Page 17 of 26
SU29.{6,8} | Renal Tumours and Bladder Cancer — SDL Guide (Part 2)
Surgical and Oncological Management
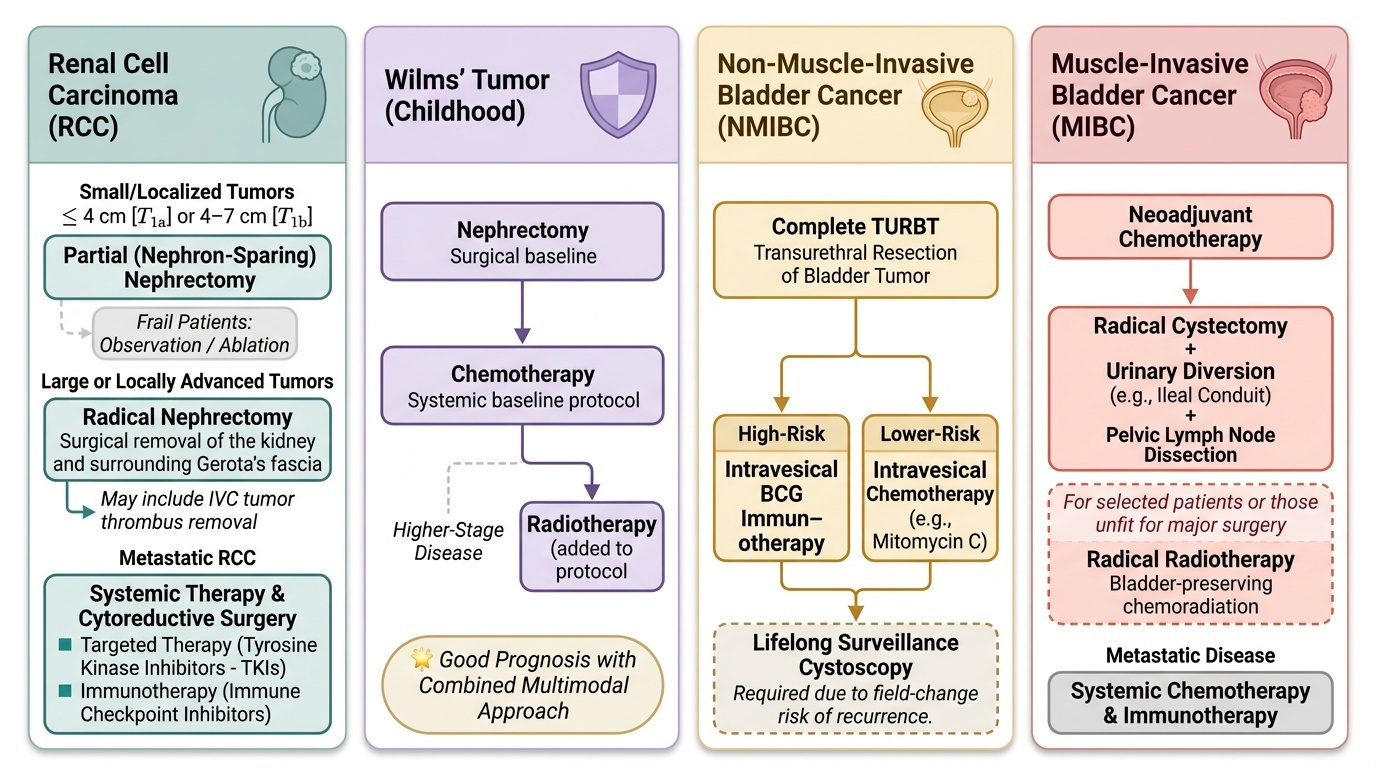
Management of both tumours follows logically from the staging just described, and the principles are best learned tumour by tumour. For renal cell carcinoma, surgery is the mainstay of cure because the tumour is radio- and chemo-resistant. A radical nephrectomy — removal of the kidney with its surrounding (Gerota's) fascia — is the standard operation for a large or locally advanced but resectable tumour, and removing IVC tumour thrombus may be part of the procedure. For a small tumour — T1a (4 cm or less), and in selected T1b tumours (4–7 cm) where technically feasible — a partial (nephron-sparing) nephrectomy is preferred, because preserving functioning kidney protects long-term renal function; small tumours in frail patients may even be observed or ablated. For metastatic RCC, conventional chemotherapy and radiotherapy are largely ineffective, so systemic treatment relies on targeted therapy with tyrosine kinase inhibitors and on immunotherapy (immune checkpoint inhibitors), sometimes combined with cytoreductive surgery in selected patients. The childhood tumour, Wilms' tumour, is treated by a multimodal protocol of nephrectomy combined with chemotherapy, with radiotherapy added for higher-stage disease, and carries a good prognosis with this combined approach. For bladder cancer, management is dictated entirely by the muscle-invasion status. Non-muscle-invasive bladder cancer (NMIBC) is treated by complete TURBT followed by intravesical therapy — intravesical BCG immunotherapy for high-risk disease, or intravesical chemotherapy (for example mitomycin C) for lower-risk disease — to reduce recurrence and progression, with lifelong surveillance cystoscopy because urothelial cancer recurs as a field-change disease. Muscle-invasive bladder cancer (MIBC) requires aggressive treatment: the standard is radical cystectomy with urinary diversion (for example an ileal conduit) and pelvic lymph node dissection, often preceded by neoadjuvant chemotherapy; radical radiotherapy (bladder-preserving chemoradiation) is an alternative for selected patients or those unfit for major surgery. Metastatic bladder cancer is treated with systemic chemotherapy and, increasingly, immunotherapy. The unifying principle across all of these is that accurate staging — the renal mass on CT, the bladder tumour on TURBT — is what makes the right operation possible.
