Page 1 of 20
SU28.13 | Small Intestine and Large Intestine Anatomy — SDL Guide
Learning Objectives
- Describe the gross structure of the small and large intestine and the wall and mucosal features that distinguish them (SU28.13).
- Describe the arterial supply, venous and lymphatic drainage of the intestines, including the superior and inferior mesenteric territories and the watershed zones (SU28.13).
- Apply intestinal anatomy to surgical resection, anastomosis and the interpretation of a plain abdominal radiograph (SU28.13).
INSTRUCTIONS
Almost every operation on the gut — resecting a tumour, relieving an obstruction, fashioning an anastomosis, or reading the bowel-gas pattern on an X-ray — is anatomy made practical. The single most important idea in this module is that the small and large intestine are supplied along an embryological midgut–hindgut divide by two different arteries, and that this divide explains where the bowel becomes ischaemic, where a surgeon must take the vascular pedicle for a cancer operation, and why small and large bowel look different on the film. This is the basic-science foundation on which the disorders of the intestine, appendix and anorectum all build.
References
- Bailey & Love's Short Practice of Surgery, The Small and Large Intestine (textbook)
- SRB's Manual of Surgery, Intestine and Colon (textbook)
- Sabiston Textbook of Surgery, Small Intestine and Colon and Rectum (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A surgeon is operating on a 64-year-old man for a cancer near the splenic flexure of the colon. As she mobilises the bowel she pauses at one particular zone where, she explains to the students scrubbed alongside her, the blood supply is at its most marginal — the very place where, in another patient last month, a stretch of colon had turned dusky and ischaemic after a drop in blood pressure. A few metres further along the gut, the same operation on the same patient would draw blood from an entirely different artery. None of this is arbitrary. The intestine is supplied along a hidden embryological seam, and knowing exactly where that seam runs is what lets a surgeon take the right vascular pedicle, anticipate where the bowel will die, and even tell small bowel from large on a plain X-ray. Everything in this module flows from that map.
WHY THIS MATTERS
Intestinal anatomy is not anatomy for its own sake — it is the reasoning behind the commonest abdominal operations and investigations you will meet. The split between the superior and inferior mesenteric arteries decides how much bowel a surgeon must remove with a colonic cancer (the resection follows the artery and its draining lymph nodes), and it predicts the watershed zones where the colon turns ischaemic when perfusion fails. The wall features — valvulae conniventes in the small bowel, haustra in the large — let you read a plain abdominal radiograph and say at a glance whether an obstruction is small-bowel or large-bowel, which changes the whole differential and the urgency. For a final-year student, this anatomy is examined directly and is the scaffold for the disorders, appendicitis and anorectal disease that follow. Master the map now and the clinical SDLs become far easier.
RECALL
Recall a few foundations from your first-year anatomy and embryology before we build on them. The primitive gut tube is divided into foregut, midgut and hindgut, and each keeps its own artery for life: the foregut is supplied by the coeliac trunk, the midgut by the superior mesenteric artery (SMA), and the hindgut by the inferior mesenteric artery (IMA). The midgut runs from the second part of the duodenum to the proximal two-thirds of the transverse colon; the hindgut from the distal transverse colon to the upper rectum. Recall too that the veins draining the intestine join the portal venous system to reach the liver, and that intestinal lymph drains through tiers of mesenteric lymph nodes that lie along the arteries. Keep this midgut–hindgut, SMA–IMA divide firmly in mind — the rest of this module is essentially that one idea applied.
Why Intestinal Anatomy Decides the Operation
Surgical anatomy of the intestine answers three recurring clinical questions, and it is worth naming them before the detail. First, how much do I remove and where do I divide the vessels? When a surgeon resects a segment of bowel for cancer, the operation is planned around the artery that supplies it, because the draining lymph nodes — which must be cleared for an oncological cure — run alongside that artery; taking the correct vascular pedicle therefore defines the resection. Second, where will the bowel become ischaemic? The colon is most vulnerable at the boundaries between arterial territories, the so-called watershed zones, and these are predictable from the anatomy. Third, what am I looking at on the X-ray and at operation? The small and large intestine have distinct wall and mucosal features that let you identify them on a plain film and tell which part of the gut you are handling. All three questions reduce to a single underlying fact: the gut is supplied along an embryological seam by two arteries, the SMA for the midgut and the IMA for the hindgut, and the small and large bowel are structurally different organs. The rest of this module develops that fact and shows how each clinical decision falls out of it.
