Page 5 of 17
SU30.2 | Undescended Testis — SDL Guide (Part 2)
Principles of Management
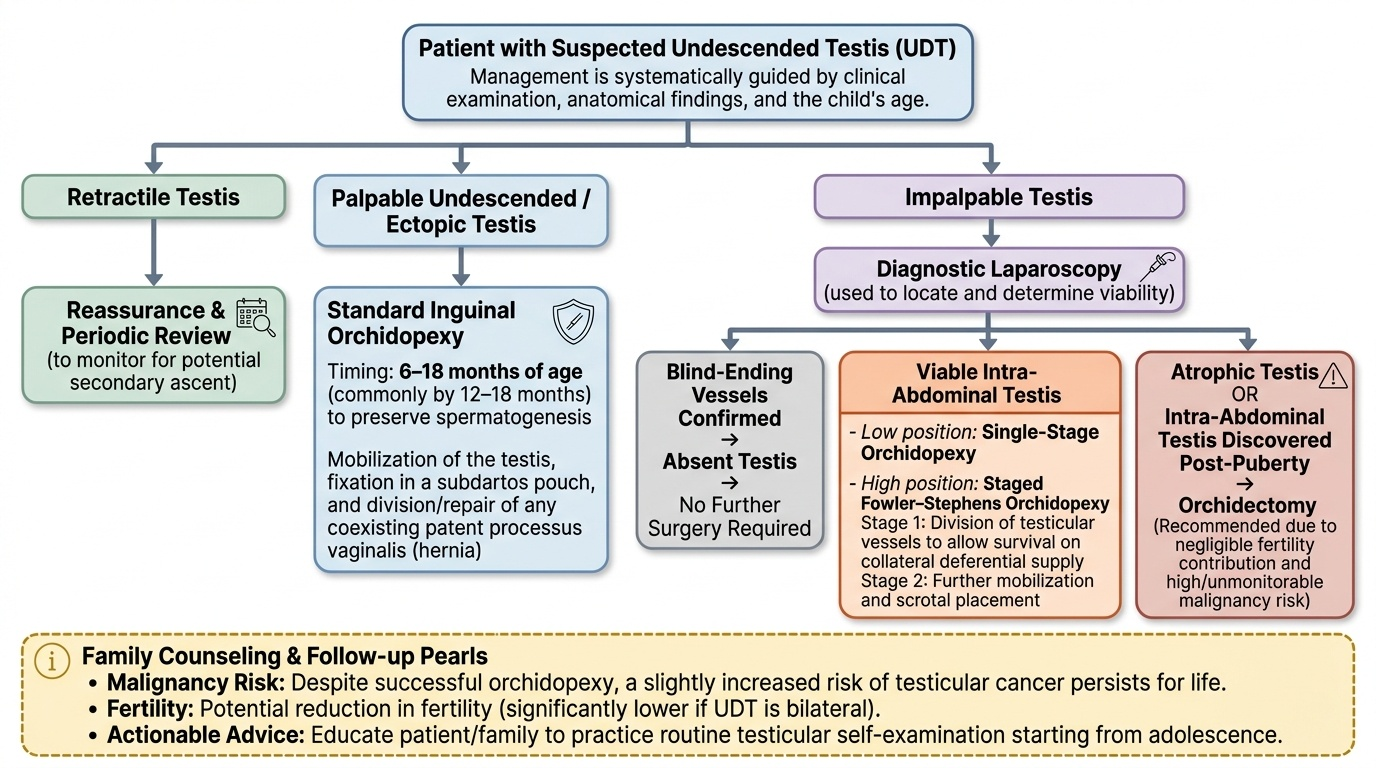
Management is guided by the diagnosis and the child's age, and the central operation is orchidopexy — mobilising the testis and fixing it in a subdartos pouch in the scrotum, with division of any associated patent processus vaginalis (hernia). Timing matters: because the harm accrues with time and most testes that will descend do so within the first few months, orchidopexy is recommended between about 6 and 18 months of age (commonly by 12–18 months), early enough to give the best chance of preserving spermatogenesis and to allow future surveillance. For the palpable undescended or ectopic testis, a standard inguinal orchidopexy is performed. For the impalpable testis, diagnostic laparoscopy both locates and treats: a viable intra-abdominal testis can be brought down, sometimes as a staged Fowler–Stephens orchidopexy (dividing the testicular vessels in a first stage so the testis survives on the deferential collateral supply and is mobilised further at a second stage); blind-ending vessels confirm an absent testis needing no further surgery. An atrophic testis or one discovered after puberty in an intra-abdominal position is usually managed by orchidectomy, because such a testis contributes little to fertility and carries a malignancy risk that is hard to monitor in that location. The retractile testis needs only reassurance and periodic review (to detect the small number that later ascend). Whatever the path, counsel the family clearly that the man will carry a slightly increased risk of testicular cancer for life despite surgery, that fertility may be reduced (especially if bilateral), and that he should learn and practise testicular self-examination from adolescence.
