Page 1 of 14
SU28.5-6 | Esophageal Anatomy and Disorders — SDL Guide
Learning Objectives
- Describe the applied anatomy and physiology of the oesophagus relevant to surgical disease (SU28.5).
- Outline the clinical features, investigations and principles of management of benign oesophageal disorders — GERD with Barrett's, achalasia cardia, and corrosive strictures (SU28.6).
- Outline the clinical features, investigations and principles of management of carcinoma of the oesophagus, including how site determines histological type (SU28.6).
INSTRUCTIONS
Dysphagia — difficulty in swallowing — is a symptom that should never be ignored, because the same complaint can mean a benign motility problem that is curable by a simple operation or a carcinoma that has already become incurable. The oesophagus is a deceptively simple muscular tube, but its anatomy (a deep, segmental blood supply and the absence of a serosa over most of its length) shapes both why its cancers spread early and why its surgery is hazardous. This module connects the applied anatomy and physiology of the oesophagus to a disciplined approach to dysphagia, so that you can separate the achalasia that needs a myotomy from the carcinoma that needs urgent staging, and understand the GERD–Barrett's–adenocarcinoma sequence that links the commonest oesophageal symptom to its most feared complication.
References
- Bailey & Love's Short Practice of Surgery, The Oesophagus (textbook)
- SRB's Manual of Surgery, Oesophagus (textbook)
- Sabiston Textbook of Surgery, Esophagus (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients in your clinic both complain of difficulty swallowing. The first is a 32-year-old woman who, for two years, has had trouble swallowing both solids AND liquids; she regurgitates undigested food at night, sometimes wakes coughing, but her weight is steady and she looks well. The second is a 64-year-old man who, over just three months, has gone from struggling with meat and bread to managing only soup; he has lost six kilograms and now finds even liquids hard. The same word — dysphagia — describes both, yet the first story points to a benign muscle that has forgotten how to relax, and the second to a tumour narrowing the lumen from within. Your task is to read the pattern of the dysphagia, choose the right investigation, and act before a curable problem becomes a fatal one.
