Page 14 of 20
SU28.17 | Common Anorectal Diseases — SDL Guide (Part 2)
Principles of Management
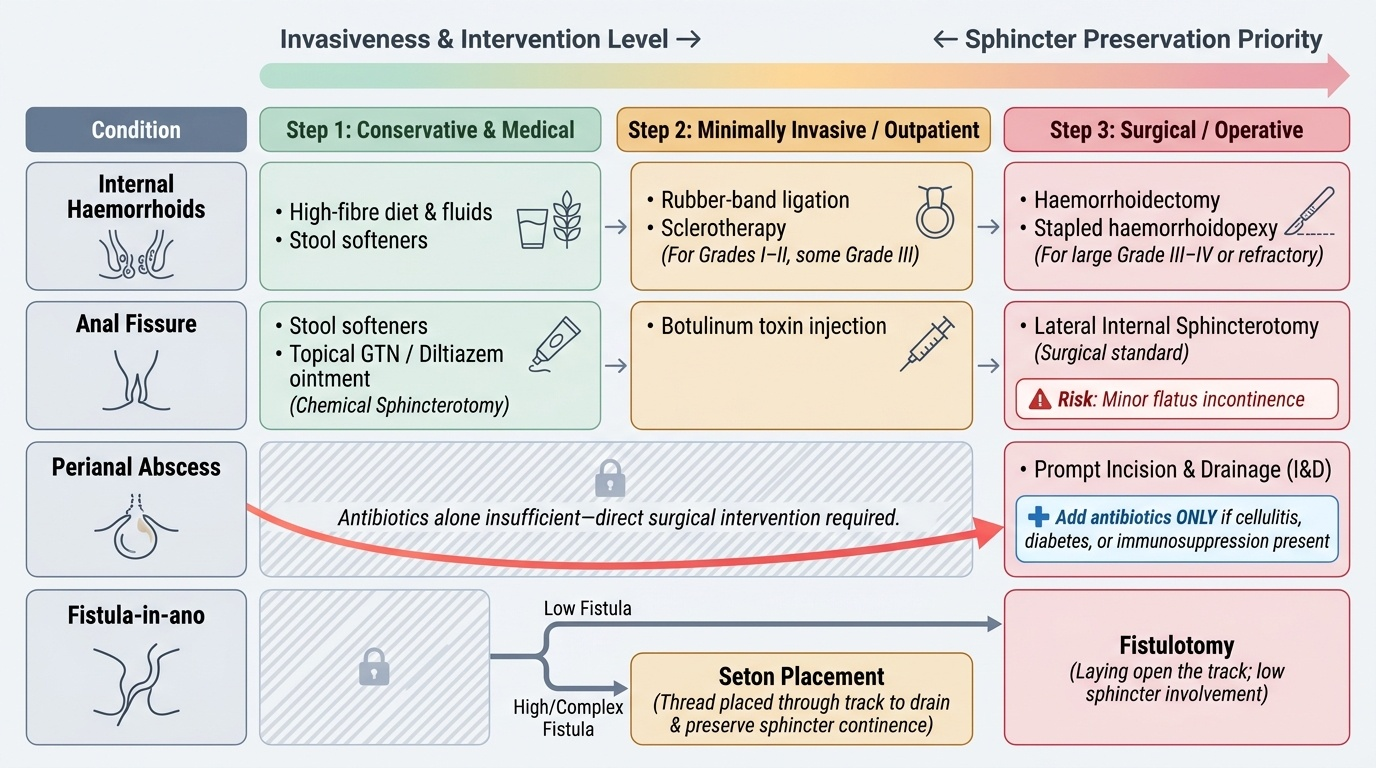
Management of each condition follows a logical ladder from conservative to operative, always respecting the sphincter complex. Haemorrhoids are managed by severity: a high-fibre diet, adequate fluids and stool softeners for all, with rubber-band ligation or sclerotherapy for grade I–II (and many grade III) internal haemorrhoids in the outpatient setting, and haemorrhoidectomy (or stapled/haemorrhoidopexy techniques) reserved for large grade III–IV or refractory disease; an acutely thrombosed external haemorrhoid seen early can be excised for rapid relief, otherwise it settles with analgesia. An anal fissure is managed first by stool softening and topical agents that relax the internal sphincter — glyceryl trinitrate (GTN) or diltiazem ointment ('chemical sphincterotomy') — then botulinum toxin, and finally, for a chronic fissure refractory to medical therapy, lateral internal sphincterotomy (the surgical standard, whose recognised risk is minor incontinence to flatus). A perianal/anorectal abscess must be treated by prompt incision and drainage — antibiotics alone are not sufficient for an abscess — with antibiotics added if there is surrounding cellulitis, diabetes or immunosuppression. A fistula-in-ano is treated by fistulotomy (laying open a low fistula) for tracks that involve little sphincter, and by a seton (a thread placed through the track to drain it and preserve continence, sometimes used to gradually cut through) for high or complex fistulae where simple laying-open would risk incontinence. Rectal prolapse is repaired by an abdominal procedure (rectopexy, increasingly laparoscopic, with the best durability) or a perineal procedure (Delorme's or Altemeier's, suited to frail patients). Anal squamous cell carcinoma is treated primarily by chemoradiotherapy (the Nigro regimen: 5-fluorouracil + mitomycin C + radiotherapy), which preserves the sphincter and cures most patients, reserving abdominoperineal resection (APR) for residual or recurrent disease — a deliberately different strategy from the surgery-first approach to rectal adenocarcinoma. Throughout, the principle is to treat the symptom proportionately and never to sacrifice continence unnecessarily.
