Page 7 of 14
SU28.12 | Diseases of the Biliary System — SDL Guide
Learning Objectives
- Describe the applied anatomy of the biliary system and relate it to safe biliary surgery.
- Recognise the clinical presentations of gallstone disease and its complications, including the classic eponymous signs.
- Outline the investigation and principles of management of biliary disease, including obstructive jaundice and ascending cholangitis.
INSTRUCTIONS
Gallstones are among the commonest of all surgical conditions, and they cause a spectrum of disease from a passing colic to life-threatening sepsis. This SDL builds from the different ways biliary disease presents, through the anatomy and pathology that explain each, to the investigations and the principles of management. As you read, learn the classic clinical signs — Murphy's, Courvoisier's, Charcot's and Reynolds' — not as trivia but as the bedside shortcuts they were designed to be, each pointing you towards a specific diagnosis and a specific next step.
References
- Bailey & Love's Short Practice of Surgery, The Gallbladder and Bile Ducts (textbook)
- SRB's Manual of Surgery, Gallbladder and Bile Ducts (textbook)
- Sabiston Textbook of Surgery, Biliary System (textbook)
Version 2.0 | CBME Content Engine
CLINICAL SCENARIO
A 45-year-old woman has had bouts of pain under her right ribs after fatty meals for months. Tonight the pain has not settled; she is feverish, and her eyes have turned yellow. In the next bed, an older man has noticed that his skin has slowly gone yellow over weeks — but he has no pain at all, and his gallbladder is easily felt as a smooth, non-tender lump. Same yellow colour, two very different stories: one is gallstones obstructing the bile duct with infection brewing, the other is a warning sign of cancer. The biliary tree turns a handful of clinical clues into precise diagnoses, and this session is about reading them.
WHY THIS MATTERS
Gallstone disease is one of the commonest reasons for elective and emergency general surgery, and laparoscopic cholecystectomy is among the most frequently performed operations in the world. Getting biliary disease right matters because the same organ produces problems ranging from a self-limiting colic to ascending cholangitis, which can kill within hours, and because a painless jaundice may be the first sign of a curable-only-if-caught-early cancer. You will need to triage the patient with right upper quadrant pain, interpret an obstructive liver-function pattern, and know when a duct must be cleared urgently — skills used constantly in surgery, medicine and the emergency department.
RECALL
