Page 7 of 14
SU9.3 | Communicating Investigation Results — SDL Guide
Learning Objectives
- Communicate routine and serious surgical investigation results clearly, using plain language and checking the patient's understanding (SU9.3).
- Apply the SPIKES protocol to break bad news such as a cancer diagnosis in a structured, empathic way (SU9.3).
- Counsel a patient on the implications of a result and the next steps, including further investigation, multidisciplinary review and support (SU9.3).
INSTRUCTIONS
How a result is communicated can matter as much to a patient as the result itself. A diagnosis delivered clumsily — in jargon, without warning, without empathy — causes lasting harm, while the same news delivered with structure and compassion preserves trust and helps the patient cope and decide. This module treats communicating results as the clinical skill it is: you will learn the principles of clear, patient-centred result-giving, the widely used SPIKES protocol for breaking bad news, how to read and respond to a patient's reaction, and how to counsel on next steps. You will practise these in simulated consultations before you ever deliver real results to real patients.
References
- Bailey & Love's Short Practice of Surgery, Communication and the Surgical Patient (textbook)
- Baile WF et al. SPIKES — A Six-Step Protocol for Delivering Bad News. The Oncologist, 2000 (journal)
- AETCOM Module (NMC) — Doctor-Patient Communication and Breaking Bad News (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A young man waits for the result of a biopsy. The surgeon, hurrying between clinics, leans into the doorway and says, 'The histology's back — it's a carcinoma, we'll need to talk about chemo,' and is gone before the word has even registered. The patient remembers nothing else from that day except the corridor and the word 'carcinoma'; he hears none of the plan, none of the hope, and carries the memory of how he was told for the rest of his life. Now imagine the same news given in a quiet room, with a warning that it is serious, in plain words, with a pause for the shock, an acknowledgement of fear, and a clear next step. The diagnosis is identical; the experience — and the trust, the understanding, the ability to decide — could not be more different. Communicating a result is not an afterthought to investigation; it is a clinical skill that shapes everything that follows.
WHY THIS MATTERS
Every investigation you order ends in a conversation, and you will have these conversations many times a week for the rest of your career — explaining a reassuring scan, a worrying blood test, or a diagnosis of cancer. Done well, clear and empathic communication improves the patient's understanding, their trust in you, their adherence to treatment and their ability to make decisions; done badly, it causes distress, confusion, complaints and harm. This is an examined AETCOM competency, assessed at the shows-how level — meaning you must be able to demonstrate it, not merely describe it — and it underpins informed consent, shared decision-making and the whole surgical-oncology pathway. You cannot counsel a patient about an operation, a cancer or a screening result without first being able to convey that result humanely and check that it has been understood. Because the skill is learnable and the stakes are high, you will rehearse it deliberately in simulation, building the structure and the habits that let you communicate well even under the emotional pressure of real bad news.
RECALL
Recall what you bring to this skill from earlier learning. From AETCOM and professionalism, recall the principles of the doctor-patient relationship — respect, honesty, confidentiality and informed consent — and that results are the patient's information, to be shared with them clearly and disclosed to others only with consent or in the patient's interest. From the investigations SDL (SU9.1), recall that a result is interpreted in context and as a trend, so that what you communicate is a considered conclusion, not a raw number out of context. From the early-detection SDL (SU9.2), recall that a cancer diagnosis triggers a multidisciplinary pathway, so counselling about a serious result naturally leads into next steps and team review. These foundations — ethical communication, considered interpretation, and the onward pathway — are what good result communication is built on.
