Page 2 of 17
SU28.1-2 | Hernias — SDL Guide (Part 2)
Principles of Surgical Management
Management is decided by the type of hernia, the symptoms and — above all — whether the hernia is complicated. For an uncomplicated, reducible inguinal hernia, the definitive treatment is surgical repair, because hernias do not resolve and carry a small ongoing risk of obstruction and strangulation; watchful waiting is a reasonable option only for a minimally symptomatic, easily reducible inguinal hernia in a selected adult who understands the risks. A femoral hernia, by contrast, should always be repaired promptly because of its high strangulation risk, even when small and asymptomatic. The modern principle of elective repair is tension-free reinforcement of the wall with a prosthetic mesh. The standard open operation is the Lichtenstein tension-free mesh repair, in which the sac is dealt with (reduced or excised) and a sheet of mesh is laid over the posterior wall of the inguinal canal to buttress it without tension. The alternative is laparoscopic repair — totally extraperitoneal (TEP) or transabdominal preperitoneal (TAPP) — which places the mesh behind the defect; it is particularly favoured for bilateral and recurrent inguinal hernias and gives less postoperative and chronic pain and a quicker return to activity in experienced hands, at the cost of needing general anaesthesia and more specialised skill. A complicated hernia changes everything: an obstructed or strangulated hernia is a surgical emergency requiring resuscitation and urgent operation to relieve the constriction, assess the viability of the contents (and resect non-viable bowel) and repair the defect. Important complications of hernia repair itself include recurrence, chronic groin pain (often from nerve entrapment), seroma or haematoma, wound or mesh infection, and, in men, ischaemic orchitis or testicular atrophy from cord injury — all of which form part of informed consent.
Natural History of Hernia Complications
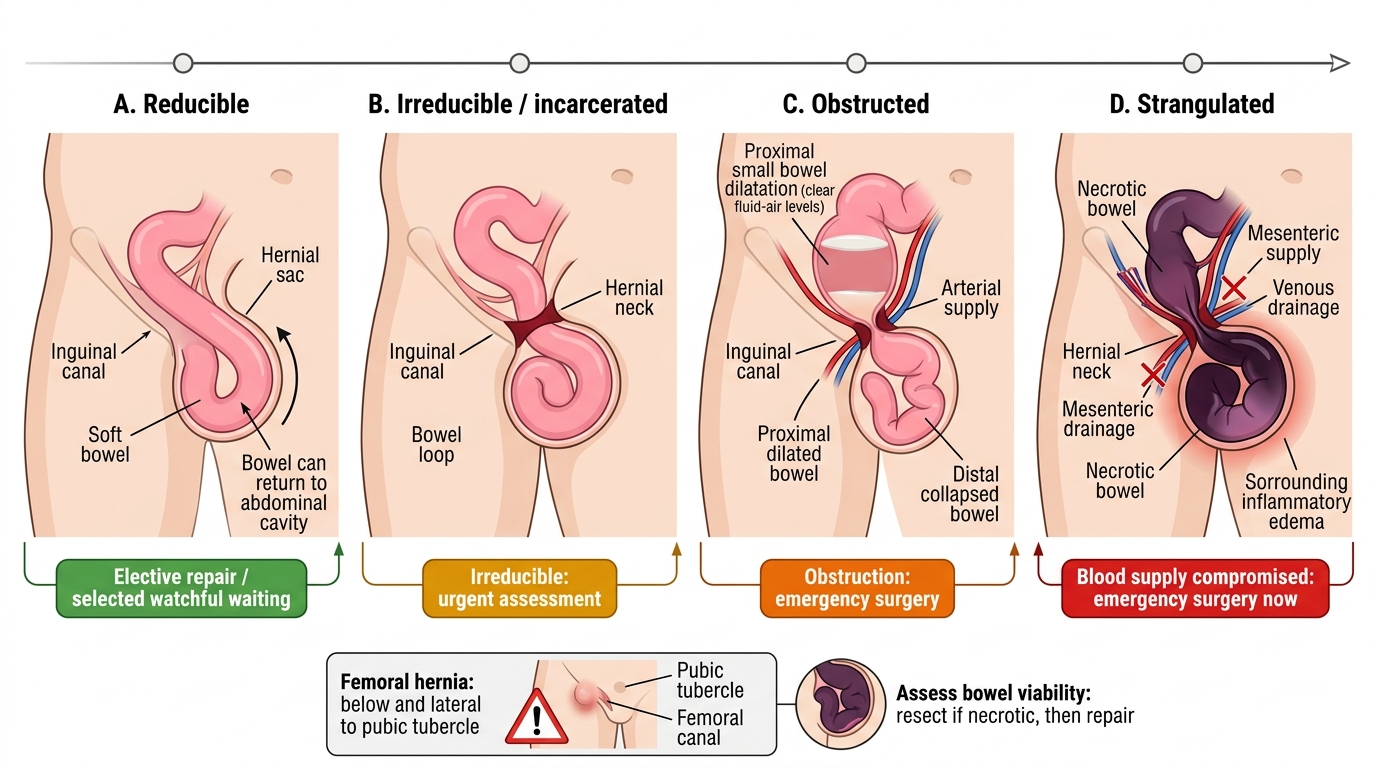
- Reducible inguinal: elective repair; watchful waiting only if minimally symptomatic and selected.
