Page 10 of 17
SU30.6 | Tumours of Testis — SDL Guide
Learning Objectives
- Describe the classification of testicular tumours, distinguishing germ-cell (seminoma vs non-seminomatous) from non-germ-cell tumours and lymphoma (SU30.6).
- Describe the clinical features and investigations of testicular tumours, including the tumour markers AFP, beta-hCG and LDH.
- Outline the principles of management, emphasising radical inguinal orchidectomy and the absolute avoidance of trans-scrotal biopsy.
INSTRUCTIONS
A firm, painless lump in the testis of a young man is, until proven otherwise, a cancer — and one of the great success stories of oncology, because even metastatic testicular germ-cell tumours are usually curable. This module classifies testicular tumours (overwhelmingly germ-cell: seminoma versus non-seminomatous), shows how the tumour markers AFP, beta-hCG and LDH both characterise the tumour and follow its treatment, and drills the two non-negotiable rules: a solid intratesticular mass is managed by radical INGUINAL orchidectomy, and the scrotum is never violated by a biopsy or a trans-scrotal approach because the testis drains to the para-aortic, not the inguinal, nodes.
References
- Bailey & Love's Short Practice of Surgery, The Testis and Scrotum / Urology (textbook)
- SRB's Manual of Surgery, Tumours of the Testis (textbook)
- Sabiston Textbook of Surgery, Urologic Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 27-year-old footballer comes to clinic embarrassed, having felt a hard lump in his right testicle while showering after a match. There is no real pain — perhaps a dull ache — and he has waited a fortnight hoping it would settle. On examination the lump is part of the testis itself: firm, craggy, you cannot get above it, and it does not transilluminate. He is otherwise fit and well. It would be easy to reassure a healthy young man with a painless lump, but the opposite instinct is the correct one: in a man of this age a solid intratesticular swelling is a germ-cell cancer until proven otherwise. The reassuring truth that sits beside that alarm is that, handled correctly, his disease is among the most curable of all solid tumours — provided no one takes a knife to his scrotum to 'biopsy' it first.
WHY THIS MATTERS
Testicular tumours matter out of all proportion to their frequency because they strike young men in their reproductive and most productive years and because the right pathway turns a frightening diagnosis into a highly curable one. The clinical lessons are sharp and examinable: recognise that a solid intratesticular mass is cancer until proven otherwise; understand the tumour markers (AFP, beta-hCG, LDH) well enough to interpret them — most pointedly that a raised AFP means the tumour is not a pure seminoma; and, above all, learn the rule that the diagnosis and first treatment is a radical inguinal orchidectomy, and that a trans-scrotal biopsy is forbidden because it can seed tumour and alter the lymphatic drainage on which staging and treatment depend. Add the duty to offer sperm banking before treatment, and the principle that even advanced disease is curable with platinum-based chemotherapy, and you have a topic that rewards precise knowledge with a genuinely life-saving impact.