Why Communicating Results Is a Clinical Skill
The indication for deliberate, skilled communication is every result that reaches a patient — not only the dramatic ones. Communication is a clinical skill in exactly the same sense as suturing or interpreting a scan: it is learnable, it can be done well or badly, it is examined, and its quality directly affects patient outcomes. The evidence is consistent that patient-centred communication — communication that explores the patient's concerns, gives information clearly and responds to emotion — improves understanding, recall, satisfaction, trust and adherence, and reduces anxiety and complaints. The converse is also true: news delivered in jargon, without warning or empathy, is poorly understood, badly remembered and damaging to the relationship, and is a frequent source of complaints and litigation even when the underlying care was sound. Crucially, the way news is delivered is largely independent of the news itself — a serious diagnosis can be delivered well or badly, and the patient's lasting impression often turns on the manner more than the content. Because this skill must be performed under emotional pressure, it benefits enormously from a structure to fall back on, which is why protocols such as SPIKES exist and why the skill is rehearsed in simulation. The remainder of this module sets out the general principles of good result-giving, the SPIKES protocol for the hardest conversations, how to read and respond to the patient in front of you, and how to counsel on next steps — the whole arc from result to agreed plan.
Principles of Good Result Communication
Whatever the result, a set of governing principles makes communication safe and effective, and these apply before any specific protocol. First, protect confidentiality and consent: confirm you are speaking to the right person, in a private setting, and disclose results to relatives or others only with the patient's consent or where it is clearly in their interest. Second, use plain language: replace jargon with words the patient understands ('a cancer' rather than 'a malignant neoplasm'), give information in small chunks, and avoid burying the message in detail. Third, be patient-centred: begin by finding out what the patient already knows and wants to know, follow their pace, and address the questions that matter to them rather than only the ones you find interesting. Fourth, be honest and clear without being brutal — do not give false reassurance, but do not strip away hope or overwhelm with worst-case detail unasked. Fifth, check understanding actively using a teach-back approach: ask the patient to tell you, in their own words, what they have understood, and correct gently — this catches the common situation where a patient nods but has grasped little. Sixth, respond to emotion before moving to problem-solving; a frightened or shocked patient cannot absorb a management plan. Finally, document what was discussed and arrange follow-up and support, because one conversation is rarely enough. These principles hold for a reassuring result and a devastating one alike; the SPIKES protocol simply organises them for the situation where the news is bad.
- Confidentiality & consent — right person, private setting, disclose to others only with consent.
- Plain language, small chunks — no jargon; do not bury the message.
- Patient-centred — start from what they know and want; follow their pace.
- Honest, not brutal — no false reassurance, no unasked worst-case flood.
- Check understanding (teach-back) — ask them to restate it.
- Respond to emotion first, then plan; document and arrange follow-up.
The SPIKES Protocol for Breaking Bad News
When the result is serious — a cancer diagnosis, an inoperable finding, a poor prognosis — a recognised structure prevents the conversation from going wrong under pressure. The most widely taught is the SPIKES protocol (Baile and colleagues, 2000), a six-step sequence whose initials name the steps. S — Setting up: prepare. Choose a quiet, private place, sit down, allow enough time, silence interruptions, and offer to have a relative or supporter present. P — Perception: before telling, ask — find out what the patient already understands about their condition and the tests ('What have you been told so far?'), so you can pitch the news correctly and correct misconceptions. I — Invitation: ask how much the patient wants to know; most want full information, but some prefer that details go to a relative, and their wishes must be respected. K — Knowledge: give the information. Begin with a warning shot ('I'm afraid the results are more serious than we hoped'), then deliver the news in small chunks of plain language, pausing frequently, avoiding jargon and bluntness alike, and checking understanding as you go. E — Emotions: respond to the patient's emotional reaction with empathy — name the emotion you observe, acknowledge it, allow silence, and do not rush to fix it; this is often the most important step and the one most easily skipped. S — Strategy and Summary: once the patient is ready, agree a clear plan and next steps — further investigations, the multidisciplinary review, treatment options and support — summarise, check understanding again, and ensure the patient leaves knowing what happens next and whom to contact. Used in order, SPIKES turns a dreaded encounter into a humane, structured conversation, and it is the reference protocol you will be expected to demonstrate.