Provided image
Normal Structure: Small Intestine and Large Intestine
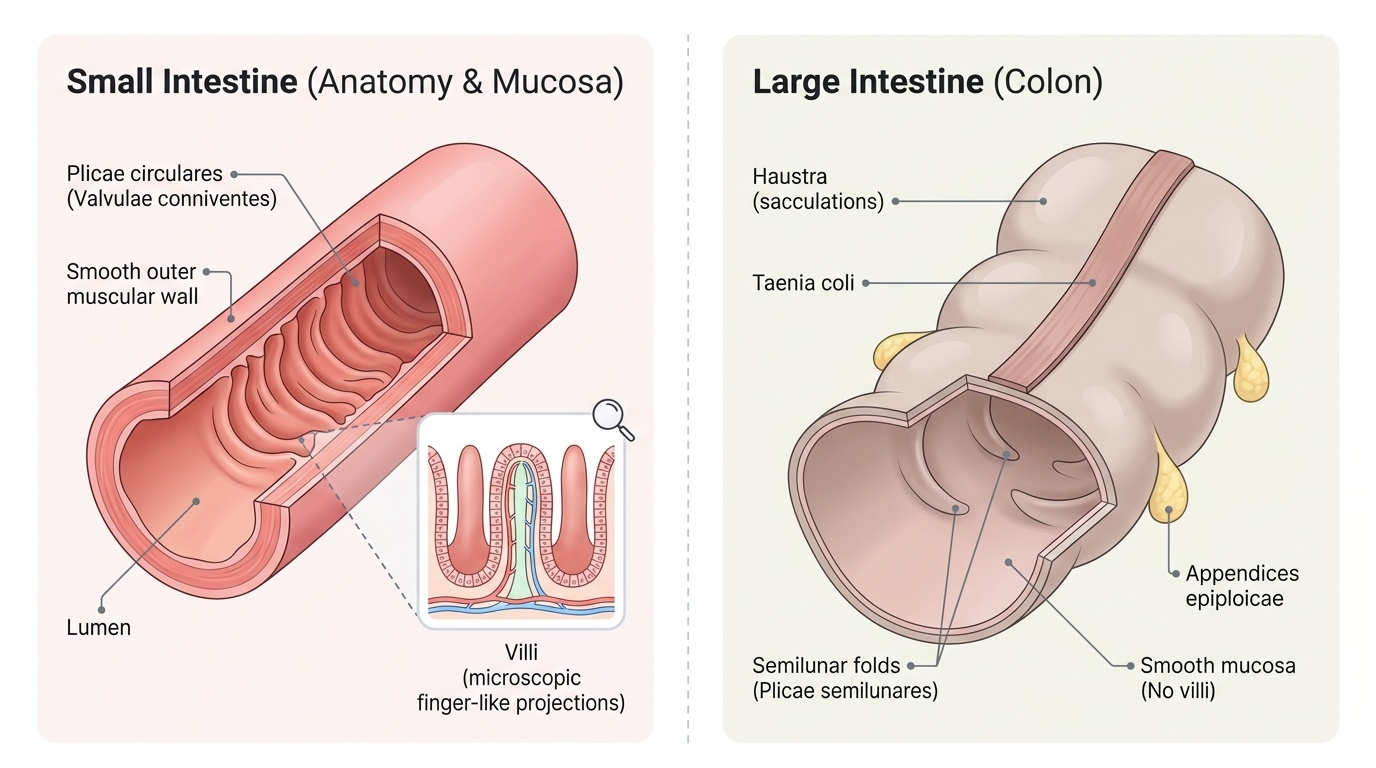
The small intestine comprises the duodenum, jejunum and ileum and measures roughly six metres in the living adult, the great majority being the mobile, mesentery-suspended jejunum and ileum; the duodenum is a short, C-shaped, largely retroperitoneal segment of about 25–30 cm. The jejunum makes up roughly the proximal two-fifths of the mobile small bowel and the ileum the distal three-fifths, and they differ usefully at operation: the jejunum is wider, thicker-walled, more vascular and has long straight vessels (vasa recta) with few arcades, whereas the ileum is narrower, thinner, has shorter vasa recta with multiple arcades, and carries the lymphoid Peyer's patches. The defining internal feature of the small bowel is the plicae circulares (valvulae conniventes) — permanent circular mucosal folds that, with the villi, vastly increase the absorptive surface; these folds span the whole circumference of the lumen, a fact that matters on the abdominal X-ray. The large intestine runs from the caecum (with the appendix) through the ascending, transverse, descending and sigmoid colon to the rectum and anal canal, and is about 1.5 metres long. Its hallmark features are three longitudinal muscle bands, the taenia coli, which are shorter than the gut and gather it into sacculations called haustra; fatty tags, the appendices epiploicae, hang from its surface. The large bowel has no villi and no plicae circulares. These structural differences — valvulae conniventes and villi versus taenia, haustra and appendices epiploicae — are how you distinguish small from large bowel by eye, on film, and at operation.
- Small intestine: jejunum + ileum (~6 m living), mesentery-suspended, SMA-supplied; plicae circulares (valvulae conniventes) + villi; jejunum wide/vascular/few arcades, ileum narrow/many arcades/Peyer's patches.
- Large intestine: caecum→sigmoid + rectum/anal canal (~1.5 m); taenia coli, haustra, appendices epiploicae; no villi.
- Appendix arises from the posteromedial caecum where the three taenia converge.
SELF-CHECK
On a plain abdominal radiograph, which feature identifies a dilated loop as SMALL bowel rather than large bowel?