WHY THIS MATTERS
Dysphagia is one of the few symptoms in surgery that carries an in-built urgency: any patient over forty with new, progressive dysphagia has oesophageal carcinoma until endoscopy proves otherwise. The oesophagus matters surgically out of all proportion to its simple structure, because its segmental blood supply, its lack of a serosal covering over most of its length, and its rich submucosal lymphatics let cancers spread early and make any resection a major undertaking with significant morbidity. At the same time, the commonest oesophageal complaint of all — heartburn from gastro-oesophageal reflux — is the start of a pathway that, through Barrett's metaplasia, leads to the rising incidence of lower-third adenocarcinoma. Understanding the oesophagus therefore lets you reassure and treat the many with benign disease while catching the few with cancer early, and it underpins a classic clinical examination short case.
RECALL
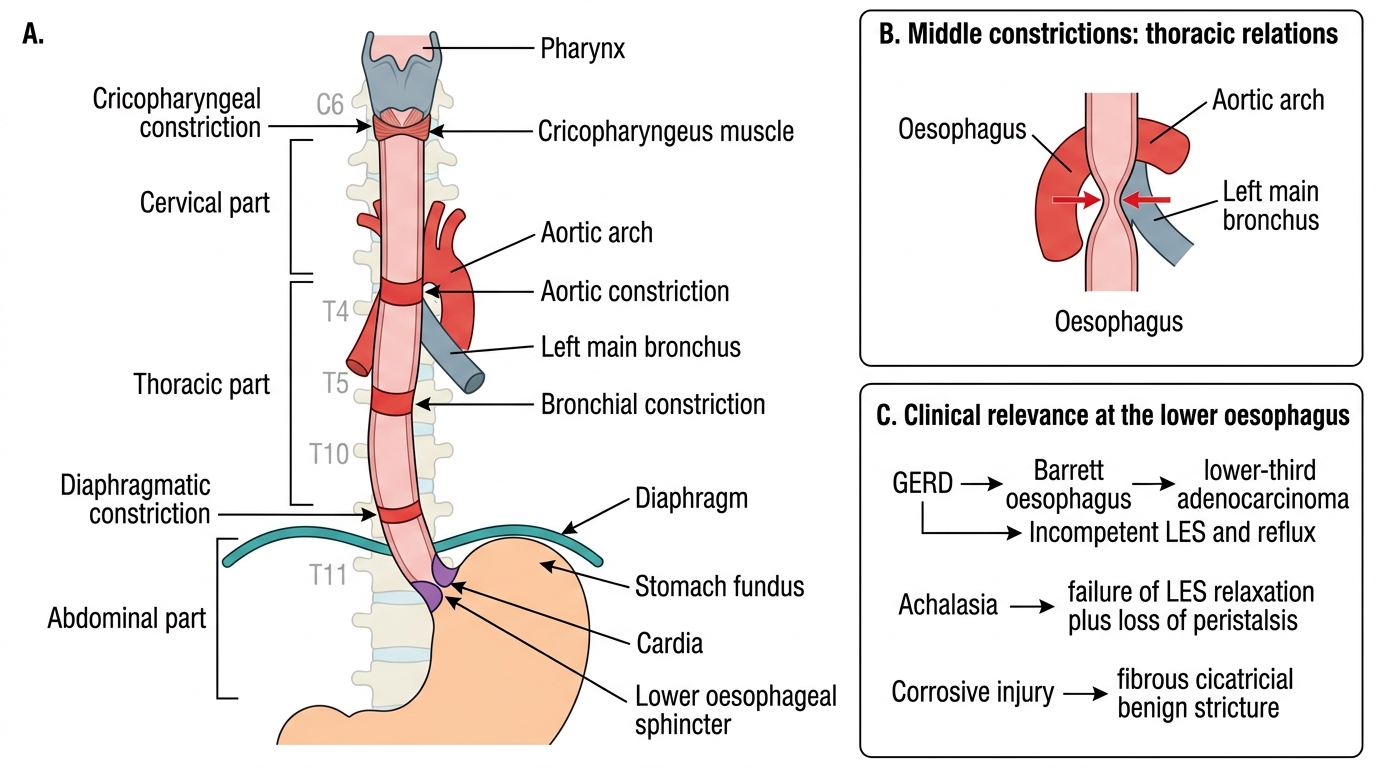
Recall a few foundations before we build on them. From anatomy: the oesophagus is a roughly 25 cm muscular tube running from the cricopharyngeus (at the level of C6) to the cardia of the stomach, with cervical, thoracic and abdominal parts and three normal constrictions — at its origin (cricopharyngeal), where the aortic arch and left main bronchus cross it, and where it pierces the diaphragm. Its upper third is striated muscle and its lower third smooth muscle. Crucially it has a segmental blood supply (inferior thyroid, bronchial and direct aortic branches, and the left gastric artery) and, over most of its length, no serosal covering — both facts matter for surgery and for cancer spread. From physiology: swallowing is a coordinated peristaltic wave, and the lower oesophageal sphincter (LES) is a physiological high-pressure zone that relaxes to let a bolus pass and stays closed to prevent reflux. Hold on to the LES in particular: its failure to relax causes achalasia, and its incompetence causes reflux.
