Page 8 of 17
SU30.3-5 | Epididymo-Orchitis, Varicocele and Hydrocele — SDL Guide (Part 2)
Principles of Management
Treatment follows the diagnosis, with the safety net that any unresolved suspicion of torsion goes to theatre. Epididymo-orchitis is treated with empirical antibiotics chosen by the likely organism — covering Chlamydia/gonococcus in sexually active young men (with partner treatment and STI counselling) and urinary coliforms in older men or those with urinary tract disease — together with analgesia, scrotal support, rest and, where relevant, treatment of any underlying obstruction; if torsion cannot be confidently excluded, the patient undergoes urgent surgical exploration rather than a trial of antibiotics. Varicocele is often managed conservatively with reassurance and a scrotal support when it is asymptomatic and fertility is not in question; intervention — surgical varicocelectomy (ligation of the dilated veins) or radiological embolisation — is reserved for significant pain, a varicocele causing testicular atrophy in an adolescent, or selected subfertile men with abnormal semen parameters; and any suspicious right-sided or non-decompressing varicocele is investigated for an underlying renal/retroperitoneal cause. Hydrocele in an adult that is small and asymptomatic may simply be observed; a large, tense or symptomatic primary hydrocele is treated surgically (e.g. Jaboulay's procedure — eversion of the sac — or Lord's plication), which is preferred to repeated aspiration; a secondary hydrocele is managed by treating its cause (infection, and crucially any underlying tumour) — one must never simply aspirate a hydrocele and reassure when a testicular tumour beneath it has not been excluded. In children, a congenital (communicating) hydrocele often resolves spontaneously by about two years and is otherwise treated by herniotomy (ligation of the patent processus vaginalis), not by aspiration.
Provided image
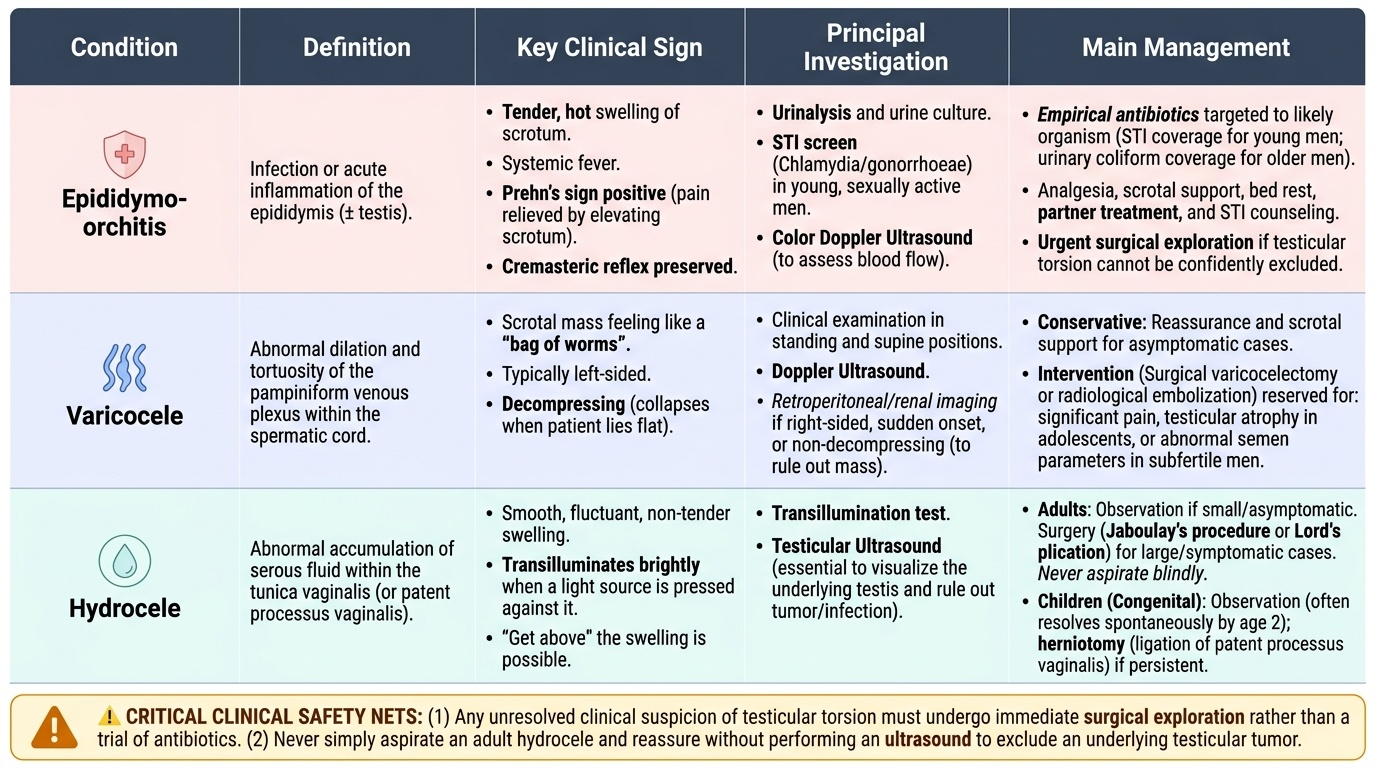
| Condition | Definition | Key clinical sign | Principal investigation | Main management |
|---|---|---|---|---|
| Epididymo-orchitis | Infection/inflammation of epididymis ± testis | Tender swelling, fever, Prehn's sign positive, reflex preserved | Urinalysis/culture + STI screen; Doppler US | Organism-directed antibiotics, analgesia, scrotal support, partner treatment; explore if torsion not excluded |
| Varicocele | Dilated pampiniform plexus (usually left) | 'Bag of worms', worse standing, decompresses lying | Standing exam/Valsalva; semen analysis; image new/right-sided | Reassurance/support; varicocelectomy or embolisation for pain/atrophy/subfertility |
| Hydrocele | Serous fluid within the tunica vaginalis | Transilluminant, can get above it | Transillumination; ultrasound to assess testis | Observe (small); Jaboulay/Lord's surgery; treat the cause of a secondary hydrocele (exclude tumour) |
CLINICAL PEARL