A. Haustra that do not cross the lumen
B. Valvulae conniventes (plicae circulares) that span the entire lumen
C. A peripheral position in the abdomen
D. Appendices epiploicae
Reveal Answer
Answer: B. Valvulae conniventes (plicae circulares) that span the entire lumen
Valvulae conniventes (plicae circulares) are circular folds that cross the whole circumference of the small-bowel lumen, so on an X-ray they appear as complete lines spanning the dilated loop, which sits centrally. Haustra are sacculations of the LARGE bowel, separated by folds that do NOT cross the full lumen, and large bowel sits peripherally.
Blood Supply, Lymphatic Drainage and the Watershed Zones
The blood supply follows the embryological seam exactly. The superior mesenteric artery (SMA) supplies the midgut — the whole of the jejunum and ileum, the caecum and appendix, the ascending colon, and the proximal two-thirds of the transverse colon — through its jejunal and ileal branches and the ileocolic, right colic and middle colic arteries. The inferior mesenteric artery (IMA) supplies the hindgut — the distal one-third of the transverse colon, the descending and sigmoid colon, and the upper rectum — through its left colic, sigmoid and superior rectal branches. Crucially, these two territories are linked along the inner border of the colon by the marginal artery of Drummond, a continuous anastomotic channel that allows some collateral flow across the SMA–IMA divide. The price of relying on this collateral is that flow is thinnest where the two systems meet, and these are the watershed zones: the splenic flexure (Griffiths' point, at the SMA–IMA junction of the transverse/descending colon) and the rectosigmoid junction (Sudeck's point), which are the classic sites of ischaemic colitis when perfusion falls. Venous drainage mirrors the arteries: the superior and inferior mesenteric veins carry intestinal blood into the portal system and so to the liver (which is why colorectal cancer metastasises first to the liver). Lymphatic drainage passes through tiers of mesenteric lymph nodes arranged along the arteries — the very nodes a cancer operation must clear.