Provided image
| Tumour | First-line management | Key principle |
|---|---|---|
| RCC, small/T1 | Partial (nephron-sparing) nephrectomy | Preserve renal function |
| RCC, large/locally advanced | Radical nephrectomy (+/- IVC thrombus removal) | Surgery is curative; RCC is radio-/chemo-resistant |
| RCC, metastatic | Targeted therapy (TKIs) / immunotherapy +/- cytoreductive surgery | Conventional chemo/radiotherapy ineffective |
| Wilms' tumour | Nephrectomy + chemotherapy (+/- radiotherapy) | Multimodal; good prognosis |
| Bladder, NMIBC | TURBT + intravesical BCG / chemotherapy + surveillance | Preserve bladder; recurrence-prone field disease |
| Bladder, MIBC | Radical cystectomy + urinary diversion (+/- neoadjuvant chemo) or radical radiotherapy | Muscle invasion mandates radical treatment |
CLINICAL PEARL
Painless visible haematuria is bladder cancer until proven otherwise — and the fact that the bleeding has stopped is NOT reassuring. Urothelial tumours bleed intermittently, so a single episode of painless visible haematuria that clears spontaneously still mandates referral for flexible cystoscopy and upper-tract imaging. Equally, never let a normal urine dipstick or a treated urinary infection close the case: the cancer can hide behind a coincidental infection. The patient who is told 'the blood has gone, all is well' is the patient whose curable tumour is found too late.
Check Your Understanding
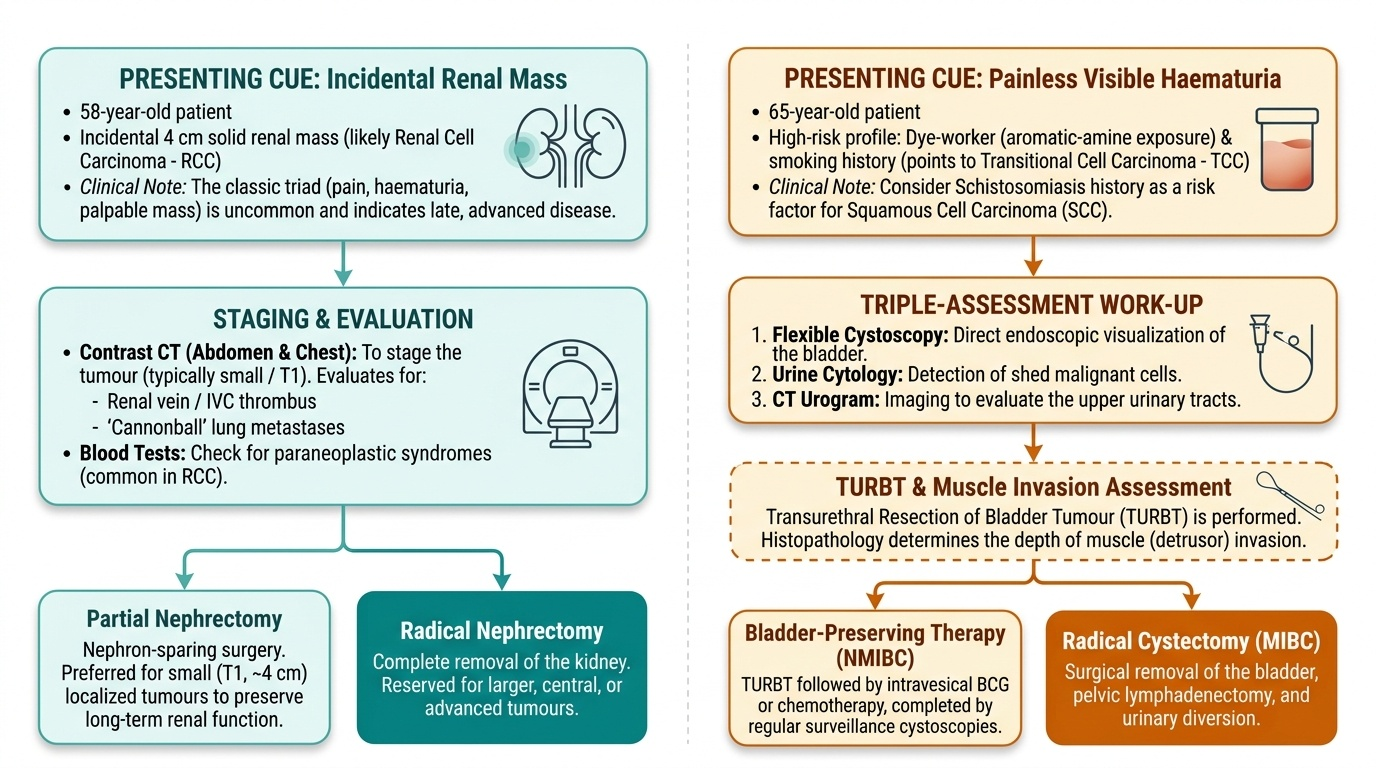
Bring the threads together by reasoning back through the two patients in the hook, because they map exactly onto the two competencies of this module. The 58-year-old with the incidental 4 cm solid renal mass sits squarely in the renal-tumour story: this is most likely a renal cell carcinoma, and because it is small (around T1) the goal is a partial, nephron-sparing nephrectomy after a contrast CT of the abdomen and chest has staged it — looking specifically for renal vein/IVC thrombus and cannonball lung metastases — and after bloods have been checked for paraneoplastic features. Remember that had he instead presented with the full triad and a palpable mass, that would have implied late, advanced disease, not an early one. The 65-year-old dye-worker with painless intermittent visible haematuria sits in the bladder-cancer story: his occupational aromatic-amine exposure