The Patient with Dysphagia
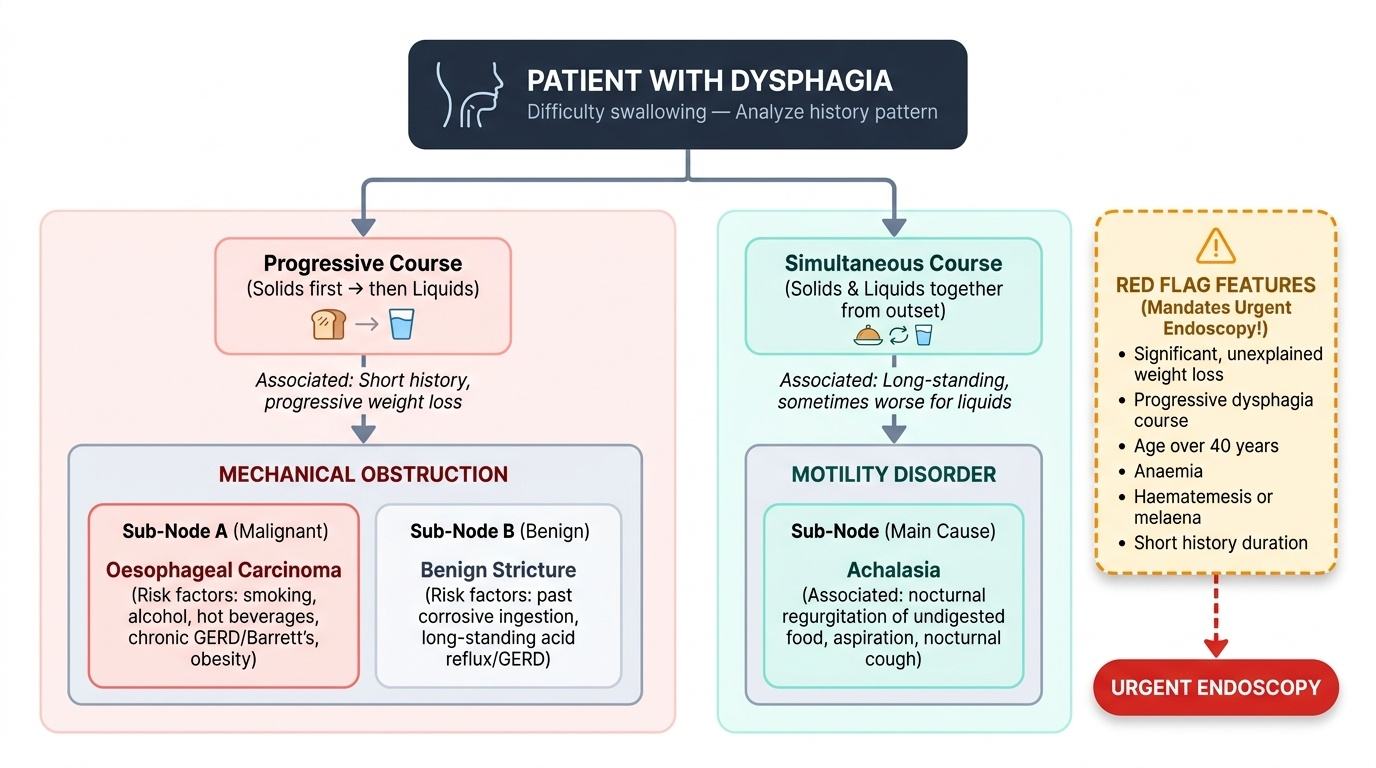
Dysphagia — difficulty in swallowing — is the cardinal symptom of oesophageal disease, and the pattern of the dysphagia is the single most useful piece of history. The first question is what the patient struggles with. Dysphagia that is progressive, beginning with solids (meat, bread) and advancing to liquids, points to a mechanical, lumen-narrowing cause — most worryingly a carcinoma, but also a benign stricture. By contrast, dysphagia to both solids and liquids from the outset, often long-standing and sometimes paradoxically worse for liquids, points to a motility disorder such as achalasia. Always screen for red-flag (alarm) features that mandate urgent endoscopy: significant weight loss, progressive dysphagia, age over forty, anaemia, haematemesis or melaena, and a short history. Ask about associated symptoms — regurgitation of undigested food (achalasia, often nocturnal with aspiration and a cough), long-standing heartburn and acid reflux (GERD, the soil for Barrett's), odynophagia (painful swallowing, suggesting ulceration or candidiasis), and hoarseness (recurrent laryngeal nerve involvement by tumour). Finally, ask about risk factors: for squamous carcinoma, smoking, alcohol, very hot beverages, and a past corrosive (acid/alkali) ingestion causing a stricture; for adenocarcinoma, chronic reflux, Barrett's oesophagus and obesity. This structured history already separates the benign from the malignant before any investigation is requested.