RECALL
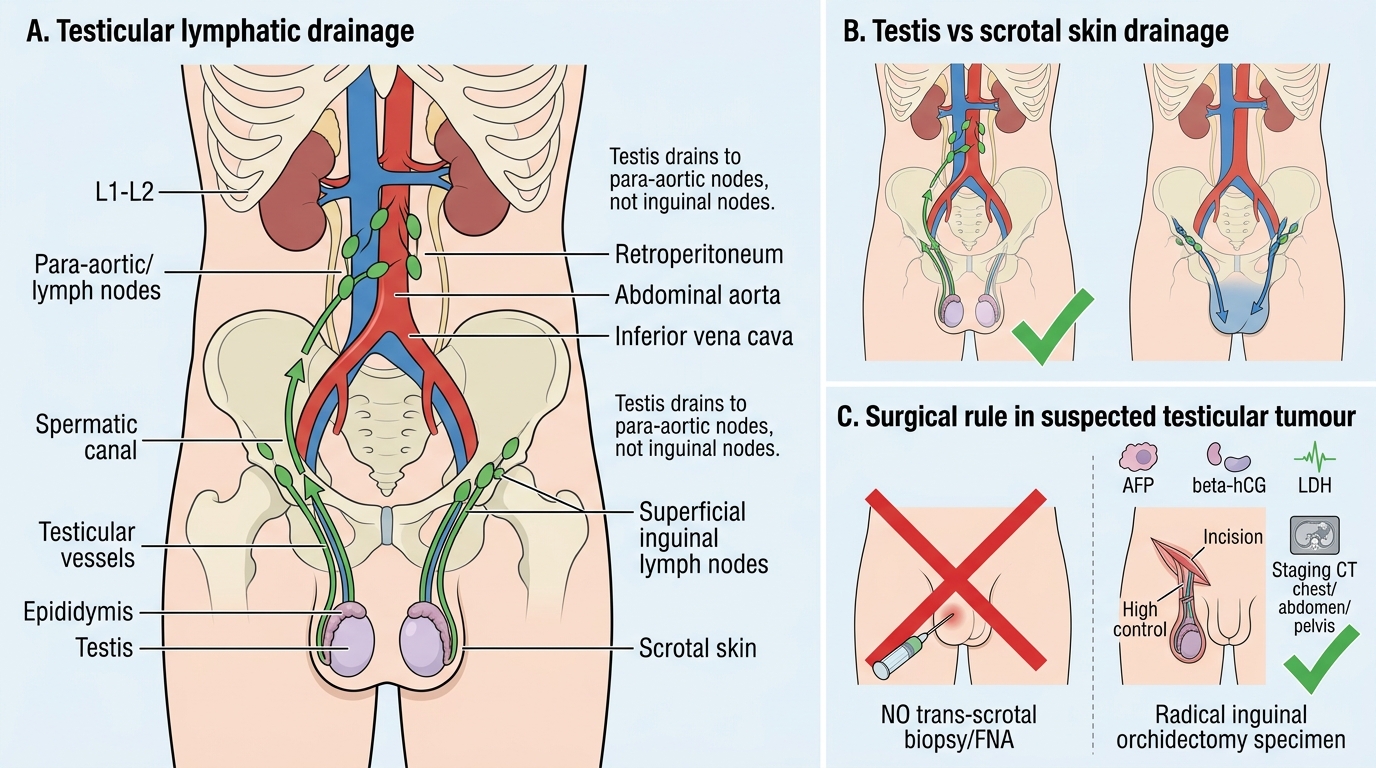
Recall two anatomical facts that govern everything about testicular cancer. First, the testis develops in the abdomen and descends to the scrotum, dragging its blood supply and, crucially, its lymphatic drainage with it — so the testis drains not to the nearby inguinal nodes but to the para-aortic (retroperitoneal) lymph nodes at the level of the renal vessels. This is why nodal disease presents as back pain or a retroperitoneal mass rather than a groin lump, and why staging imaging concentrates on the abdomen. Second, the scrotal skin has its own, separate lymphatic drainage to the inguinal nodes; violating the scrotum with a biopsy or a trans-scrotal incision can therefore spill tumour into a new lymphatic territory and worsen the prognosis. Hold on to one more link from earlier in this cluster: a history of an undescended testis (cryptorchidism) is a recognised risk factor for germ-cell tumours, tying SU30.2 to SU30.6.
