxygen and adjuncts; cardiogenic shock needs cautious fluids and inotropic/vasopressor support with treatment of the cause (e.g. revascularisation), since flooding the failing heart worsens pulmonary oedema; and septic shock requires generous fluid resuscitation plus early broad-spectrum antibiotics and source control, with vasopressors (noradrenaline) if hypotension persists. The endpoints that confirm success are the reversal of the very signs you used to recognise shock — a falling heart rate, a restored blood pressure and mentation, a warming periphery, a clearing lactate and a urine output climbing back above 0.5 mL/kg/h.
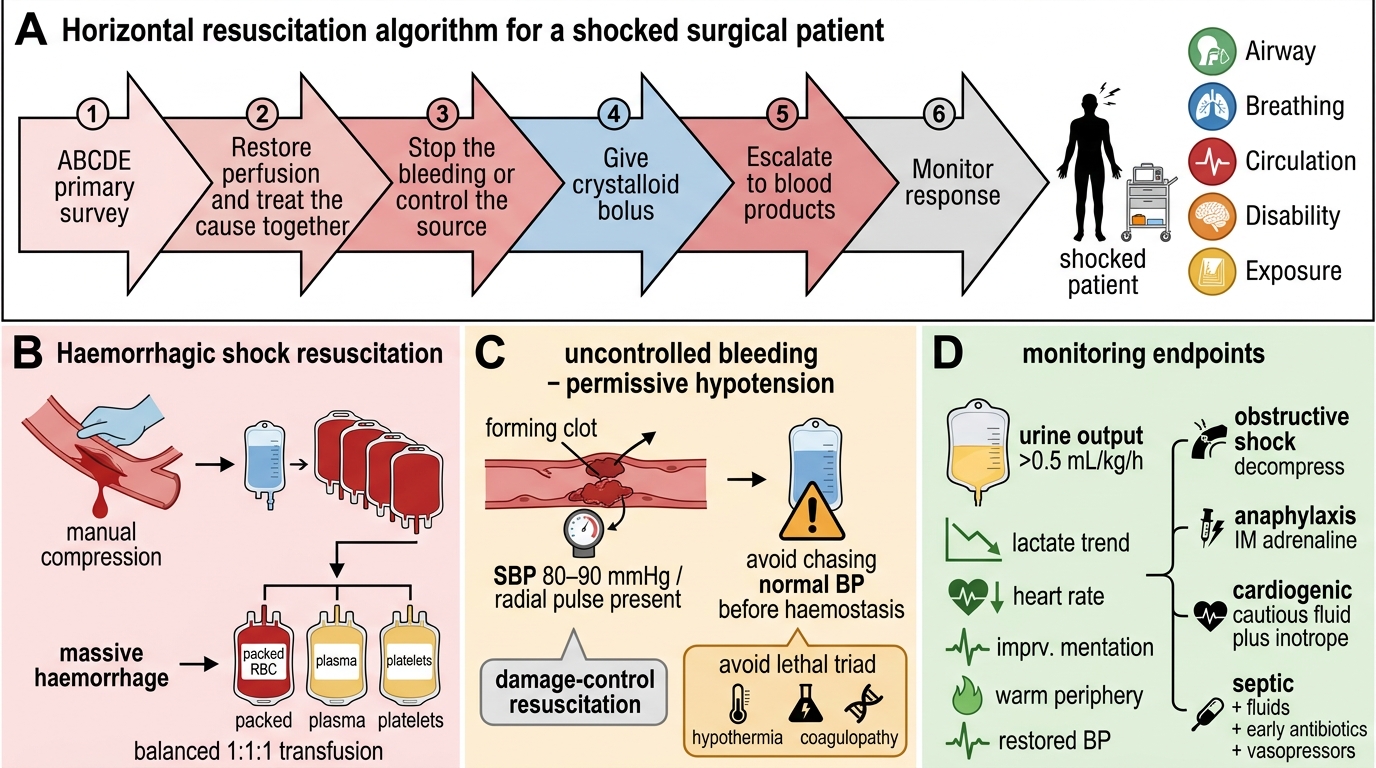
Resuscitation Algorithm for the Shocked Surgical Patient
- Restore perfusion + treat the cause — always together.