Recall the biliary anatomy from your dissections: bile drains from the liver via the right and left hepatic ducts, which join to form the common hepatic duct; the gallbladder stores and concentrates bile and empties through the cystic duct, which joins the common hepatic duct to form the common bile duct (CBD); the CBD passes behind the duodenum and through the head of the pancreas to open at the ampulla of Vater, guarded by the sphincter of Oddi. Recall too from biochemistry the difference between unconjugated bilirubin (fat-soluble, pre-hepatic) and conjugated bilirubin (water-soluble, excreted in bile) — because obstruction downstream of the liver raises the conjugated fraction and spills it into the urine while pale stools result from absent bile pigment in the gut.
The Patient with Biliary Disease
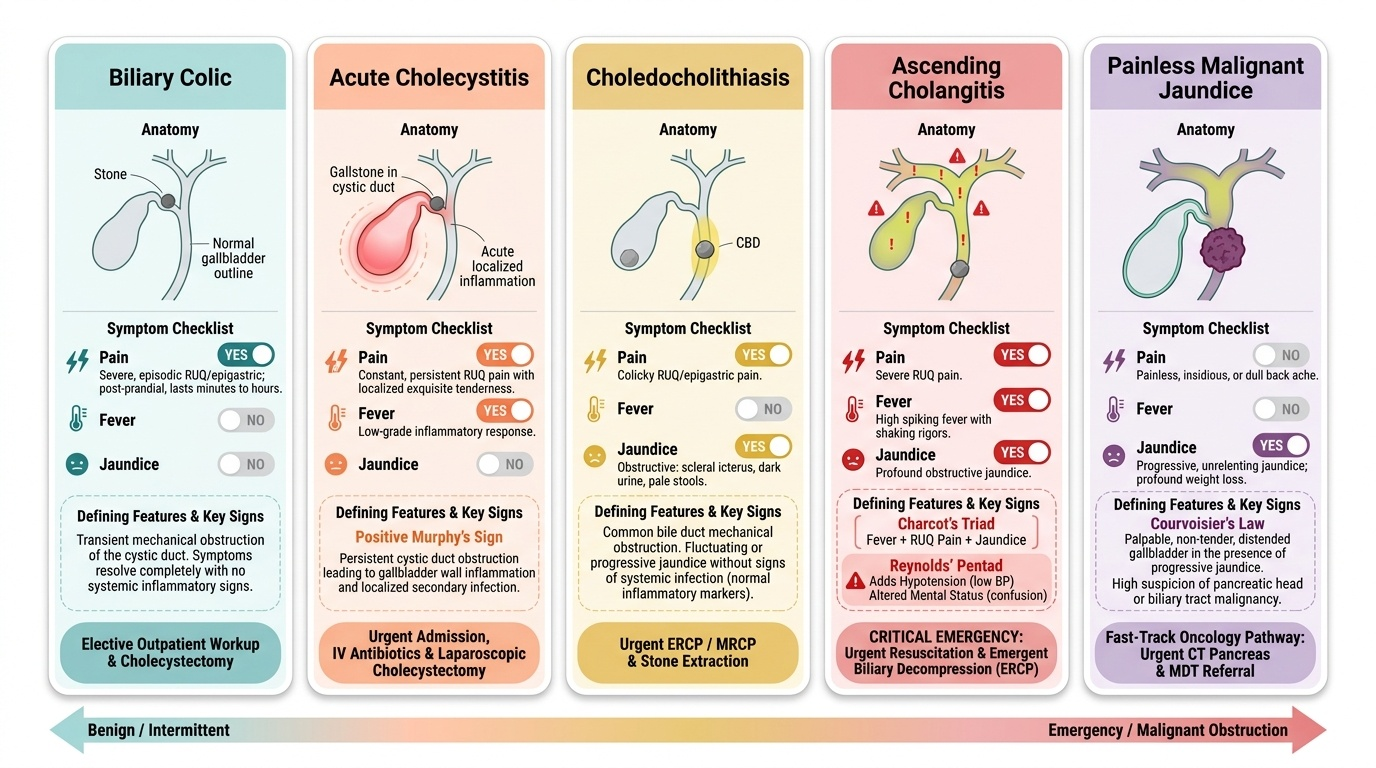
Biliary disease presents along a recognisable spectrum, and identifying which point on that spectrum a patient occupies is the first and most important clinical step. The mildest is biliary colic: severe, gripping right upper quadrant or epigastric pain, often after a fatty meal, lasting minutes to a few hours as a stone transiently obstructs the gallbladder neck or cystic duct, then settling, with no fever and no jaundice. When a stone impacts and the gallbladder becomes inflamed and infected, the picture becomes acute cholecystitis: more persistent RUQ pain, tenderness, fever and a positive Murphy's sign. If a stone passes into and obstructs the common bile duct (choledocholithiasis), the patient develops obstructive jaundice — yellow sclerae, dark urine and pale stools — typically with pain. Add infection of the static, obstructed bile and you get ascending cholangitis, recognised by Charcot's triad of fever (with rigors), right upper quadrant pain and jaundice; if the patient also becomes hypotensive and confused, that is Reynolds pentad, signalling severe, life-threatening cholangitis. Finally, painless, progressive jaundice, especially with a palpable non-tender gallbladder (Courvoisier's law) and weight loss, should raise the suspicion of malignant obstruction such as a periampullary or pancreatic-head cancer or cholangiocarcinoma.
Provided image
Reading the presentation — pain or no pain, fever or no fever, jaundice or no jaundice — already places the patient on this spectrum and tells you how urgently to act. A patient with the full Reynolds pentad is a surgical emergency; a patient with painless jaundice needs urgent investigation for cancer.
Applied Anatomy and the Pathology of Biliary Disease
Safe biliary surgery and a clear understanding of biliary disease both rest on the anatomy of the biliary tree. The critical surgical landmark is Calot's triangle (the cystohepatic triangle), bounded by the cystic duct, the common hepatic duct and the inferior edge of the liver; within it runs the cystic artery. The surgeon must achieve the critical view of safety — clearly identifying the cystic duct and cystic artery as the only two structures entering the gallbladder — before clipping anything, because misidentifying the common bile duct for the cystic duct is the cause of catastrophic bile-duct injury. Downstream, the common bile duct runs to the ampulla of Vater, where the sphincter of Oddi controls bile flow into the duodenum; a stone or tumour here produces obstructive jaundice.
