Page 2 of 17
SU30.1 | Phimosis, Paraphimosis and Carcinoma Penis — SDL Guide (Part 2)
Surgical and Emergency Management
Management follows directly from the diagnosis and its urgency. Physiological phimosis in a young boy needs only reassurance and hygiene advice — most resolve spontaneously and forcible retraction is harmful; a short course of topical steroid can soften a mildly tight ring in selected children, with circumcision reserved for true pathological or symptomatic cases. Pathological phimosis (a scarred ring, recurrent balanitis, BXO, or obstructive symptoms) is treated by circumcision, the definitive removal of the prepuce, which is also therapeutic for recurrent infection. Paraphimosis is the emergency: attempt prompt manual reduction — squeeze the oedematous glans steadily for several minutes to reduce its bulk (a compressive technique, with adequate analgesia or a penile block), then push the glans back through the constricting ring while drawing the foreskin forward. If manual reduction fails, a dorsal slit of the constricting band relieves it urgently; once the acute episode settles, an elective circumcision prevents recurrence. Carcinoma penis is managed by stage- and grade-directed surgery plus management of the inguinal nodes. Small, superficial, low-grade lesions may be treated with organ-sparing options (wide local excision, glansectomy, laser or topical therapy for premalignant disease) to preserve length and function; larger or invasive tumours need partial or total penectomy with an adequate margin. The inguinal nodes are addressed according to risk: dynamic sentinel node biopsy or inguinal lymphadenectomy for node-positive or high-risk disease, with chemotherapy/radiotherapy in advanced cases. Throughout, the message is that prevention — hygiene and, where culturally appropriate, circumcision — and early biopsy of any suspicious lesion are what change outcomes.
Provided image
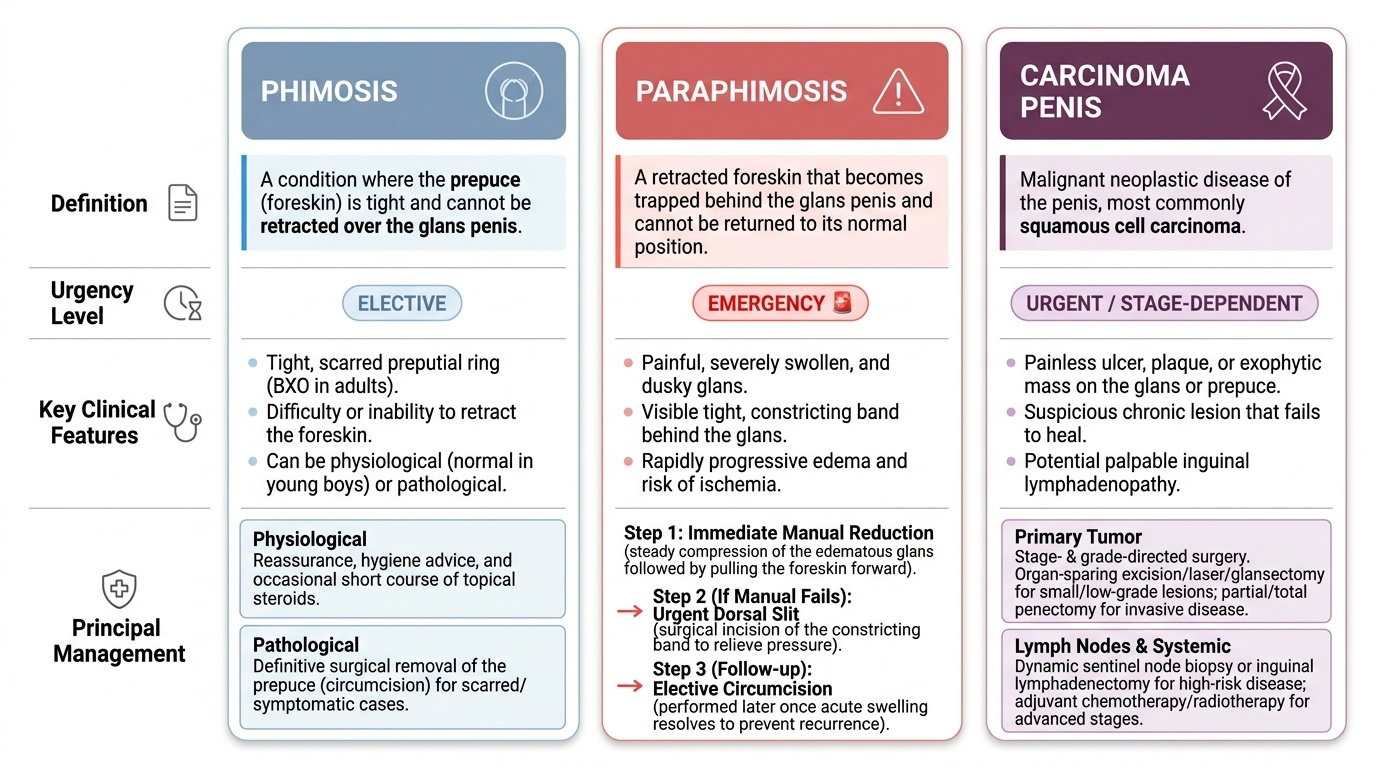
| Condition | Definition | Urgency | Key feature | Principal management |
|---|---|---|---|---|
| Phimosis | Non-retractile prepuce | Elective | Tight/scarred preputial ring (BXO in adults) | Reassurance/topical steroid (physiological); circumcision (pathological) |
| Paraphimosis | Retracted foreskin trapped behind glans | Emergency | Painful swollen dusky glans, constricting band | Immediate manual reduction; dorsal slit if it fails; later circumcision |
| Carcinoma penis | Squamous cell carcinoma of glans/prepuce | Urgent (cancer pathway) | Non-healing ulcer/fungating lesion ± inguinal nodes | Biopsy; organ-sparing or partial/total penectomy + inguinal node management |
CLINICAL PEARL