The Young Man with a Testicular Lump
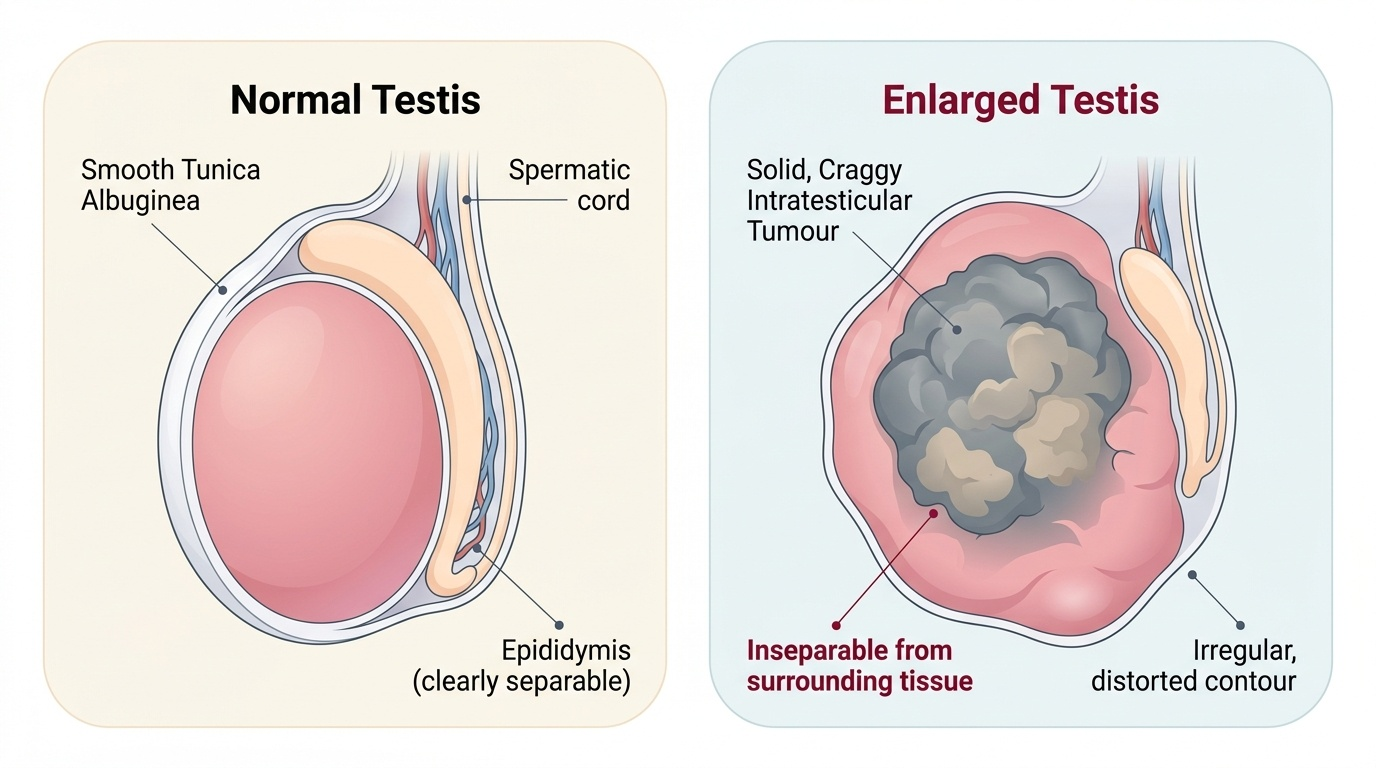
The classic presentation is a painless, firm or craggy swelling of the testis in a young man, typically between 15 and 35 years, often noticed by the patient himself or his partner, or drawn to attention by a minor injury that prompts examination rather than causing the lump. The swelling is part of the testis: on examination you cannot get above it, it does not transilluminate (it is solid, not fluid), and the normal testicular sensation is lost over the mass. A minority of men have a dull ache or heaviness; frank pain is uncommon and, if present, can mislead towards infection. Some patients present not with the primary lump but with the consequences of spread or hormone production: back pain or an abdominal mass from bulky para-aortic nodal disease, breathlessness from lung metastases, or gynaecomastia from beta-hCG-secreting tumours. A secondary hydrocele can accompany the tumour and occasionally obscures it — a reminder that the testis beneath any hydrocele must be assessed. The overriding clinical instinct must be that a solid intratesticular mass is a cancer until proven otherwise, however young and well the patient appears.
Provided image
- Painless, firm/craggy intratesticular lump in a man aged 15–35; cannot get above it; does not transilluminate.
- Less common presentations: dull ache/heaviness, back pain or abdominal mass (para-aortic nodes), gynaecomastia (beta-hCG), or a secondary hydrocele obscuring the lump.
- Rule: a solid intratesticular mass is cancer until proven otherwise.