Provided image
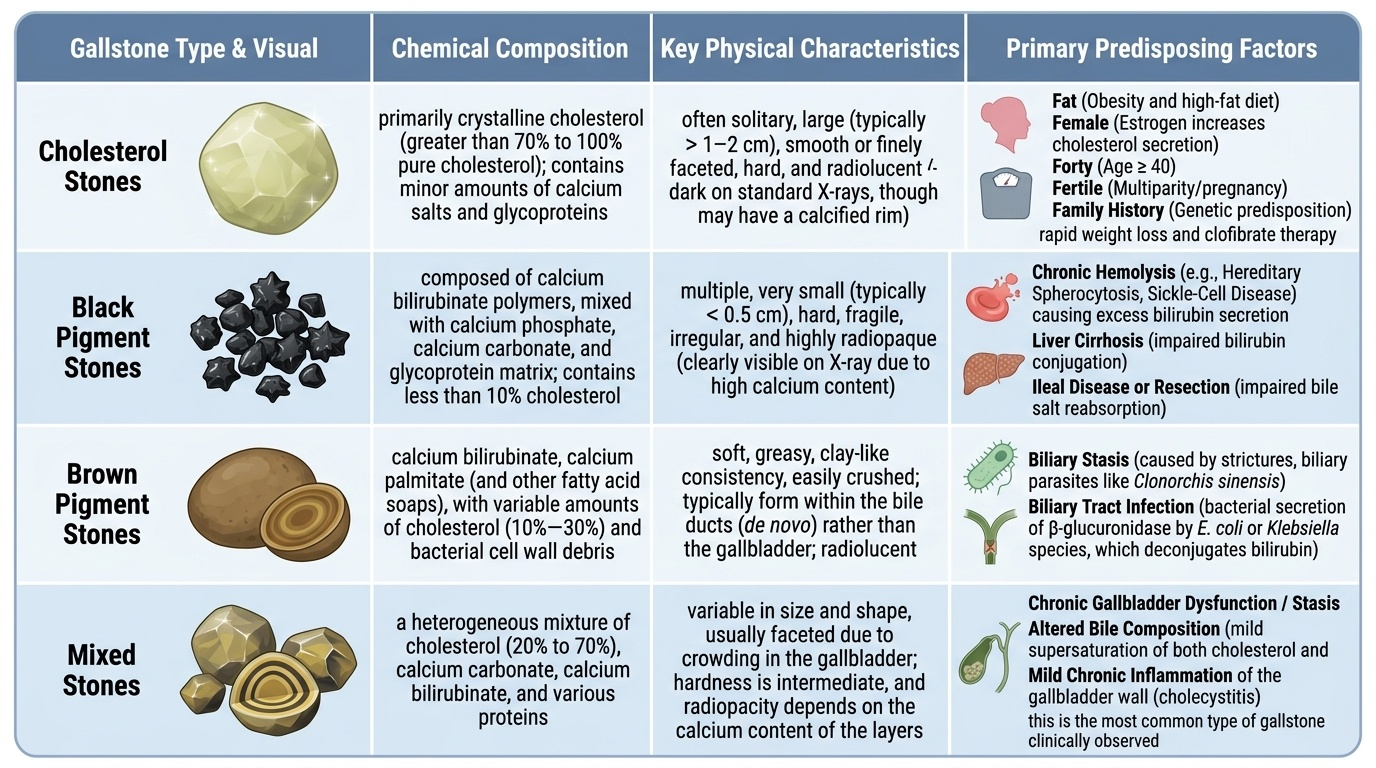
The pathology begins with gallstones, which form when bile becomes lithogenic. Cholesterol stones (the commonest in the West and increasingly common in India) form when bile is supersaturated with cholesterol, classically in the patient described by the 5 F's — Fat, Female, Forty, Fertile and Family history. Pigment stones are of two kinds: black pigment stones, made of calcium bilirubinate and associated with chronic haemolysis (e.g. hereditary spherocytosis, sickle-cell disease) and cirrhosis; and brown pigment stones, associated with biliary infection and stasis. Most stones are in fact mixed. From the stone flow the complications: impaction at the gallbladder neck causes colic; persistent obstruction with inflammation causes acute cholecystitis (and, if pus accumulates, an empyema, or if sterile mucus, a mucocoele); a stone in the CBD causes obstructive jaundice and, with infection, ascending cholangitis; a stone impacted at the ampulla can trigger gallstone pancreatitis. Chronic irritation, and conditions such as a 'porcelain' gallbladder, raise the risk of gallbladder carcinoma.
