Page 1 of 14
SU28.10 | Liver Abscess, Hydatid Disease, Liver Injury and Liver Tumors — SDL Guide
Learning Objectives
- Describe the applied surgical anatomy of the liver and use it to explain the behaviour of focal liver lesions.
- Differentiate amoebic from pyogenic liver abscess, recognise hydatid disease, and outline the principles of managing each.
- Explain the assessment and management of liver injury and the approach to benign and malignant liver tumours.
INSTRUCTIONS
Right upper quadrant pain with fever, a mass found on a scan, or a liver laceration after blunt trauma — all bring the surgical liver into the clinic and the emergency room. This SDL builds from the patient's presentation, through the anatomy and pathology that explain it, to the investigations and the principles of management. Read it actively: at each step ask yourself why the anatomy makes a lesion behave as it does, and why one abscess is drained, another is never aspirated blindly, and a stable liver injury is often best left alone.
References
- Bailey & Love's Short Practice of Surgery, The Liver (textbook)
- SRB's Manual of Surgery, Liver (textbook)
- Sabiston Textbook of Surgery, The Liver (textbook)
Version 2.0 | CBME Content Engine
CLINICAL SCENARIO
A 34-year-old man returns from working in a rural district with two weeks of fever, drenching sweats and a dull ache under his right ribs that worsens when he lies on his left side. He looks unwell, his liver edge is tender, and an ultrasound shows a single large fluid-filled cavity in the right lobe. Is this an amoebic abscess that will melt away with a tablet, a pyogenic abscess that needs draining, or something that must never be touched with a needle? The same right upper quadrant can hide a curable infection, a dangerous parasitic cyst, a torn liver after a road accident, or a cancer — and telling them apart is what this session is about.
WHY THIS MATTERS
The liver is the commonest solid organ injured in blunt abdominal trauma, amoebic and hydatid disease are endemic across much of India, and hepatocellular carcinoma is rising on the back of viral hepatitis and alcohol. As a clinician you will be expected to resuscitate a bleeding liver, recognise when a febrile traveller has a tropical abscess, avoid the catastrophe of puncturing a hydatid cyst, and refer a suspicious liver mass before it becomes inoperable. These are high-frequency, high-stakes problems where a correct first decision changes the outcome.
RECALL
Recall from anatomy and physiology that the liver has a dual blood supply — roughly three-quarters of its inflow is from the portal vein (carrying nutrient- and toxin-rich blood from the gut) and a quarter from the hepatic artery — and that venous drainage is by the hepatic veins into the inferior vena cava. Remember that gut and appendiceal infection can seed the liver through the portal vein, and that the liver's enormous functional reserve means a large volume can be resected or destroyed before function fails. Keep the lobular architecture and the relationship of the liver to the diaphragm and right pleura in mind — they explain referred shoulder-tip pain and a sympathetic right pleural effusion.