Provided image
| Condition | Management ladder |
|---|---|
| Internal haemorrhoids | Diet/fibre/stool softeners → banding or sclerotherapy (I–III) → haemorrhoidectomy (III–IV/refractory) |
| Anal fissure | Stool softeners → topical GTN/diltiazem → botulinum toxin → lateral internal sphincterotomy |
| Perianal / anorectal abscess | Prompt incision and drainage (antibiotics alone insufficient) |
| Fistula-in-ano | Fistulotomy (low) or seton (high/complex, to preserve continence) |
| Rectal prolapse | Abdominal rectopexy or perineal (Delorme/Altemeier) repair |
| Anal squamous cell carcinoma | Chemoradiotherapy (Nigro regimen); APR for salvage |
CLINICAL PEARL
Two rules will keep you safe in anorectal practice. First, never call rectal bleeding 'just piles' without excluding a proximal colorectal cancer — examine the patient and arrange a colonoscopy where there are red flags or the patient is older. Second, an anal abscess needs drainage, not antibiotics — pus must be let out, and waiting on antibiotics lets it spread and risks a complex fistula. And whenever you operate near the sphincter — a fissure or a high fistula — remember the continence mechanism: a seton preserves the sphincter where laying open would not.
Check Your Understanding
Bring it together by reasoning through the four patients from the hook. The first, with painless bright-red bleeding, has internal haemorrhoids (above the dentate line) — managed by fibre and stool softeners, with banding for persistent grade I–II disease, after a colonoscopy has excluded a proximal cancer. The second, with searing pain on defaecation and a posterior skin tag, has a chronic anal fissure — managed by stool softeners and topical GTN or diltiazem, then botulinum toxin, then lateral internal sphincterotomy if it fails. The third, with a hot, tender perianal swelling and fever, has a perianal abscess — needing prompt incision and drainage, not antibiotics alone. The fourth, with a chronic perianal discharge, has a fistula-in-ano — mapped by Goodsall's rule and MRI and treated by fistulotomy or a seton to protect continence. Now self-test the three competency strands. First, can you give the dominant symptom and clinical features of each condition (haemorrhoids, fissure, fistula, abscess, prolapse, anal cancer)? Second, can you describe the examination (inspection, DRE, proctoscopy, Goodsall's rule) and state the cardinal rule of excluding a proximal cancer? Third, can you outline the management ladder for each, including the Nigro regimen for anal cancer and the continence-sparing logic of a seton? The questions below check exactly these links.
SELF-CHECK
What is the primary treatment of anal squamous cell carcinoma, and how does it differ from the management of rectal adenocarcinoma?
A. Abdominoperineal resection first; the same as for rectal adenocarcinoma
B. Chemoradiotherapy (Nigro regimen) first, with surgery for salvage; rectal adenocarcinoma is treated primarily surgically
C. Topical chemotherapy only; rectal cancer needs radiotherapy only
D. Local excision only; rectal cancer needs chemoradiotherapy only
Reveal Answer
Answer: B. Chemoradiotherapy (Nigro regimen) first, with surgery for salvage; rectal adenocarcinoma is treated primarily surgically
Anal squamous cell carcinoma is treated PRIMARILY by chemoradiotherapy — the Nigro regimen (5-fluorouracil + mitomycin C + radiotherapy) — which is sphincter-preserving and curative in most patients, reserving abdominoperineal resection for residual/recurrent disease. Rectal adenocarcinoma, a different tumour, is treated primarily by surgical resection (often with neoadjuvant chemoradiotherapy for advanced rectal tumours).