and (especially) smoking point to a transitional cell carcinoma, he needs flexible cystoscopy, urine cytology and a CT urogram, and the TURBT that follows will tell us, by the depth of muscle invasion, whether he has bladder-preserving NMIBC (TURBT plus intravesical BCG or chemotherapy and surveillance) or MIBC demanding radical cystectomy. Use these cases to self-test the two competencies. First, for renal tumours: can you state why the classic triad signals late disease, name the commonest RCC subtype and its cell of origin, recall the paraneoplastic syndromes, and choose between radical and partial nephrectomy — and can you name the commonest renal tumour of childhood and its treatment? Second, for bladder cancer: can you name the commonest type and its major risk factors, recall the schistosomiasis–SCC link, recite the work-up (cystoscopy, cytology, CT urogram, TURBT), and explain how muscle invasion divides management into intravesical therapy versus radical cystectomy? The questions and the summary that follow check exactly these links.
Provided image
SELF-CHECK
Which statement about renal cell carcinoma is correct?
A. The classic triad of haematuria, flank pain and a palpable mass is common and usually indicates early, curable disease
B. It is highly radiosensitive, so radiotherapy is the first-line treatment for the primary tumour
C. The clear-cell subtype is the most common, it arises from proximal tubular epithelium, and it may extend as tumour thrombus into the IVC
D. It is the commonest renal tumour of childhood and is treated with nephrectomy plus chemotherapy
Reveal Answer
Answer: C. The clear-cell subtype is the most common, it arises from proximal tubular epithelium, and it may extend as tumour thrombus into the IVC
Clear-cell RCC is the commonest subtype, arises from the proximal convoluted tubule, and characteristically invades the renal vein and may extend as tumour thrombus into the IVC, spreading to lung ('cannonball' metastases) and bone. The classic triad is in fact UNCOMMON and indicates LATE disease (most RCCs are now incidental findings). RCC is relatively radio- and chemo-RESISTANT, so surgery (radical or partial nephrectomy) is the mainstay and targeted therapy/immunotherapy is used for metastatic disease. The commonest renal tumour of CHILDHOOD is Wilms' tumour, not RCC.