Classification and Pathological Basis
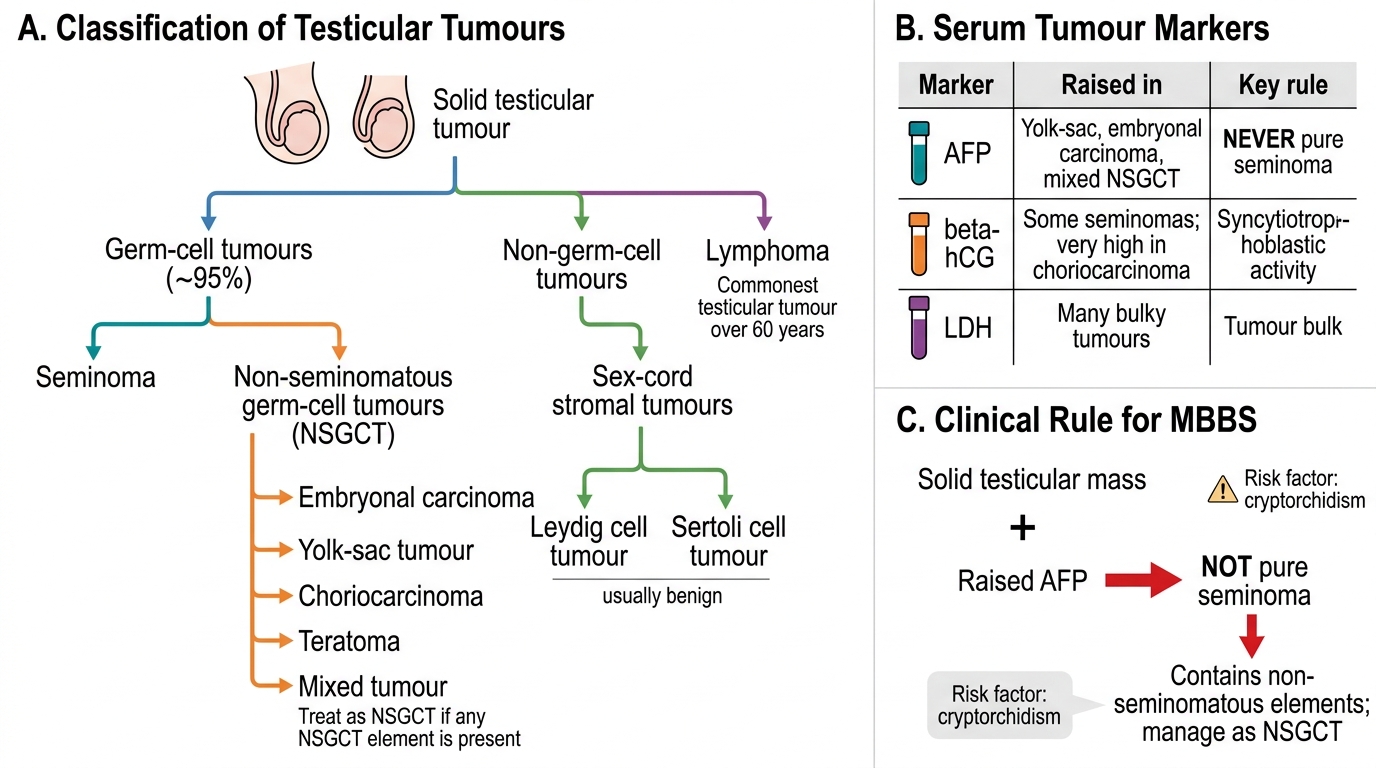
Classification is the backbone of this topic and directs both markers and treatment. The great majority of testicular tumours — about 95% — are germ-cell tumours (GCTs), which are divided into seminoma and non-seminomatous germ-cell tumours (NSGCT); the NSGCT group comprises embryonal carcinoma, yolk-sac tumour, choriocarcinoma, teratoma, and mixed germ-cell tumours (a tumour with any non-seminomatous element behaves as, and is treated as, NSGCT). A minority are non-germ-cell / sex-cord stromal tumours — Leydig cell and Sertoli cell tumours, mostly benign and occasionally hormone-secreting — and the testis is also a site of lymphoma, which is in fact the commonest testicular tumour in men over 60, an important age-related exception to the 'young man' rule. The main risk factor is a history of cryptorchidism (undescended testis), with a prior contralateral germ-cell tumour, a positive family history and infertility adding smaller increments of risk. The biology explains the tumour markers: alpha-fetoprotein (AFP) is produced by yolk-sac and embryonal elements and is therefore raised in NSGCT but is never raised by a pure seminoma — so a raised AFP proves the tumour is not pure seminoma; beta-human chorionic gonadotrophin (beta-hCG) is produced by trophoblastic (syncytiotrophoblast) tissue and may be modestly raised in some seminomas and is markedly elevated in choriocarcinoma; and lactate dehydrogenase (LDH) is a non-specific marker of tumour bulk used in staging and prognosis. Spread is to the para-aortic lymph nodes first (following the testicular lymphatics) and haematogenously to the lungs.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Classification and Markers of Testicular Tumours
- Germ-cell (~95%): seminoma vs NSGCT (embryonal carcinoma, yolk-sac, choriocarcinoma, teratoma, mixed).