Never treat a non-healing ulcer or persistent warty lesion on the glans or prepuce as 'just an infection' and never let a tight phimotic foreskin hide it — retract or biopsy. A penile lesion that has not healed in a few weeks is carcinoma until a biopsy proves otherwise, and the single most important thing you can add to the examination is to palpate BOTH groins, because inguinal nodal status drives both prognosis and treatment. Equally, never confuse paraphimosis with phimosis: phimosis can wait for an elective clinic, but a paraphimosed, swelling, dusky glans needs reduction now.
Check Your Understanding
Bring the three patients from the hook back to mind and test whether the foreskin thread now ties them together. The four-year-old has physiological phimosis: a naturally non-retractile prepuce with a normal stream needs only reassurance and hygiene, and forcible retraction would do harm — so you can reason your way from 'non-retractile foreskin' to 'reassure and wait'. The 24-year-old has paraphimosis: a retracted foreskin trapped behind the glans, a constricting ring, and progressive painful oedema that you have learned can threaten the glans with ischaemia — so you can reason from 'trapped retracted foreskin' to 'reduce it now, dorsal slit if that fails, circumcise later'. The 62-year-old with a non-healing, bleeding, malodorous lesion who was never circumcised has carcinoma penis until biopsy says otherwise — so you can reason from 'non-healing penile ulcer in an uncircumcised man with chronic phimosis' to 'biopsy the lesion, examine both groins, and stage'. Use these threads to self-test the competency: can you define each of the three precisely; separate physiological from pathological phimosis; list the risk factors for penile carcinoma and explain why neonatal circumcision is protective; and state the immediate management of paraphimosis and the principles (biopsy, organ-sparing vs penectomy, inguinal node management) for carcinoma? The questions that follow check exactly these links.
SELF-CHECK
Which of the following is the strongest PROTECTIVE factor against carcinoma of the penis?
A. Smoking cessation in adulthood
B. Neonatal circumcision
C. Treatment of recurrent balanitis with antibiotics
D. Regular HPV testing
Reveal Answer
Answer: B. Neonatal circumcision
Neonatal circumcision virtually abolishes carcinoma penis and the disease is rare in populations circumcised at birth, because it removes the prepuce and prevents the chronic irritation from retained smegma, poor hygiene and phimosis that drive squamous cell carcinoma. The other measures are reasonable but far less protective; HPV (16/18) is a risk factor, not a protective screen.