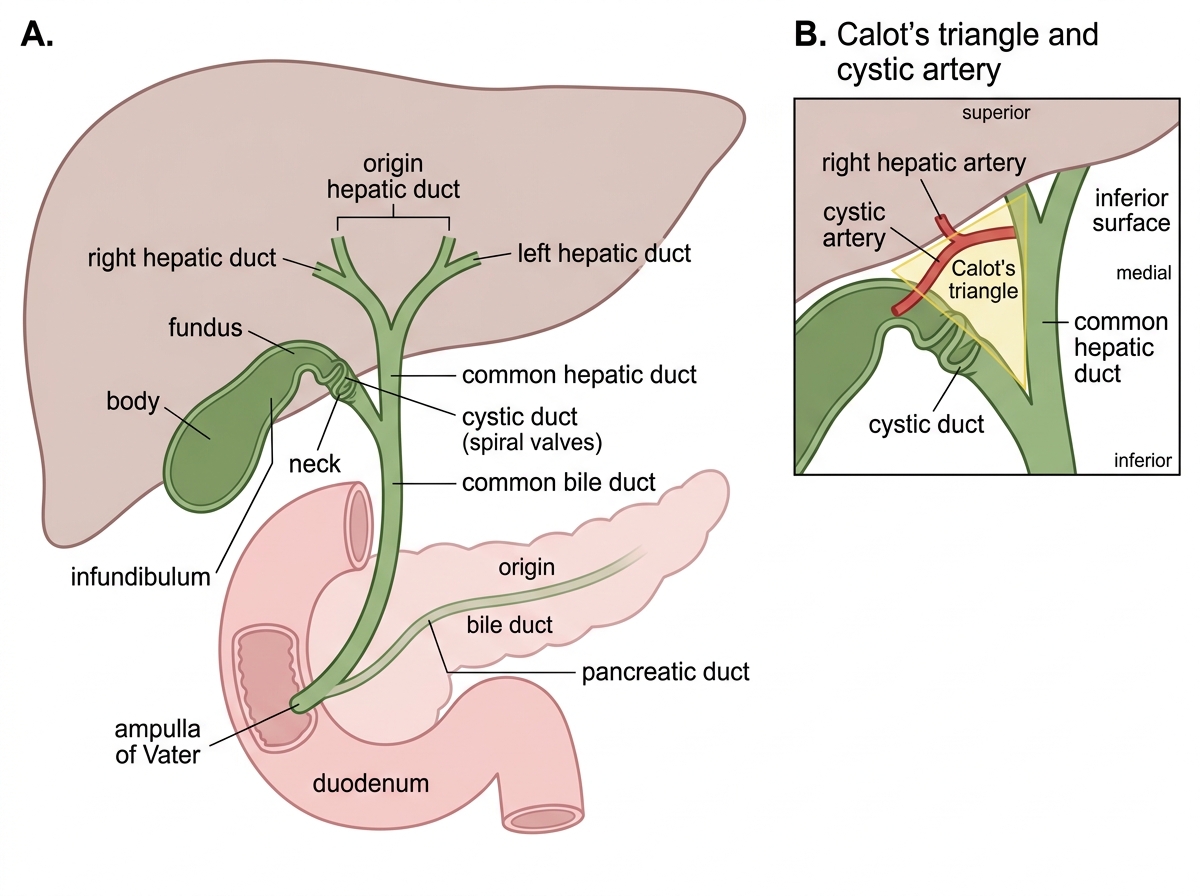
Biliary Tree and Calot's Triangle
SELF-CHECK
A febrile patient with rigors has right upper quadrant pain and jaundice. This combination is known as which eponymous triad, and what does it indicate?
A. Charcot's triad — ascending cholangitis
B. Reynolds pentad — acute pancreatitis
C. Courvoisier's law — gallbladder malignancy
D. Murphy's sign — acute cholecystitis
Reveal Answer
Answer: A. Charcot's triad — ascending cholangitis
Fever (with rigors) + right upper quadrant pain + jaundice is Charcot's triad, indicating ascending cholangitis — infection of obstructed bile. If the patient also develops hypotension and confusion, the picture becomes Reynolds pentad, signalling severe/suppurative cholangitis that needs urgent biliary drainage.