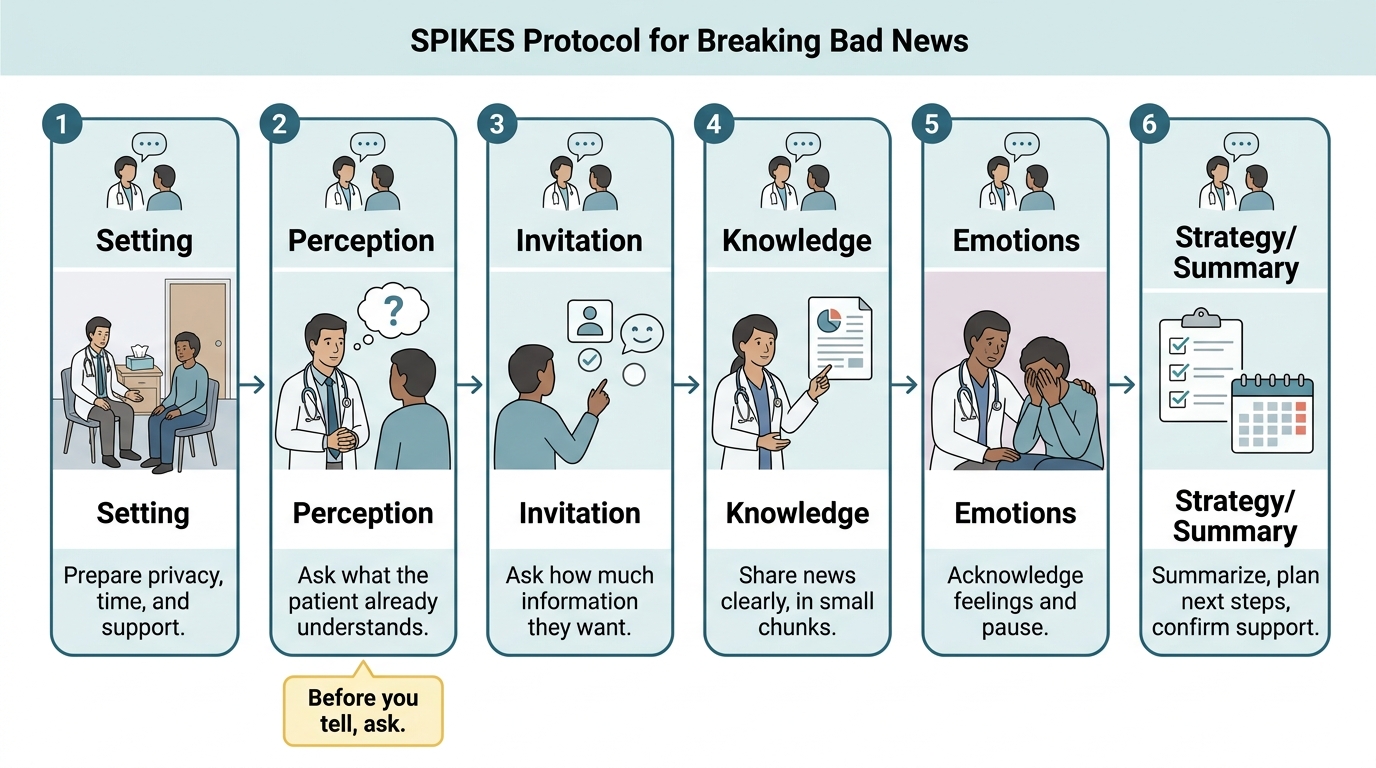
Six-Step SPIKES Protocol for Breaking Bad News
SELF-CHECK
In the SPIKES protocol, what does the 'P' (Perception) step require you to do BEFORE you tell the patient the diagnosis?
A. Prescribe medication for anxiety
B. Ask what the patient already understands about their condition, so you can pitch the news appropriately
C. Give the full pathology report in technical detail
D. Phone the patient's relatives to tell them first
Reveal Answer
Answer: B. Ask what the patient already understands about their condition, so you can pitch the news appropriately
Perception is the 'before you tell, ask' step: you find out what the patient already knows and believes about their illness and tests, so you can match your explanation to their starting point and correct any misconceptions. It is not about prescribing, dumping technical detail, or informing relatives before the patient (which would breach confidentiality).