Provided image
- Solids → liquids, progressive, weight loss: mechanical/malignant (carcinoma, stricture).
- Solids and liquids together from the outset: motility disorder (achalasia).
- Red flags (urgent endoscopy): weight loss, progressive course, age >40, anaemia, haematemesis/melaena.
Applied Anatomy, Physiology and the Basis of Oesophageal Disease
Safe understanding of oesophageal disease begins with its applied anatomy. The three constrictions (cricopharyngeal, aortic/bronchial, and diaphragmatic) are where swallowed foreign bodies lodge and where corrosives cause the deepest burns and later strictures. The segmental blood supply (inferior thyroid artery to the cervical part, bronchial and direct aortic branches to the thoracic part, and branches of the left gastric and inferior phrenic arteries to the abdominal part) and the absence of a serosa over the thoracic oesophagus together explain why anastomoses leak and why tumour spreads beyond the wall early. Physiologically the lower oesophageal sphincter (LES) must relax to admit a bolus and stay shut between swallows. From this anatomy and physiology the major diseases follow. In gastro-oesophageal reflux disease (GERD), an incompetent LES allows acid reflux, producing heartburn and oesophagitis; chronic reflux drives Barrett's oesophagus, a change of the normal squamous lining to columnar (intestinal) metaplasia in the lower oesophagus — a premalignant lesion that follows a metaplasia–dysplasia–carcinoma sequence to adenocarcinoma. In achalasia cardia, there is failure of relaxation of the LES together with loss of normal peristalsis, so food accumulates above a functionally obstructed cardia. Corrosive ingestion burns the mucosa and, on healing, produces a fibrous cicatricial stricture. Carcinoma is determined by site: the upper and middle thirds give squamous cell carcinoma (SCC), while the lower third gives adenocarcinoma arising in Barrett's metaplasia.
Oesophagus: Parts, Constrictions and LES
- GERD → Barrett's → adenocarcinoma: incompetent LES → reflux → columnar metaplasia → lower-third adenocarcinoma.
- Achalasia: failure of LES relaxation + loss of peristalsis (a primary motility disorder).
- Corrosive injury: mucosal burn → fibrous cicatricial stricture (benign).
SELF-CHECK
A 30-year-old has had difficulty swallowing both solids and liquids for two years, with nocturnal regurgitation of undigested food but no weight loss. Which is the most likely underlying defect?
A. A carcinoma narrowing the lumen
B. Failure of relaxation of the lower oesophageal sphincter with loss of peristalsis
C. A corrosive stricture at the cricopharyngeus
D. Columnar metaplasia of the lower oesophagus
Reveal Answer
Answer: B. Failure of relaxation of the lower oesophageal sphincter with loss of peristalsis
Dysphagia to BOTH solids and liquids from the outset, long-standing, with nocturnal regurgitation and preserved weight, is the classic picture of achalasia cardia — failure of LES relaxation with loss of peristalsis. Progressive solids-then-liquids dysphagia with weight loss would instead suggest carcinoma.