Examination and Investigation
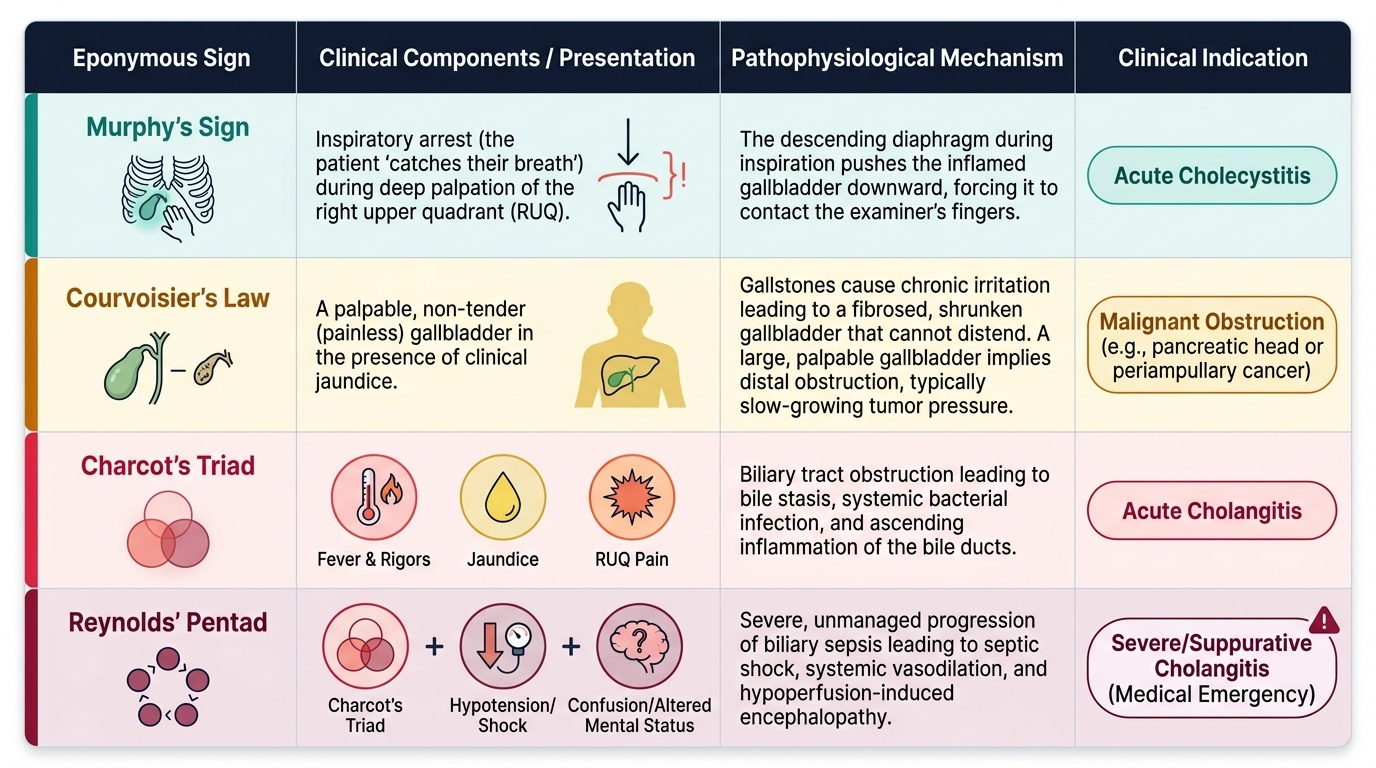
Examination of the biliary patient is rich in classic signs that each point to a diagnosis. In suspected acute cholecystitis you elicit Murphy's sign — ask the patient to breathe in while you press in the right upper quadrant; the descending inflamed gallbladder meets your fingers and the patient catches their breath (arrest of inspiration). In the jaundiced patient you apply Courvoisier's law: a palpable, non-tender gallbladder in the presence of jaundice is unlikely to be due to gallstones — because stones cause a fibrosed, contracted gallbladder — and should instead raise suspicion of malignant obstruction of the distal bile duct (periampullary or pancreatic-head cancer). You also assess for fever, rigors, hypotension and confusion to recognise Charcot's triad and Reynolds pentad. Investigation then confirms the picture. Liver function tests in obstruction show an obstructive (cholestatic) pattern — raised conjugated bilirubin, markedly raised alkaline phosphatase (ALP) and gamma-glutamyl transferase (GGT), with relatively modest transaminase rise. Ultrasound is the first-line imaging: it detects gallstones, gallbladder wall thickening and pericholecystic fluid in cholecystitis, and a dilated common bile duct in obstruction. MRCP (magnetic resonance cholangiopancreatography) is the non-invasive test of choice to image ducts and confirm CBD stones, while ERCP (endoscopic retrograde cholangiopancreatography) is reserved as a mainly therapeutic procedure to clear duct stones, because it carries risks such as pancreatitis. A raised white cell count and inflammatory markers support infection, and amylase/lipase are checked if pancreatitis is suspected.
Provided image