- Non-germ-cell: sex-cord stromal (Leydig, Sertoli, usually benign); lymphoma is the commonest testicular tumour over 60.
- Markers: AFP (NSGCT — yolk-sac/embryonal; NEVER pure seminoma); beta-hCG (some seminomas; high in choriocarcinoma); LDH (tumour bulk). Risk factor: cryptorchidism.
SELF-CHECK
A young man with a solid testicular mass has a markedly raised serum AFP. What does this tell you about the tumour?
A. It confirms a pure seminoma
B. It indicates the tumour is NOT a pure seminoma (it contains non-seminomatous elements)
C. It indicates a Leydig cell tumour
D. It rules out malignancy
Reveal Answer
Answer: B. It indicates the tumour is NOT a pure seminoma (it contains non-seminomatous elements)
AFP is produced by yolk-sac and embryonal (non-seminomatous) elements and is NEVER raised by a pure seminoma. A raised AFP therefore means the tumour is not pure seminoma — it contains non-seminomatous germ-cell elements and is managed as an NSGCT. beta-hCG, by contrast, may be modestly raised in some seminomas; LDH reflects tumour bulk.
Examination and Investigation
Examination and investigation follow a fixed sequence designed around the cardinal rule that the diagnosis is made on the orchidectomy specimen, not on a needle. Examine the scrotal contents to confirm the mass is intratesticular (you cannot get above it; it does not transilluminate; the testis is hard or replaced), then examine the abdomen for a retroperitoneal/para-aortic mass, the supraclavicular nodes, the chest (effusion, metastases) and the breasts (gynaecomastia). The first imaging test is a scrotal ultrasound, which reliably confirms a solid intratesticular lesion and distinguishes it from benign extratesticular swellings. Serum tumour markers — AFP, beta-hCG and LDH — must be measured before orchidectomy (they aid diagnosis and provide a baseline) and again afterwards (their fall, against their known half-lives, monitors the adequacy of treatment and detects residual or recurrent disease). Once the diagnosis is suspected, staging is by CT of the chest, abdomen and pelvis to assess the para-aortic nodes and the lungs. The non-negotiable point is the route to tissue diagnosis: never perform a trans-scrotal biopsy or fine-needle aspiration and never approach the tumour through the scrotum, because breaching the scrotum can seed tumour and divert lymphatic drainage to the inguinal nodes, worsening the prognosis — the testis is removed and examined whole, through the groin.
Testicular Lymphatic Drainage and Surgical Approach
- Examination: confirm intratesticular (no get-above-it, no transillumination); examine abdomen/nodes/chest/breasts.
- Investigations: scrotal ultrasound (first-line imaging); tumour markers (AFP/beta-hCG/LDH) BEFORE and after orchidectomy; CT chest/abdomen/pelvis for staging.
- Absolute rule: NO trans-scrotal biopsy/FNA — diagnosis is on the radical inguinal orchidectomy specimen.