Examination and Investigation of Oesophageal Disorders
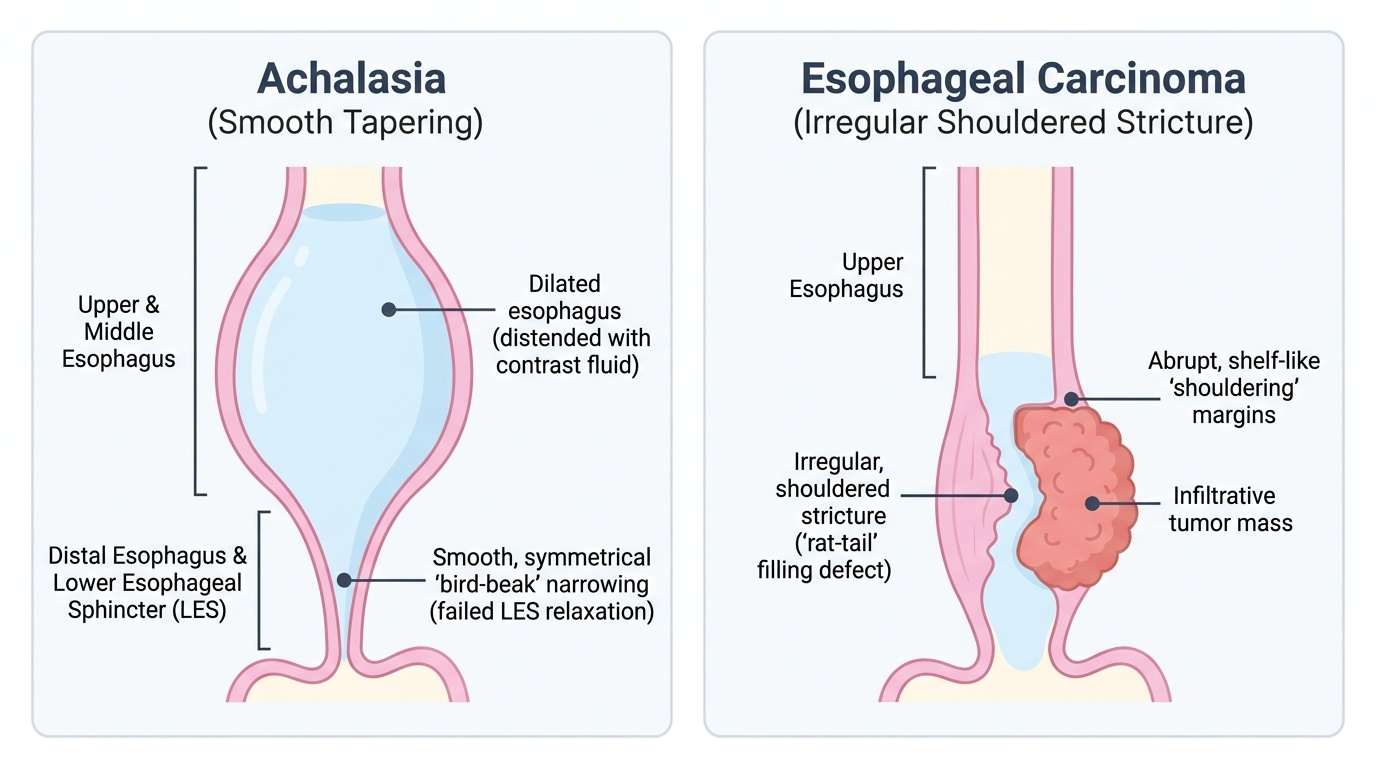
General examination of a patient with oesophageal disease looks for the consequences of the disease as much as its cause: nutritional state and weight loss, anaemia, supraclavicular and cervical lymphadenopathy (notably a left supraclavicular node), hepatomegaly suggesting metastasis, and signs of aspiration at the chest bases. The investigations are then chosen to answer specific questions, and one rule overrides all others: in any adult with new dysphagia, upper gastrointestinal endoscopy (oesophagoscopy) with biopsy is the first and most important investigation, because it both visualises the mucosa and provides tissue to confirm or exclude carcinoma and Barrett's. Barium swallow is complementary and especially useful in motility disorders, showing the smooth, tapering 'bird-beak' (rat-tail) narrowing of achalasia with a dilated oesophagus above, against the irregular, shouldered 'rat-tail' filling defect of a carcinoma. Oesophageal manometry is the gold standard for diagnosing achalasia, demonstrating absent peristalsis with incomplete LES relaxation, and 24-hour pH study confirms and quantifies acid reflux in GERD. Once a carcinoma is confirmed, staging investigations define resectability: CT of the chest and abdomen for distant spread, endoscopic ultrasound (EUS) for depth of wall invasion (T) and local nodes (N), and PET where available for occult metastases.
Provided image
- Endoscopy + biopsy: first-line in all dysphagia — diagnoses carcinoma, Barrett's, oesophagitis.
- Barium swallow: bird-beak (achalasia) vs irregular shouldered stricture (carcinoma).
- Manometry: gold standard for achalasia; pH study for GERD.
- CT + EUS (± PET): staging of confirmed carcinoma (T, N, M).