The Patient with Liver Disease: Presentations You Must Recognise
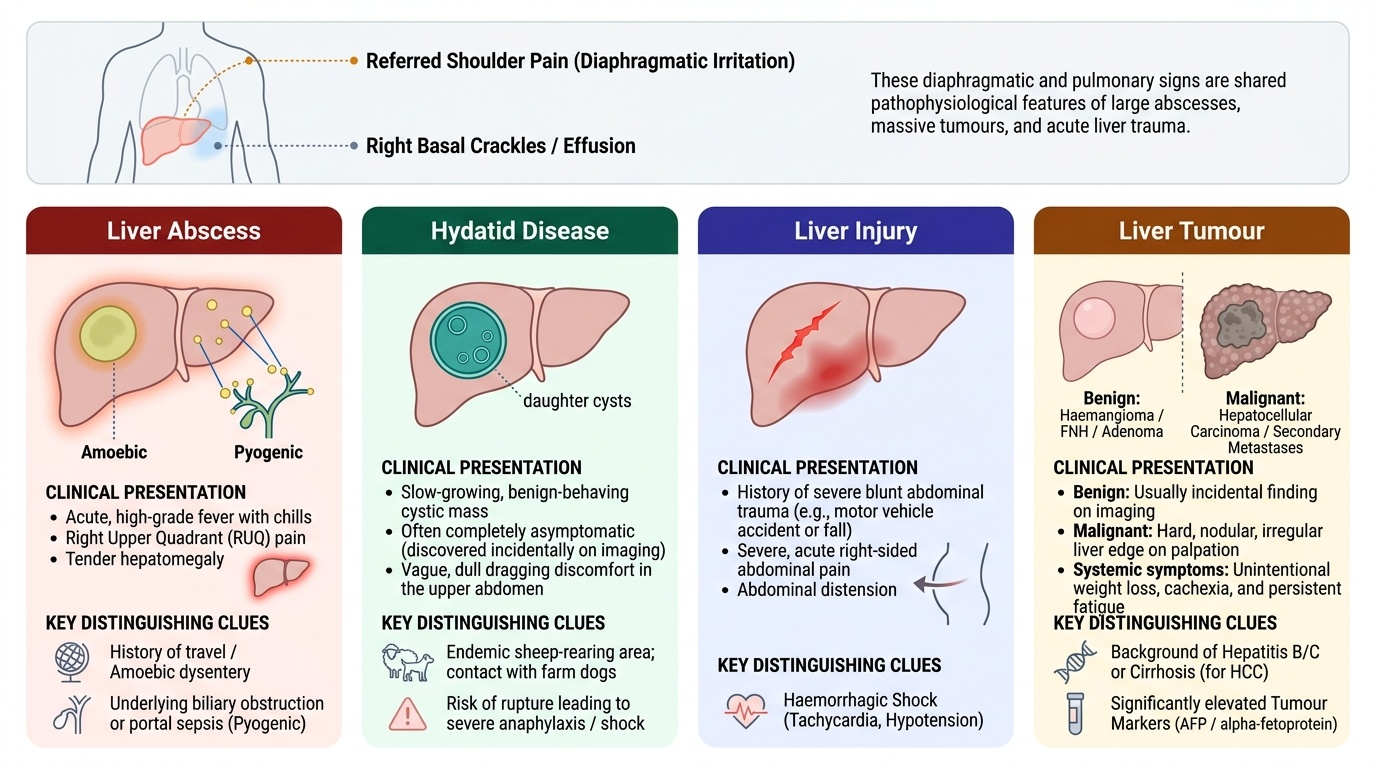
Surgical liver disease announces itself in a handful of recognisable ways, and the pattern of presentation already narrows the differential before any test is ordered. The first is the febrile, painful liver: a patient with fever, right upper quadrant pain, tender hepatomegaly and often a history of dysentery or travel suggests a liver abscess — amoebic or pyogenic. The second is the incidental or slowly enlarging mass: a smooth cystic swelling found on a scan, sometimes with a vague dragging discomfort, which may be a hydatid cyst or a benign tumour, while a hard, irregular liver with weight loss and a background of cirrhosis points to hepatocellular carcinoma. The third is the injured liver: blunt abdominal trauma from a road accident or fall producing right-sided pain, abdominal distension and signs of blood loss. Pain referred to the right shoulder tip (diaphragmatic irritation) and a reactive right basal lung crackle or effusion are clues common to abscess, large tumour and injury alike. A careful history of fever pattern, dysentery, contact with dogs and sheep, alcohol intake, viral hepatitis and trauma mechanism is therefore the most powerful diagnostic tool you have at the bedside, and it should be taken before you reach for imaging.
Provided image
The competency groups these problems together for a reason: they share an organ and an anatomy but demand very different responses. Sorting the presentation into one of these four buckets — abscess, hydatid, injury, tumour — is the first clinical task.
