Page 2 of 11
SU3.1 | Blood Products and Transfusion Complications — SDL Guide (Part 2)
Recognising and Managing Transfusion Complications
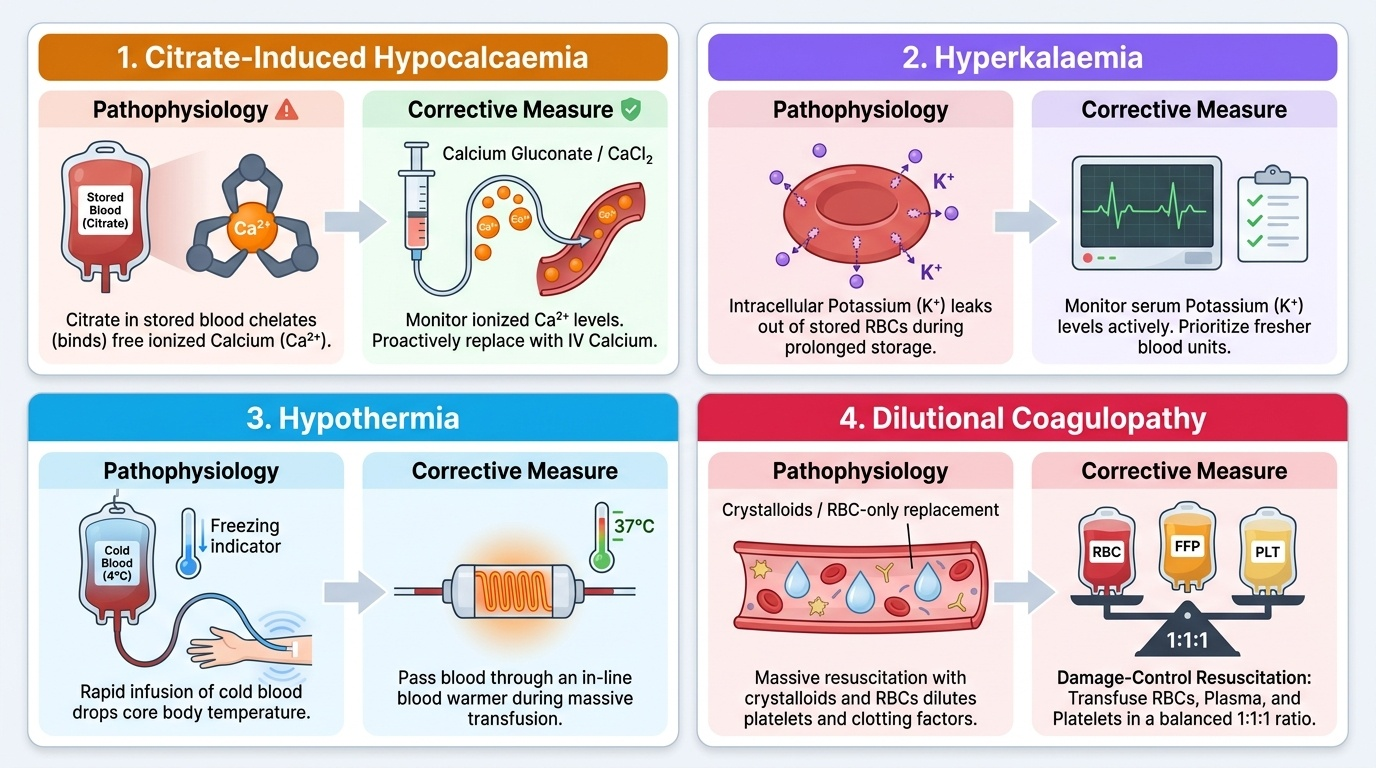
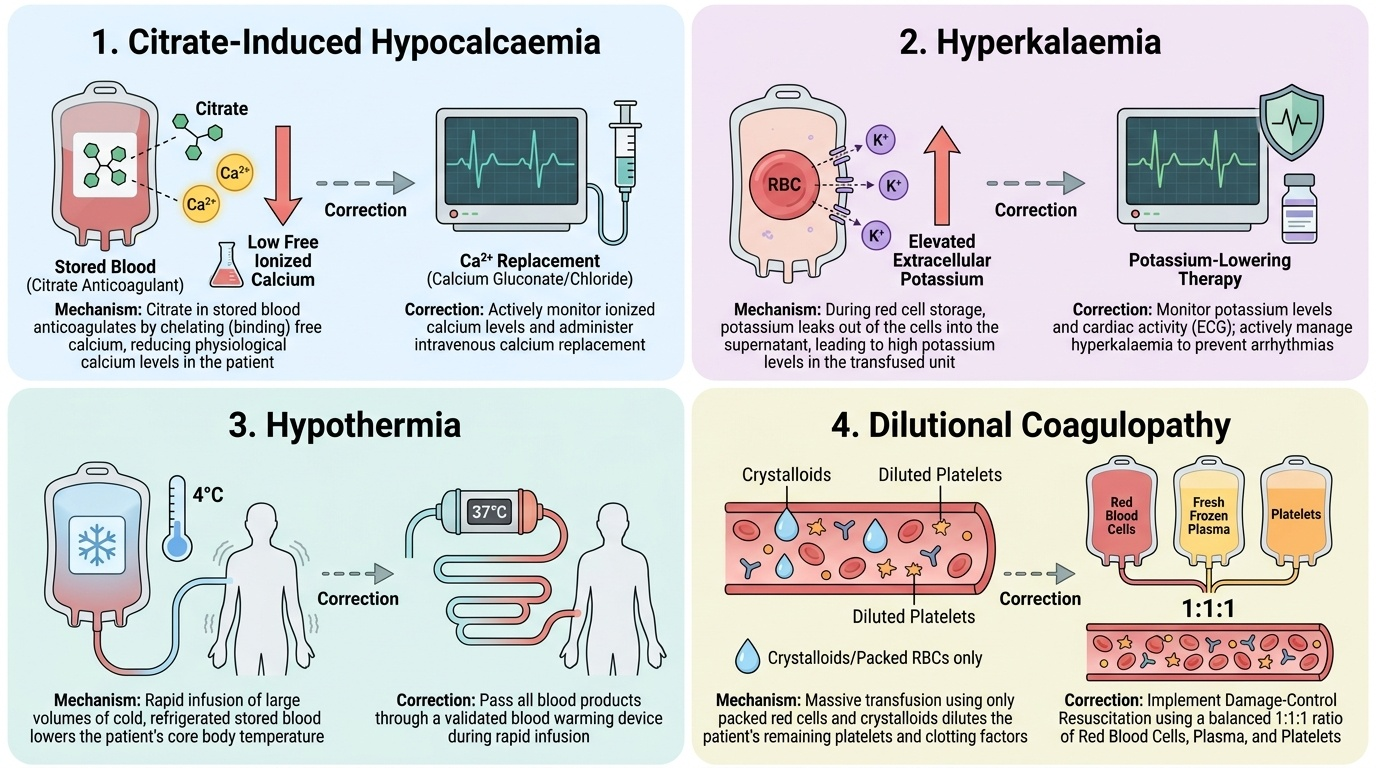
Recognising a reaction depends on its timing and features, because management hinges on telling a dangerous reaction from a benign one. An acute haemolytic reaction declares itself within minutes with fever, loin/back pain, burning at the drip site, hypotension, haemoglobinuria and the threat of DIC and renal failure; the response is to stop the transfusion immediately, maintain the airway and circulation with intravenous fluids, return the unit and a fresh sample to the laboratory, and support the kidneys and clotting — this is an emergency. An FNHTR causes fever and rigors during or soon after transfusion without haemolysis; the transfusion is paused, other causes excluded, and an antipyretic given, with future leucodepleted units to prevent recurrence. Allergic reactions range from urticaria, managed by slowing the transfusion and giving an antihistamine, to anaphylaxis with bronchospasm and shock, which requires the transfusion stopped and adrenaline given. TRALI presents as acute hypoxia and bilateral pulmonary infiltrates within six hours and is treated as acute respiratory distress with respiratory support, and it must be distinguished from TACO, whose breathlessness comes from circulatory overload and responds to slowing or stopping the transfusion and giving a diuretic. Bacterial contamination causes rapid high fever, rigors and septic shock and demands the transfusion be stopped with cultures taken and broad-spectrum antibiotics started. A delayed haemolytic reaction appears days later as an unexplained fall in haemoglobin, jaundice and a positive direct antiglobulin test, and is usually managed supportively. Finally, the metabolic complications of massive transfusion must be actively prevented and corrected: stored blood is anticoagulated with citrate, which chelates calcium and causes hypocalcaemia; potassium leaks from stored red cells causing hyperkalaemia; cold blood causes hypothermia; and replacing lost blood with red cells and crystalloid dilutes platelets and clotting factors, causing a dilutional coagulopathy — which is why damage-control resuscitation gives red cells, plasma and platelets together in a balanced ratio of approximately 1:1:1, warms the blood, and monitors and replaces ionised calcium. Underpinning all of this is prevention: correct ABO and Rh grouping, a valid crossmatch, and the bedside identity check that ensures the right unit reaches the right patient.