- Haemorrhage: crystalloid first, then blood; balanced 1:1:1 in massive transfusion.
- Uncontrolled bleeding: permissive hypotension (radial pulse / SBP ~80–90) until haemostasis; damage-control resuscitation; avoid the lethal triad.
- Cause-specific: obstructive → decompress; anaphylaxis → IM adrenaline; cardiogenic → cautious fluid + inotropes; septic → fluids + early antibiotics + vasopressors.
- Endpoints: falling HR, restored BP/mentation, warm periphery, clearing lactate, urine >0.5 mL/kg/h.
CLINICAL PEARL
A 'normal' blood pressure in a tachycardic, oliguric, cold patient is a TRAP — it is compensated shock, not stability. Treat the trajectory, not the snapshot: a heart rate that keeps climbing and a lactate that fails to clear despite fluids mean the patient is still under-resuscitated or still bleeding, and the answer is to find and stop the source (and give blood), not to give yet another bag of crystalloid. In uncontrolled haemorrhage, chasing a textbook blood pressure with crystalloid before the bleeding is stopped actively harms the patient by dislodging clot and diluting clotting factors.
Check Your Understanding
Bring the threads together by reasoning back through two patients. Return first to the motorcyclist from the hook: his tachycardia, narrowed pulse pressure, confusion and oliguria in the face of a near-normal systolic pressure place him in compensated (Class II–III) haemorrhagic shock — the correct response is the ABCDE survey, two large-bore lines, a hunt for the bleeding source (chest, abdomen, pelvis, long bones, 'on the floor'), crystalloid moving rapidly to balanced blood-product transfusion, permissive hypotension until the surgeon or interventional radiologist controls the source, and relentless monitoring of his urine output and lactate. Now contrast a 70-year-old woman admitted warm, flushed and confused with a low blood pressure, a high lactate and a urinary catheter draining cloudy urine: this is distributive (septic) shock, where the first moves are fluids plus early broad-spectrum antibiotics, cultures and source control, escalating to noradrenaline if she stays hypotensive — pouring in fluid alone would be a mistake. Use these to self-test the competencies this module covers. First, can you recognise shock from its bedside signs and explain why hypotension is a late sign? Second, can you name the four mechanistic types, place septic/anaphylactic/neurogenic correctly under distributive and tamponade/tension pneumothorax under obstructive, and give the haemodynamic profile of each? Third, can you state the principles of resuscitation — crystalloid then blood, balanced 1:1:1 transfusion, permissive hypotension in uncontrolled haemorrhage, damage-control resuscitation, cause-specific treatment, and the monitored endpoints of urine output and lactate? The questions that follow check exactly these links.
SELF-CHECK
A young man with uncontrolled intra-abdominal haemorrhage from blunt trauma is awaiting laparotomy. Before the bleeding is surgically controlled, which resuscitation strategy is most appropriate?
A. Aggressive crystalloid boluses to drive the systolic blood pressure above 120 mmHg
B. Permissive hypotension with balanced blood products, targeting a palpable radial pulse until haemostasis is achieved
C. Withhold all fluids and blood until the patient reaches the operating theatre
D. Vasopressors as first-line to maintain a normal blood pressure
Reveal Answer
Answer: B. Permissive hypotension with balanced blood products, targeting a palpable radial pulse until haemostasis is achieved
In UNCONTROLLED haemorrhage the principle is permissive (hypotensive) resuscitation with balanced blood products (1:1:1) as part of damage-control resuscitation: aim for a palpable radial pulse / systolic ~80–90 mmHg and an alert patient until the source is controlled. Driving the pressure up with crystalloid (option A) dislodges clot, dilutes clotting factors and worsens bleeding and the lethal triad. Fluids/blood are not withheld (C), and vasopressors are not first-line for haemorrhagic shock (D).