- Liver abscess — fever, RUQ pain, tender hepatomegaly; amoebic (single, right lobe, history of dysentery) vs pyogenic (often multiple, biliary or portal source)
- Hydatid disease — slow-growing cystic mass, often asymptomatic; contact with dogs, sheep-rearing area; risk of rupture and anaphylaxis
- Liver injury — trauma history, haemorrhagic shock, right-sided abdominal pain and distension
- Liver tumours — benign (haemangioma, focal nodular hyperplasia, adenoma) usually incidental; malignant HCC (cirrhosis, hepatitis, weight loss, raised AFP) or secondary metastases
Applied Anatomy and the Pathology of Liver Lesions
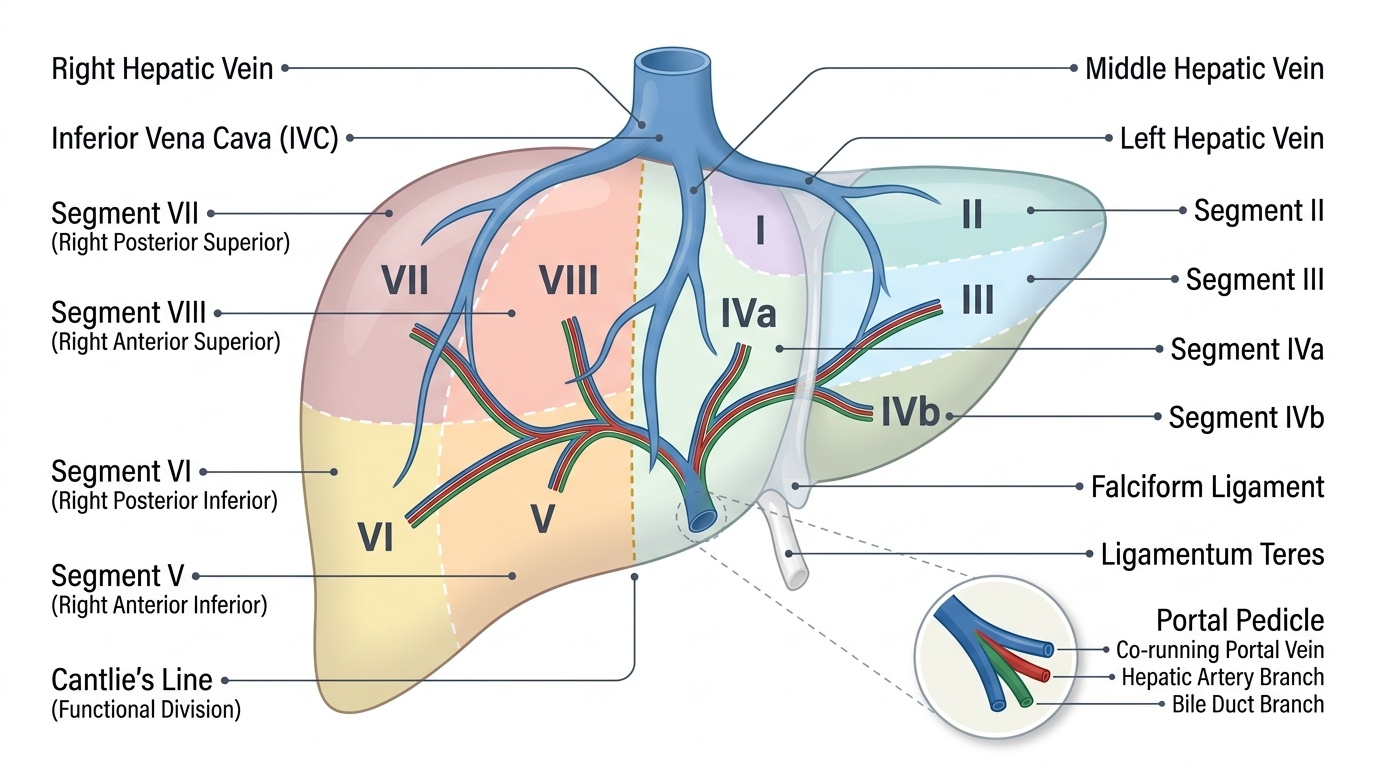
The behaviour and the surgery of every liver lesion follow from the liver's functional anatomy, so this is where understanding must start. The surgically useful map is Couinaud's segmental anatomy, which divides the liver into eight functionally independent segments, each supplied by its own portal pedicle (a branch of the portal vein, hepatic artery and bile duct) and drained by the hepatic veins that run between the segments. Because each segment is self-contained, a surgeon can resect one or several without devascularising the rest — this is the anatomical basis of anatomical liver resection. The old division into right and left lobes by the falciform ligament is a surface marking only; the true functional division runs along the plane of the middle hepatic vein (Cantlie's line). The ligamentum teres within the free edge of the falciform ligament is the remnant of the umbilical vein. The liver's dual blood supply also explains pathology: the portal vein delivers gut organisms to cause pyogenic abscess, while the rich arterial supply makes injured or resected liver bleed briskly.
