Page 5 of 14
SU28.{7,9} | Stomach Anatomy and Clinical Examination — SDL Guide (Part 2)
Principles Linking Examination Findings to Management
The value of a disciplined examination is that each positive finding translates directly into an investigation and a management decision. A palpable epigastric mass with weight loss demands urgent upper GI endoscopy with biopsy to confirm carcinoma, followed by CT of the chest, abdomen and pelvis to stage it. A succussion splash establishes gastric outlet obstruction, prompting nasogastric decompression and correction of the resulting metabolic derangement before endoscopy defines whether the cause is a benign scarred ulcer or an antral cancer. The metastatic signs found at the bedside are the most consequential of all, because they can establish incurability without any imaging: a Virchow's node (Troisier's sign), a Sister Mary Joseph nodule, a Blumer's shelf, a Krukenberg tumour, or ascites all indicate advanced, incurable disease, redirecting the plan from attempted curative gastrectomy toward palliation (relief of obstruction, nutrition, and chemotherapy). Conversely, a patient with classic ulcer-type pain, no alarm features and a normal examination can reasonably be tested for Helicobacter pylori and treated medically, with endoscopy reserved for alarm features or treatment failure. The examination, in short, is not a ritual but a decision tool: it places the patient on the benign or malignant pathway and, in the malignant case, often decides between cure and palliation before a single scan is ordered.
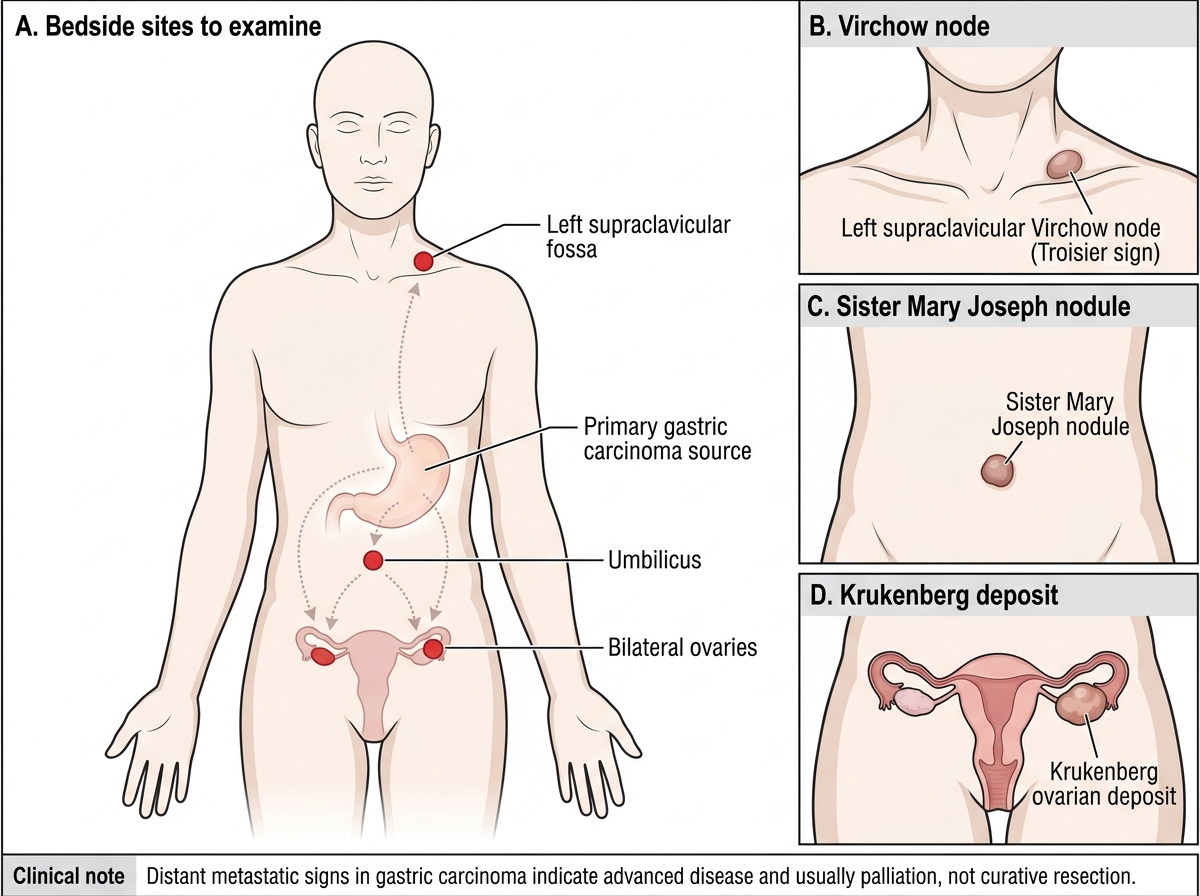
Distant Metastatic Signs in Gastric Carcinoma
- Epigastric mass + weight loss → endoscopy+biopsy → CT staging.
- Succussion splash → gastric outlet obstruction → decompress + correct → endoscopy.
- Virchow's/Sister Mary Joseph/Blumer's shelf/Krukenberg/ascites → advanced disease → palliation, not curative resection.
- Ulcer-type pain, no alarm features → test for H. pylori + treat medically.
CLINICAL PEARL
Always finish the 'abdominal' examination of a stomach patient OUTSIDE the abdomen — at the left supraclavicular fossa, the umbilicus, the rectum and (in women) the pelvis. The left supraclavicular node (Virchow's node, the finding being Troisier's sign), an umbilical Sister Mary Joseph nodule, a hard Blumer's shelf on rectal examination, and a Krukenberg ovarian mass are all transcoelomic or lymphatic metastases of gastric carcinoma, and any one of them can establish incurability at the bedside. Skipping these steps is the commonest way a student misses the single finding that should change the whole management plan.
Check Your Understanding
Bring the threads together by returning to the patient in the hook. The 58-year-old man's enlarged left supraclavicular node (Virchow's node, the finding being Troisier's sign) and hard, irregular epigastric mass together pointed to advanced gastric carcinoma before any scan — the node alone implies distant spread and likely incurability, redirecting management toward staging and palliation rather than attempted cure. Use this to self-test the two competencies this module covers. First, can you describe the applied anatomy — the regions and curvatures, the named arteries (left and right gastric on the lesser curve; left and right gastro-epiploic and short gastric on the greater curve), the lymphatic drainage that governs cancer surgery, and the parietal/chief/G-cell physiology — and say why each matters surgically? Second, can you perform and describe the examination in its correct sequence (general survey, then inspect, palpate, percuss and auscultate the abdomen), elicit an epigastric mass and a succussion splash, and name the metastatic signs (Virchow's/Troisier's, Sister Mary Joseph nodule, Blumer's shelf, Krukenberg tumour) with what each implies? Third, can you translate each finding into the next investigation and the broad management decision? The questions that follow check exactly these links.
SELF-CHECK
An audible succussion splash elicited more than three to four hours after a meal indicates which condition?
A. Ascites from peritoneal metastasis
B. Gastric outlet obstruction with retained gastric contents
C. A perforated peptic ulcer
D. Hepatomegaly from metastasis
Reveal Answer
Answer: B. Gastric outlet obstruction with retained gastric contents
A succussion splash heard well after a meal means the stomach still contains fluid and food it should have emptied — i.e. gastric outlet obstruction (from a scarred pyloric ulcer or an antral carcinoma). It is elicited by rocking the abdomen side to side and listening for the splash of retained gastric contents.