In every acutely painful scrotum, exclude testicular torsion FIRST — do not let a fever or dysuria lull you into calling it epididymo-orchitis, because torsion is a time-critical emergency (best salvage within about 6 hours) and a Doppler ultrasound must never delay surgical exploration when the diagnosis is clinically suspected. Two more habits save errors: never aspirate a hydrocele and reassure without excluding an underlying testicular tumour (treat the cause of a secondary hydrocele), and treat a new or non-decompressing right-sided varicocele as a red flag for a renal or retroperitoneal mass until imaging proves otherwise.
Check Your Understanding
Bring the three patients from the hook back and run the reasoning. The 28-year-old with a two-day tender, hot, swelling hemiscrotum, fever, dysuria and relief on elevation has epididymo-orchitis: Prehn's sign is positive and the cremasteric reflex is preserved, so you would screen the urine and (given his age) for STIs, start organism-directed antibiotics with analgesia and scrotal support, and treat his partner — reasoning from 'gradual, febrile, eases on lifting' to 'infection, treat appropriately'. The 19-year-old with sudden, severe pain, a high-riding tender testis and an absent reflex has testicular torsion until proven otherwise: you would proceed to urgent surgical exploration without letting imaging delay theatre — reasoning from 'sudden, no relief, absent reflex, teenager' to 'emergency'. The 32-year-old with a soft, painless, transilluminant swelling you can get above has a hydrocele, which you would scan to exclude an underlying tumour before deciding between observation and surgery. Now self-test the competency directly. Can you give the applied anatomy behind the left-sided varicocele and the tunica-vaginalis origin of a hydrocele? Can you list the clinical features and the bedside signs (get-above-it, transillumination, Prehn's sign, cremasteric reflex, standing/Valsalva) that separate the three swellings — and torsion — from one another? Can you name the targeted investigations and the principles of management for each, including the rules to exclude torsion, exclude a tumour beneath a hydrocele, and image a suspicious varicocele? The questions that follow check these links.
SELF-CHECK
A 35-year-old is found to have a soft scrotal swelling that transilluminates brightly and above which the examining fingers can meet. What is the diagnosis, and what is the essential next step before reassurance?
A. Inguinoscrotal hernia — arrange urgent herniorrhaphy
B. Hydrocele — aspirate it in clinic and reassure
C. Hydrocele — perform ultrasound of the testis to exclude an underlying tumour (secondary hydrocele)
D. Varicocele — recommend a scrotal support only
Reveal Answer
Answer: C. Hydrocele — perform ultrasound of the testis to exclude an underlying tumour (secondary hydrocele)
A transilluminant scrotal swelling above which you can get is a hydrocele (you cannot get above an inguinoscrotal hernia). Before reassuring, the underlying testis must be assessed with ultrasound, because a hydrocele may be secondary to a testicular tumour. Simply aspirating and reassuring risks missing a cancer; aspiration is not the definitive treatment for a primary hydrocele either.