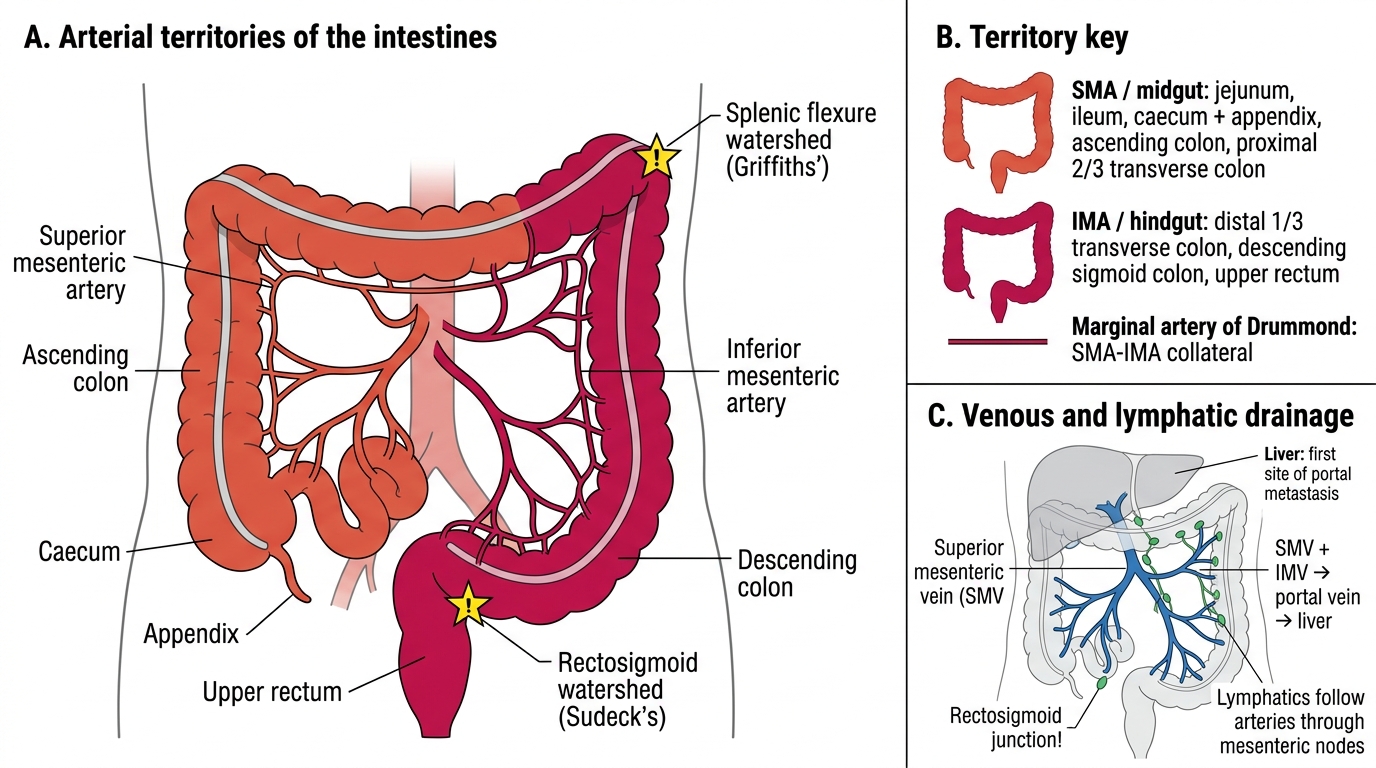
Arterial Supply of the Intestines
- SMA (midgut): jejunum, ileum, caecum/appendix, ascending colon, proximal two-thirds of transverse colon.
- IMA (hindgut): distal one-third of transverse colon, descending and sigmoid colon, upper rectum.
- Marginal artery of Drummond links SMA and IMA; watershed zones = splenic flexure (Griffiths') and rectosigmoid (Sudeck's) — sites of ischaemic colitis.
- Venous: SMV + IMV → portal vein → liver (first site of metastasis). Lymphatics follow the arteries through mesenteric nodes.