Provided image
Provided image
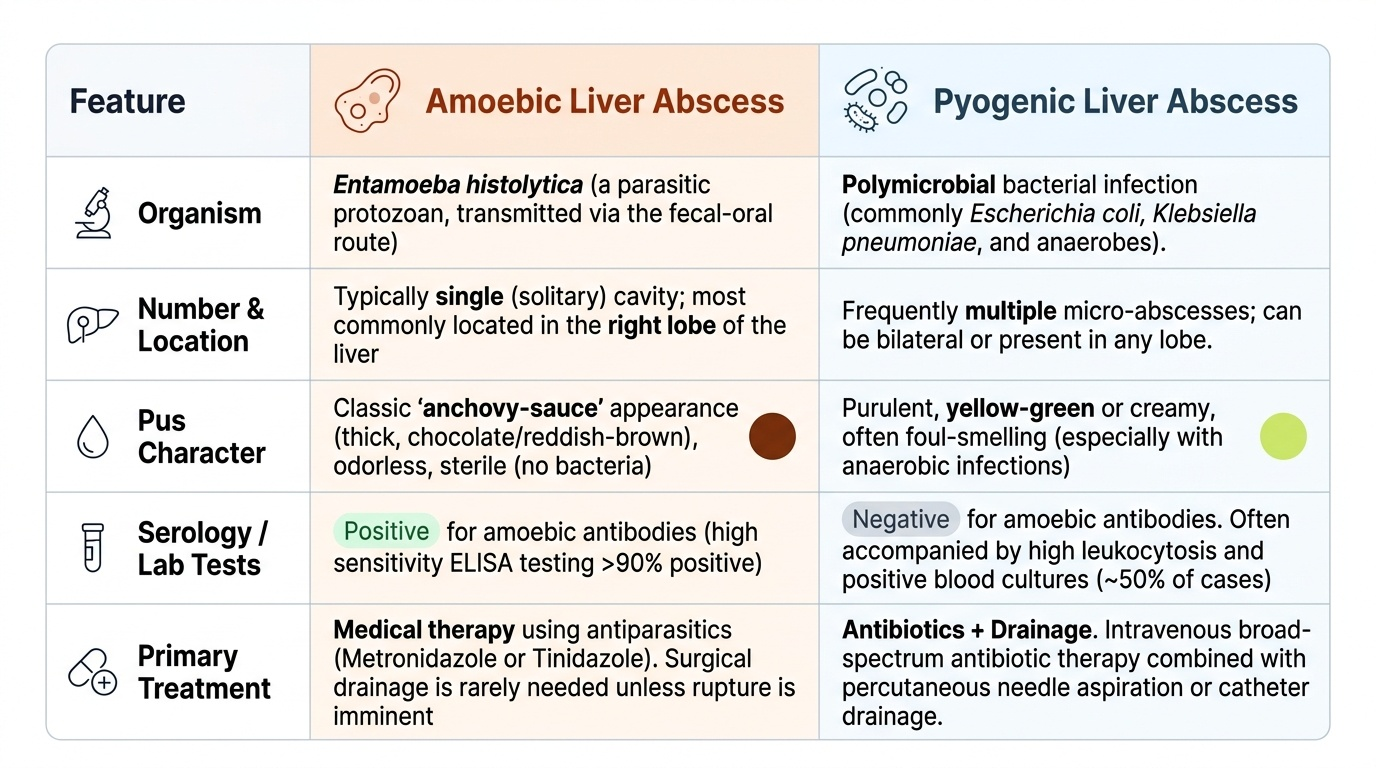
The pathology of each problem can now be understood against this background. Amoebic abscess results from Entamoeba histolytica trophozoites reaching the liver through the portal vein from colonic infection; they cause liquefactive necrosis producing the classic "anchovy-sauce" (reddish-brown) sterile pus, usually a single cavity in the right lobe. Pyogenic abscess is bacterial (often polymicrobial, including E. coli and anaerobes) and arises from biliary disease, portal pyaemia (e.g. appendicitis), or haematogenous spread; abscesses are frequently multiple. Hydatid disease is caused by the larval stage of the tapeworm Echinococcus granulosus; humans are accidental intermediate hosts who ingest eggs shed by dogs, and the larva forms a slowly expanding cyst with a laminated wall and daughter cysts containing infective scolices. Liver tumours include benign lesions (haemangioma — the commonest, a vascular malformation; focal nodular hyperplasia; and hepatic adenoma, linked to oral contraceptives) and malignant lesions — primary hepatocellular carcinoma arising on a background of cirrhosis, hepatitis B or C, and secondary metastases, which are in fact the commonest malignant liver tumours overall.
SELF-CHECK