Provided image
- Orchidopexy at ~6–18 months (by 12–18 months) for the palpable undescended/ectopic testis; repair any coexisting hernia.
- Impalpable: diagnostic laparoscopy → orchidopexy (staged Fowler–Stephens if high) or orchidectomy for an atrophic/post-pubertal intra-abdominal testis.
- Counsel: malignancy risk persists after orchidopexy, possible subfertility (worse if bilateral), lifelong self-examination; retractile testis = reassure + review.
CLINICAL PEARL
Orchidopexy repositions the testis and lets you and the patient watch it — it does NOT cancel the increased risk of testicular cancer, so every man with a history of an undescended testis must learn lifelong self-examination. And before labelling any boy 'undescended', prove it is not a retractile testis: a normal testis that you can coax into the scrotum and that stays there is a variant that needs only reassurance. Do not order an ultrasound to 'find' an impalpable testis — a negative scan does not exclude an intra-abdominal testis, and diagnostic laparoscopy is the definitive step.
Check Your Understanding
Return to the two children from the hook and test whether the reasoning now flows. The six-week-old baby with a flat, empty hemiscrotum has a genuinely undescended testis: you would examine carefully to decide whether it is palpable or impalpable, give spontaneous descent a few months but plan orchidopexy by 12–18 months, and counsel the parents about future fertility, the malignancy risk that persists after surgery, and self-examination — reasoning from 'empty scrotum that does not coax down' to 'plan timed surgery and lifelong follow-up'. The three-year-old whose testis you drew into the scrotum, where it stayed until the reflex provoked it, has a retractile testis: reasoning from 'coaxes down and stays' to 'reassure and review', with no operation needed. Now self-test the competency directly. Can you describe the applied anatomy of descent and name the common sites of arrest and ectopia? Can you separate undescended from retractile and ectopic testes on examination, and palpable from impalpable? Can you justify why ultrasound is unhelpful and diagnostic laparoscopy definitive for the impalpable testis? And can you state the timing and principles of orchidopexy, the role of Fowler–Stephens and orchidectomy, and the counselling on fertility and persisting cancer risk? The questions that follow check these links.
SELF-CHECK
Which statement about the malignancy risk in undescended testis is correct?
A. Orchidopexy completely removes the increased risk of testicular cancer
B. The increased risk of testicular malignancy persists even after orchidopexy
C. There is no increased risk of malignancy in cryptorchidism
D. The risk is eliminated only if orchidopexy is done after puberty
Reveal Answer
Answer: B. The increased risk of testicular malignancy persists even after orchidopexy
An undescended testis carries an increased risk of germ-cell malignancy, and this risk persists even after the testis is brought down — orchidopexy corrects position and, importantly, allows the testis to be examined and watched, but it does not abolish the cancer risk. This is why lifelong testicular self-examination is counselled. Late surgery does not reduce risk; earlier surgery is preferred for fertility and surveillance.