- Femoral: always repair promptly (high strangulation risk).
- Repair: open tension-free mesh (Lichtenstein) or laparoscopic (TEP/TAPP — favoured for bilateral/recurrent).
- Obstructed/strangulated: emergency surgery — relieve constriction, assess bowel viability, resect if necrotic, repair.
CLINICAL PEARL
Always settle the pubic-tubercle question first: a femoral hernia (below and lateral to the pubic tubercle, commoner in women) is easy to miss and the most likely groin hernia to strangulate, so never dismiss a small, tender lump below the groin crease as 'just a node'. And remember the cardinal rule of the acute abdomen: in any patient with intestinal obstruction, examine the hernial orifices — a small strangulated femoral or inguinal hernia is a classic and reversible cause that is missed only because it was not looked for.
Check Your Understanding
Return to the two patients in the hook and reason through them with the framework you now have. The labourer's lump appears on standing, reduces on lying, has a cough impulse and no pain — a reducible inguinal hernia; if it is controlled by occluding the deep ring it is indirect, and it can be managed by elective Lichtenstein or laparoscopic mesh repair, or even watchful waiting if he understands the risks. The elderly woman's small, tender, irreducible lump below the groin crease with vomiting and distension is a strangulated femoral hernia causing intestinal obstruction — a surgical emergency needing resuscitation and urgent operation. Use these to self-test the competencies this module covers. First, can you classify a groin hernia by relating it to the pubic tubercle (inguinal above/medial vs femoral below/lateral) and to the inferior epigastric vessels (indirect lateral vs direct medial), and state which is congenital, which descends to the scrotum and which most often strangulates? Second, can you describe and perform the examination — cough impulse, reduction, and the deep-ring occlusion test — and know that the diagnosis is clinical with ultrasound or CT reserved for doubt? Third, can you state the principles of management, distinguishing elective tension-free mesh repair (open Lichtenstein vs laparoscopic TEP/TAPP) from the emergency management of an obstructed or strangulated hernia? The questions that follow check exactly these links.
SELF-CHECK
A 68-year-old woman presents with a tender, irreducible lump below and lateral to the right pubic tubercle, with vomiting and abdominal distension. Which statement is correct?
A. This is most likely a direct inguinal hernia and can be managed with watchful waiting
B. This is most likely a strangulated femoral hernia requiring emergency surgery
C. Femoral hernias rarely strangulate and surgery can be deferred
D. An expansile cough impulse confirms the lump is benign and reducible
Reveal Answer
Answer: B. This is most likely a strangulated femoral hernia requiring emergency surgery
A lump BELOW and LATERAL to the pubic tubercle is a femoral hernia; femoral hernias are commoner in women and carry the HIGHEST strangulation risk because of their narrow rigid neck. Irreducibility with vomiting and distension indicates obstruction/strangulation — a surgical emergency requiring resuscitation and urgent operation, not watchful waiting.