A liver abscess that is single, located in the right lobe, and yields sterile reddish-brown "anchovy-sauce" pus is most likely caused by which organism?
A. Escherichia coli
B. Entamoeba histolytica
C. Echinococcus granulosus
D. Staphylococcus aureus
Reveal Answer
Answer: B. Entamoeba histolytica
These features are classic for an amoebic liver abscess caused by the protozoan Entamoeba histolytica, which reaches the liver via the portal vein and causes liquefactive necrosis; the pus is sterile on ordinary culture. E. coli causes pyogenic (bacterial) abscess, Echinococcus granulosus causes hydatid cysts (not abscess), and S. aureus is a less common pyogenic cause.
Examination and Investigation of the Liver Lesion
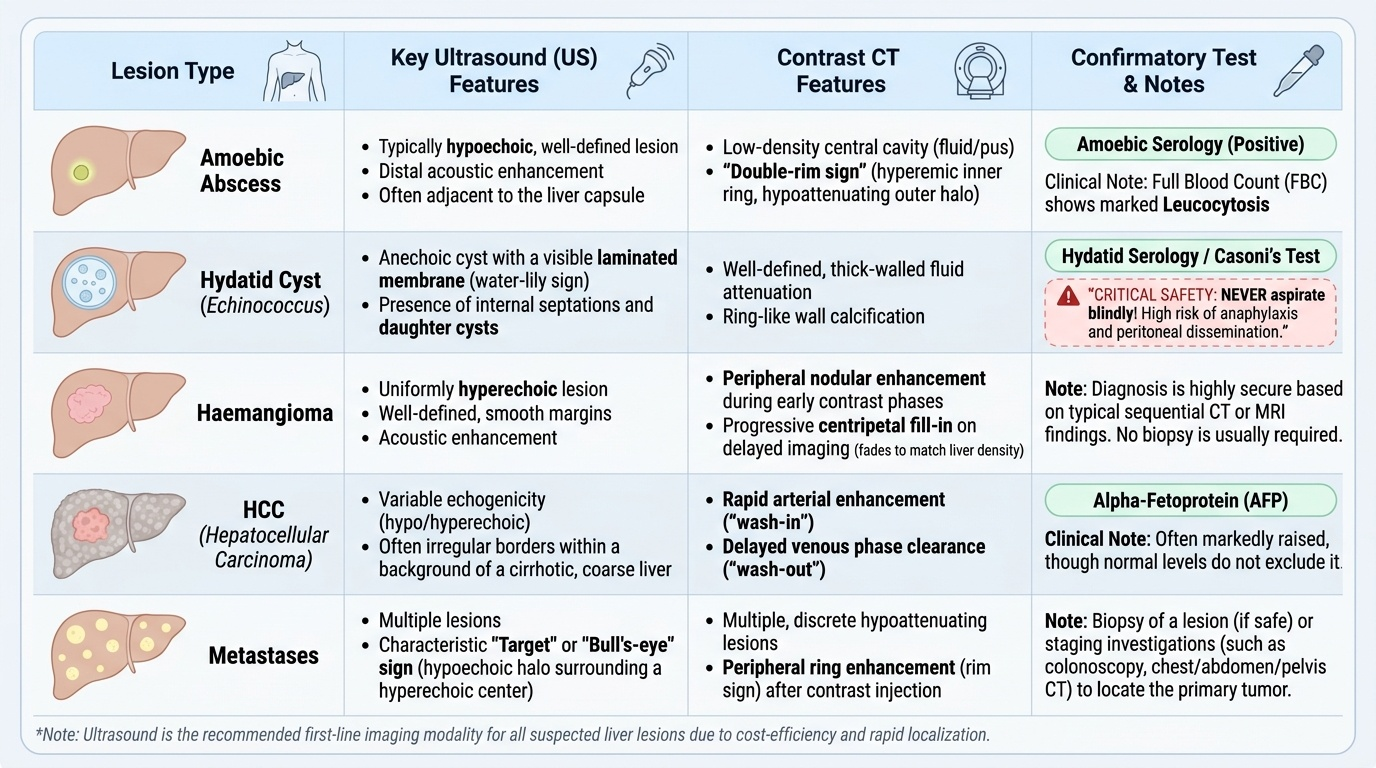
Examination begins with the general state — fever, weight loss, jaundice, pallor, signs of chronic liver disease — and proceeds to the abdomen, where you palpate for tender or non-tender hepatomegaly, assess its surface (smooth in abscess and hydatid, hard and irregular in malignancy), and check for ascites, a palpable gallbladder and splenomegaly. In trauma you are looking instead for the signs of intra-abdominal haemorrhage: tachycardia, hypotension, abdominal distension and tenderness. Investigation is then directed by the suspected diagnosis. Ultrasound is the first-line imaging in almost every case — cheap, quick and excellent for distinguishing solid from cystic, locating an abscess for drainage, and showing the daughter cysts and laminated membrane of hydatid disease. Contrast-enhanced CT characterises lesions further, defines segmental anatomy for surgery, stages tumours, and in trauma grades the injury and detects active bleeding. Blood tests include a full blood count (leucocytosis in abscess), liver function tests, and serology: amoebic serology is positive in most invasive amoebic disease, and Casoni's test and hydatid (echinococcal) serology support hydatid disease. The tumour marker alpha-fetoprotein (AFP) is often markedly raised in hepatocellular carcinoma, though a normal level does not exclude it.
Provided image
A crucial safety rule belongs here. A cystic liver lesion that might be hydatid must never be aspirated blindly for diagnosis, because spillage of cyst fluid can trigger fatal anaphylaxis and disseminate daughter cysts throughout the peritoneum. Diagnosis of hydatid rests on imaging plus serology, not on a diagnostic tap. By contrast, an amoebic or pyogenic abscess can be safely aspirated under ultrasound guidance when needed — confirming the diagnosis (anchovy-sauce pus, or pus that grows organisms) and relieving the cavity.