Provided image
Provided image
| Reaction | Mechanism | Typical timing | Key features & first action |
|---|---|---|---|
| Acute haemolytic | ABO incompatibility, IgM, intravascular haemolysis | Minutes | Fever, loin pain, haemoglobinuria, shock, DIC — STOP, resuscitate, support kidneys |
| Febrile non-haemolytic | Anti-leucocyte antibody / cytokines | During/soon after | Fever, rigors, no haemolysis — pause, antipyretic, leucodeplete future units |
| Allergic / anaphylactic | Antibody to donor plasma proteins | Minutes | Urticaria → bronchospasm/shock — antihistamine; adrenaline if anaphylaxis |
| TRALI | Donor anti-leucocyte antibodies activate lung neutrophils | < 6 hours | Acute hypoxia, bilateral infiltrates, non-cardiogenic oedema — respiratory support |
| TACO | Hydrostatic circulatory overload | During/after | Breathlessness, raised JVP, hypertension — slow/stop, diuretic |
| Delayed haemolytic | Anamnestic IgG to minor antigen, extravascular | Days later | Unexplained Hb fall, jaundice, positive DAT — supportive |
| Bacterial contamination | Endotoxin / sepsis | Minutes–hours | High fever, rigors, septic shock — STOP, cultures, antibiotics |
Check Your Understanding
Consolidate this module by reasoning through it rather than memorising lists. Return to the bleeding obstetric patient from the start: she received a unit of red cells and within minutes developed fever, loin pain, hypotension and red-wine urine. Trace the mechanism — incompatible donor cells, recipient IgM anti-A/anti-B, complement, intravascular haemolysis, haemoglobinuria — and you arrive at an acute haemolytic reaction whose first action is always to stop the transfusion and resuscitate; you also realise it was a preventable identification error. Now test three links. First, match product to deficit: which component would you reach for in isolated thrombocytopenia, in a low fibrinogen, in multiple-factor coagulopathy, and in symptomatic anaemia — and recall how each is stored. Second, match reaction to mechanism and timing: place fever-with-haemoglobinuria, fever-without-haemolysis, urticaria, hypoxia-within-six-hours, breathlessness-with-overload, and a fall in haemoglobin days later into their correct categories. Third, reason through the massively transfused trauma patient: name the four metabolic complications, link each to its cause (citrate→hypocalcaemia, leaked potassium→hyperkalaemia, cold blood→hypothermia, dilution→coagulopathy), and justify warming the blood, giving balanced ratios and watching the ionised calcium. If you can do these three things you have met the competency.
CLINICAL PEARL
The first 15 minutes are everything. The most dangerous reactions — acute haemolytic, severe allergic/anaphylactic and bacterial sepsis — declare themselves early, so a transfusion must be started slowly and watched closely from the very first drops. And remember the single most important safety rule: the commonest cause of a fatal haemolytic reaction is not exotic immunology but a clerical error — the wrong unit given to the wrong patient. No laboratory crossmatch can rescue a failed bedside identity check, so the patient-to-unit verification at the bedside is the final and most important barrier.
SELF-CHECK
Two hours into a unit of packed red cells an elderly patient with poor cardiac reserve becomes acutely breathless with a raised jugular venous pressure and hypertension, but no fever, rash or haemoglobinuria. Which complication is most likely and what is the immediate action?
A. TRALI — give adrenaline
B. Transfusion-associated circulatory overload (TACO) — slow or stop the transfusion and give a diuretic
C. Acute haemolytic reaction — return the unit for regrouping
D. Febrile non-haemolytic reaction — give an antipyretic
Reveal Answer
Answer: B. Transfusion-associated circulatory overload (TACO) — slow or stop the transfusion and give a diuretic
Breathlessness with a raised JVP and hypertension in a patient with limited cardiac reserve, without fever or haemolysis, is transfusion-associated circulatory overload (TACO) — hydrostatic volume overload. The immediate action is to slow or stop the transfusion, sit the patient up and give a diuretic. TRALI causes non-cardiogenic oedema (normal/low filling pressures) within six hours; an acute haemolytic reaction would show fever, loin pain and haemoglobinuria; an FNHTR is defined by fever.